
,%204x13,%204.5x4(3).jpg)
|
|
|
|
|
|
|
|
|
|
Short Clinical Crown Height
The buccal gingival margin of the residual root at #4 is coronally migrated (Fig.1). The clinical crown height is expected to be short. After wound heals, the abutment mentioned below will be changed to the one with shorter cuff (2 mm for example) with preparation if needed. The margin of the provisional will be fabricated subgingival and bulging so that the gingival margin will be gradually migrated apically.
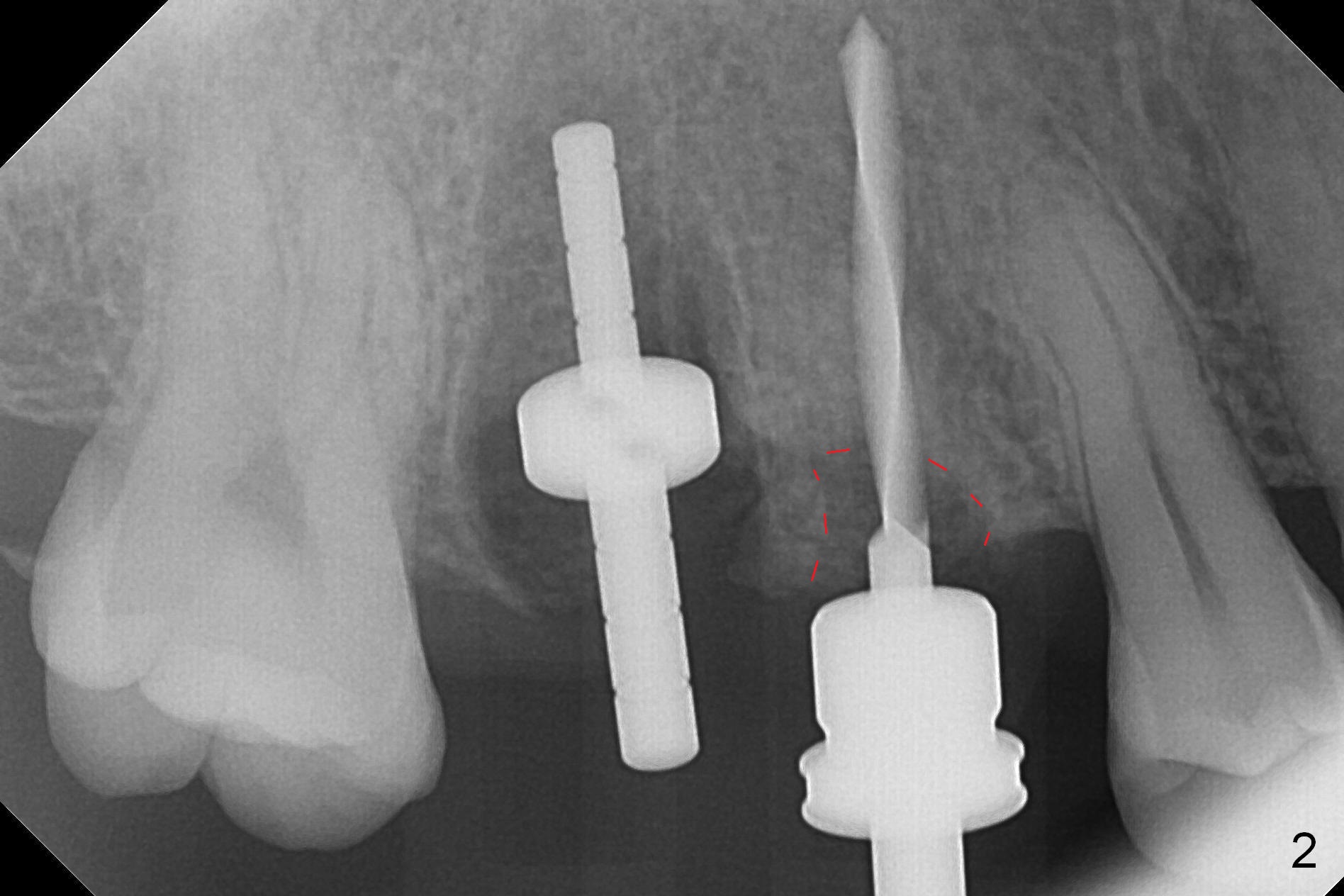
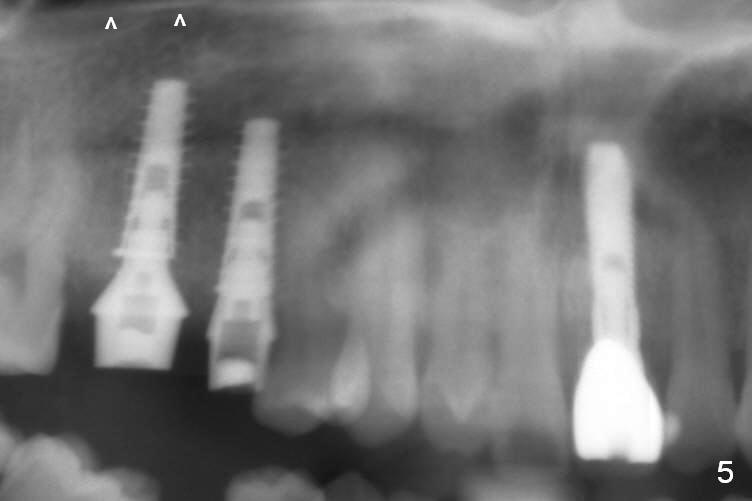
After extraction, osteotomy is established in the septum of #3 and the mesial slope of the shallow socket of #4 (Fig.2 red dashed line) for 11 and 13 mm deep, respectively. Since the septum is sloped palatally, a series of Magic Drills (MD) are used. A single large MD may wobble in the slope. By the time MD 3.8 mm is used, there is perforation palatally. The insertion torque of 4.5x13 mm IBS implant is less than 30 Ncm (Fig.3). In retrospectively, the osteotomy should have been initiated more buccally or deeper, since there is fair amount of clearance from the sinus floor (Fig.5 ^). The implant at #9 is 3.8x16 mm.
