,%204x11.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Less is More
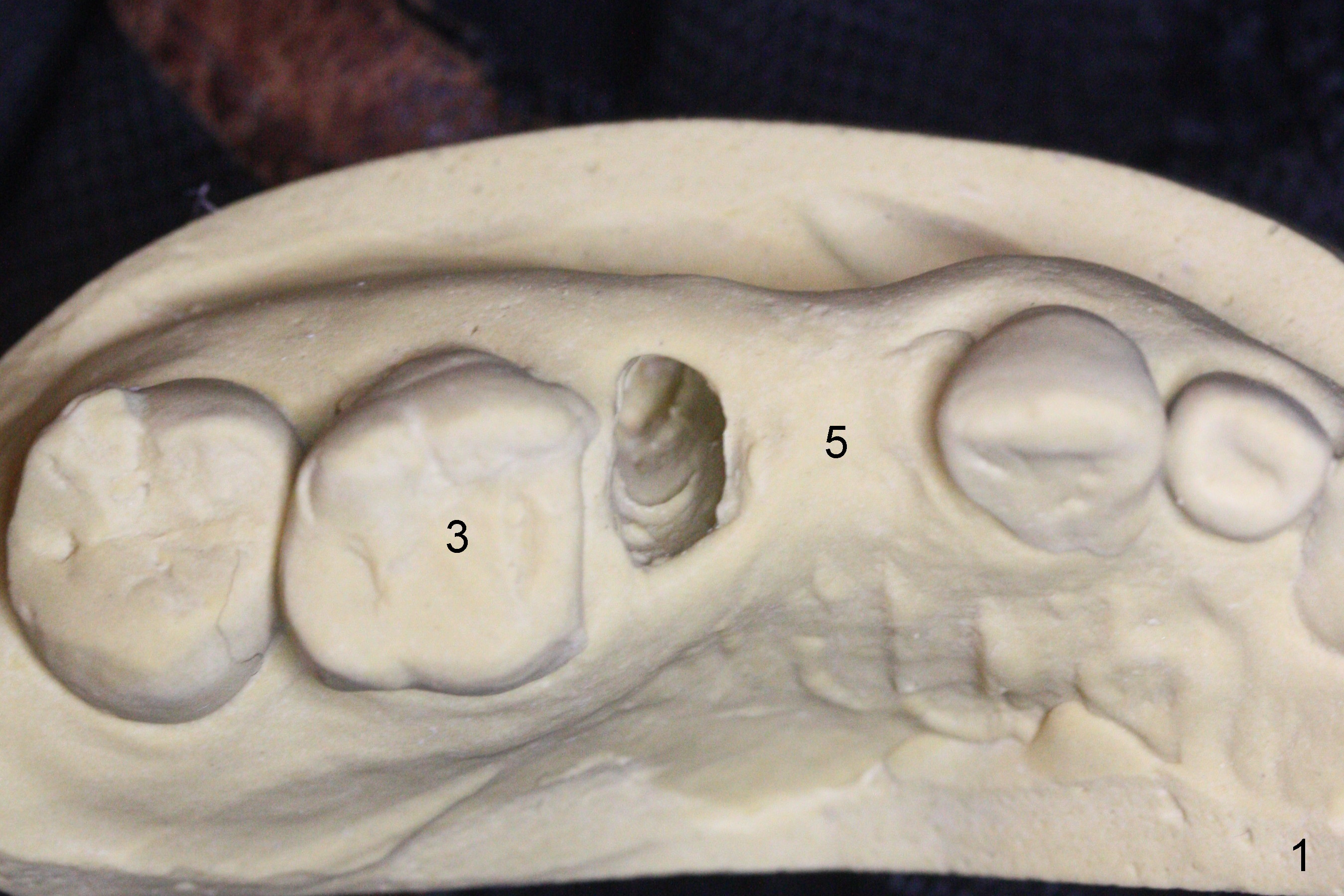
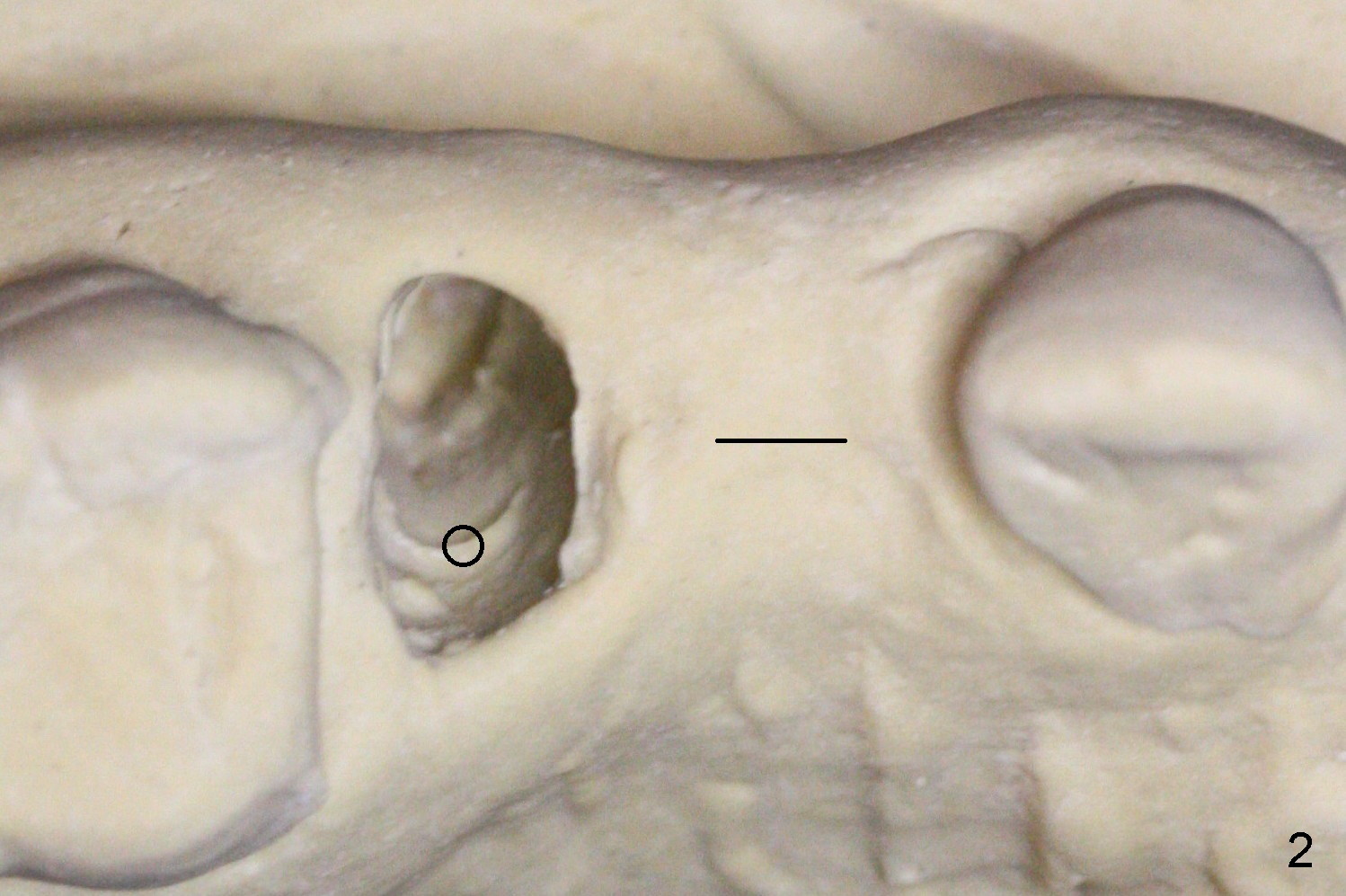
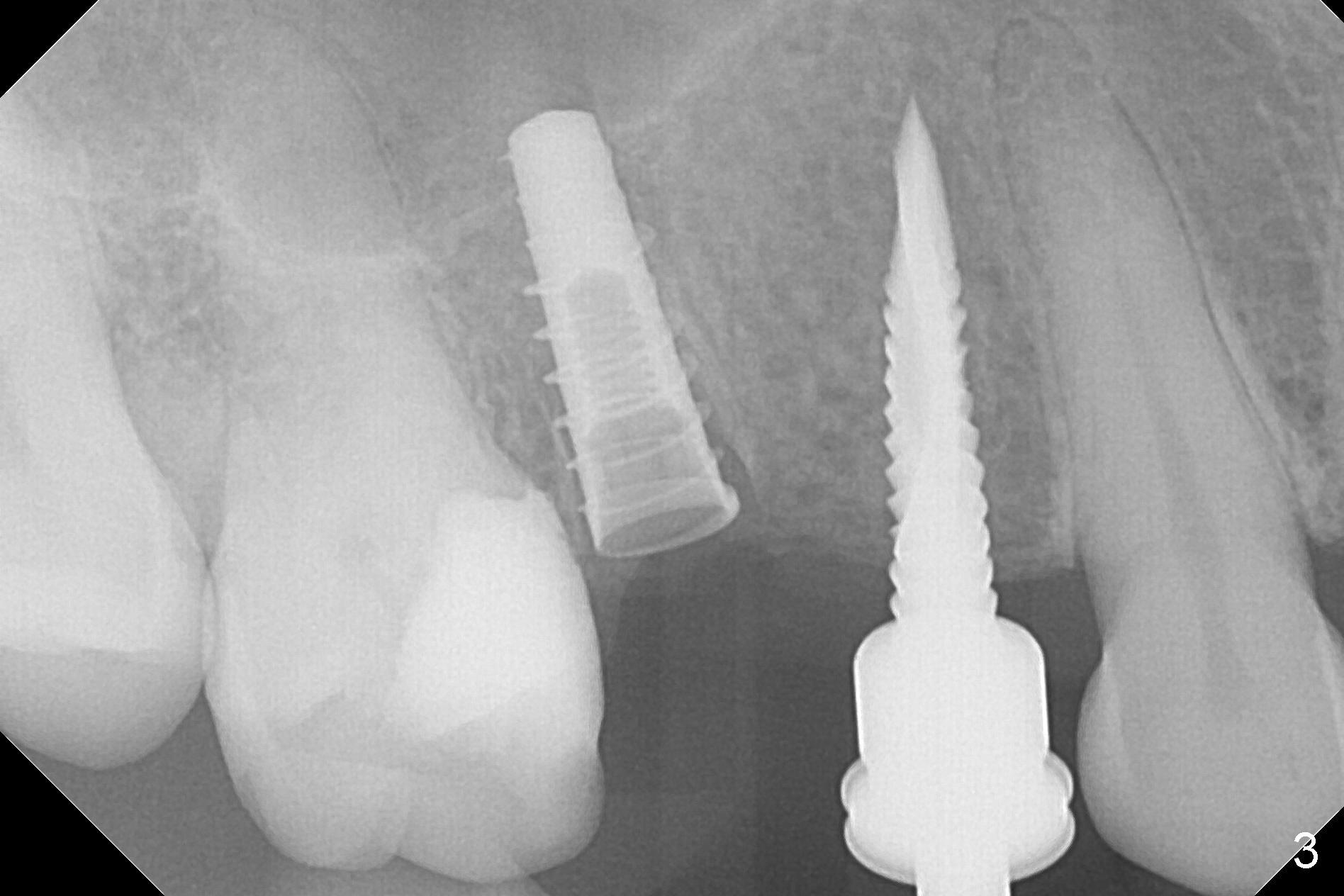
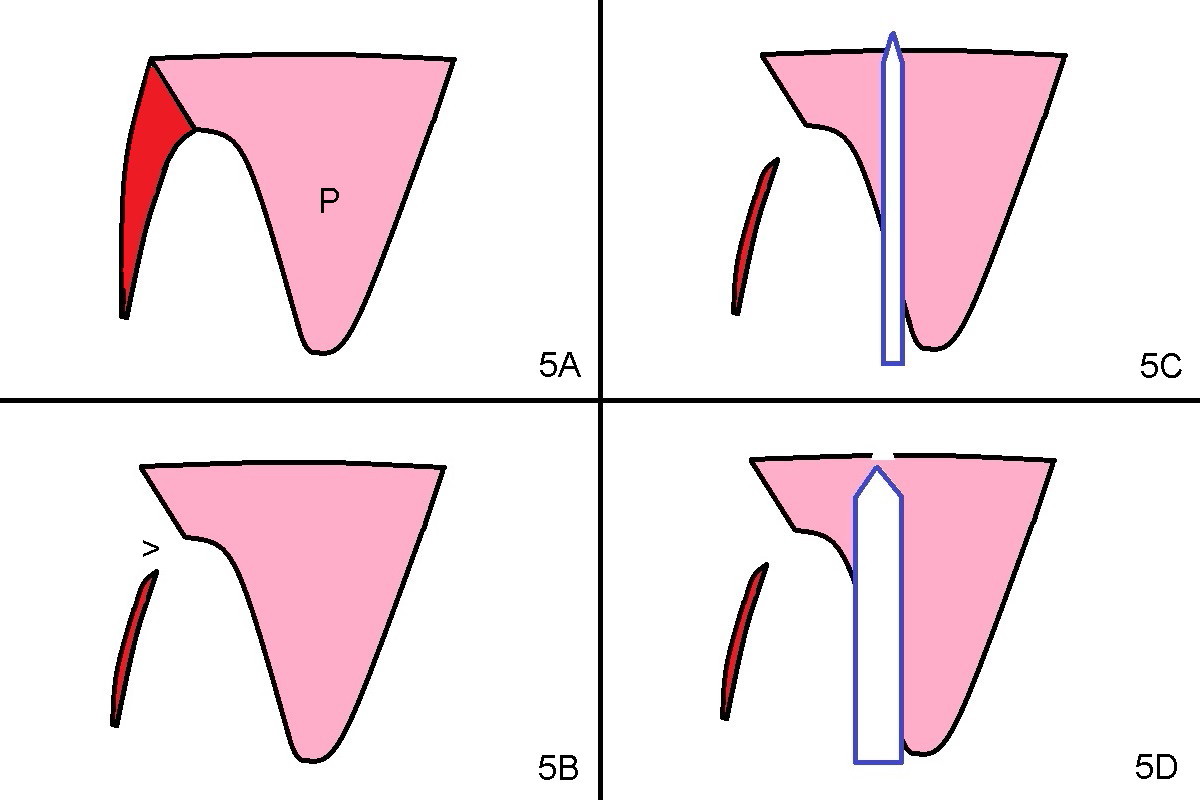
The buccal plate of the socket of #4 is thin and short (Fig.1, 5B (coronal section of the socket) red area) with apical perforation (Fig.5B >). Osteotomy at #4 starts with 1.6 mm drill in the palatal slope (Fig.2 circle; Fig.5C blue arrow), while that at #5 with Magic Split (Fig.2 black line). In fact sinus perforation occurs with the 1.6 mm drill. Osteotomy increases by using Magic Drills sequentially (2.8 and 3.3 mm) at #4 and Magic expander (3.0 mm) and the same Magic Drills at #5 (Fig.3). A 4x11 mm dummy IBS implant is placed with insertion torque of 45 Ncm at #4 with apparently intruding into the sinus (Fig.3). When a 4.5x9 mm implant is placed, the insertion torque is actually reduced (<35 Ncm, Fig.4). As osteotomy or implant diameter enlarges, it shifts buccally with less bone contact buccally (Fig.5D, as compared to Fig.5C)). In brief, once a dummy implant has achieved a reasonably high stability, do not over seat it. A small immediate implant may have more solid bone contact.