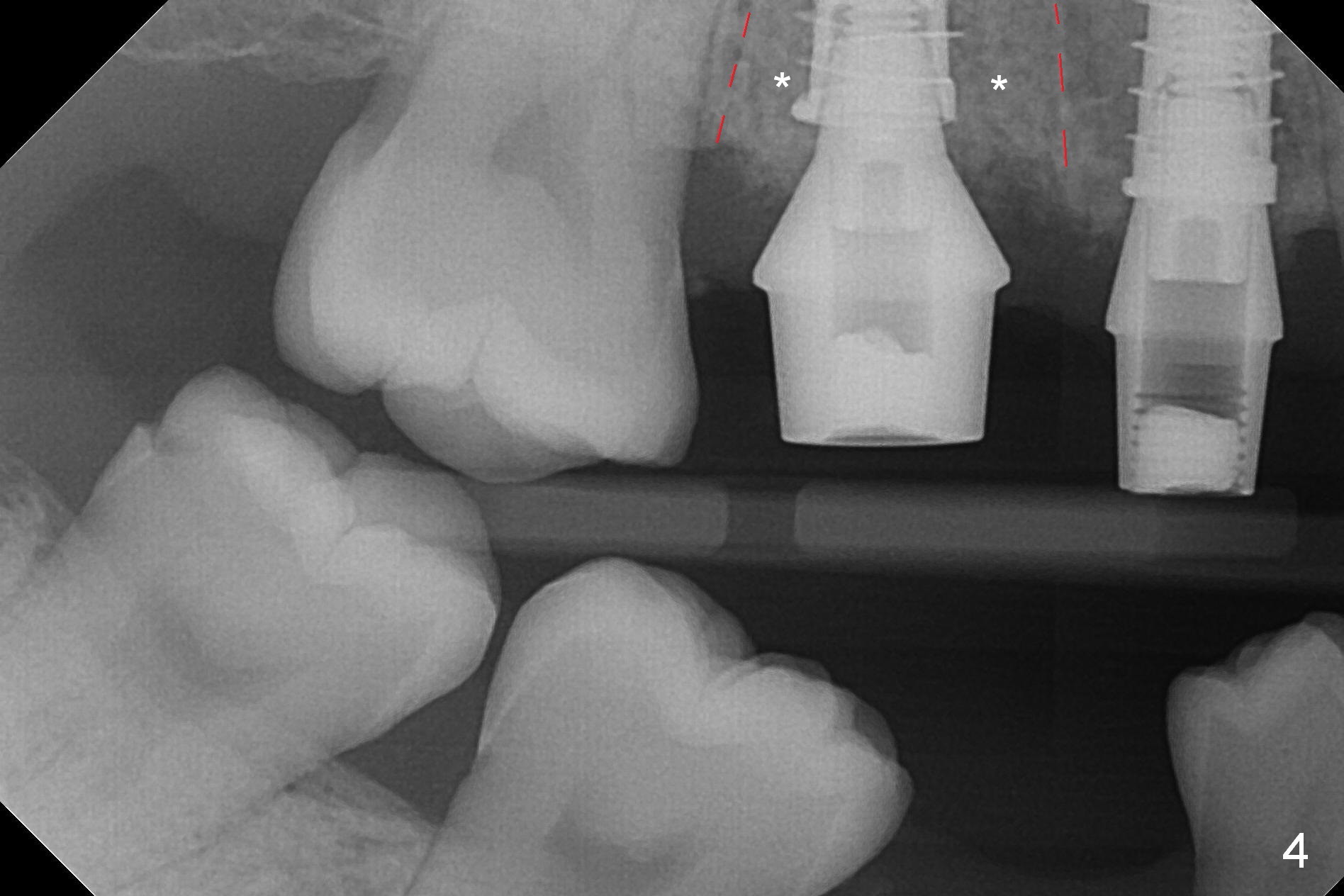
In contrast, osteotomy at #4 is finished with a single MD 3.3 mm. A 4x13 mm implant is placed with more than 50 Ncm. Pair abutments are immediately placed (6.5x4(3) and 4.5x4(3) mm) for splinted immediate provisional. The remaining socket (Fig.4 red dashed line) is filled with mixture of allograft, autogenous bone and Osteogen (*).
Return to
Upper Premolar,
Molar
Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
Xin Wei, DDS, PhD, MS 1st edition 02/09/2017, last revision 02/10/2017