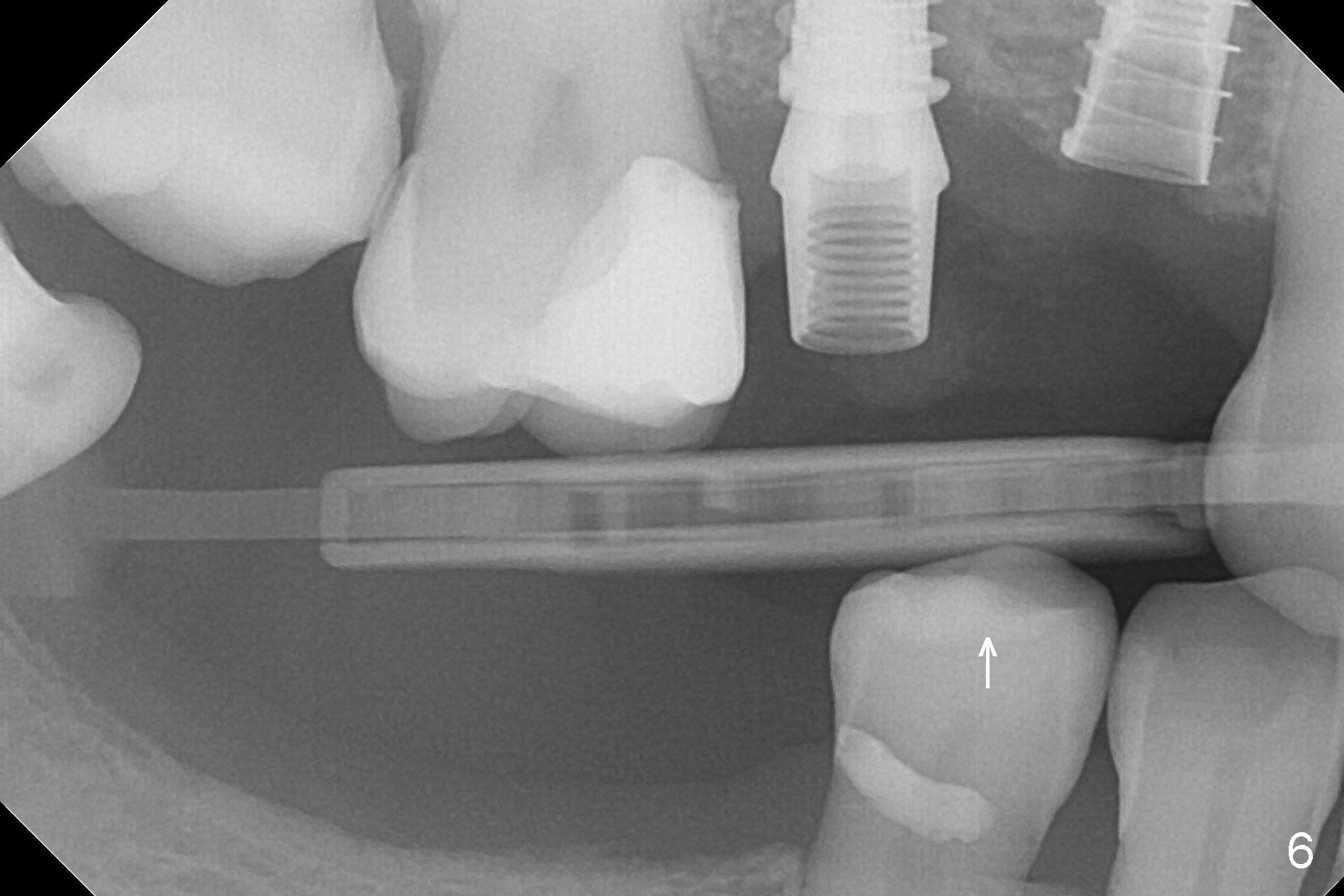
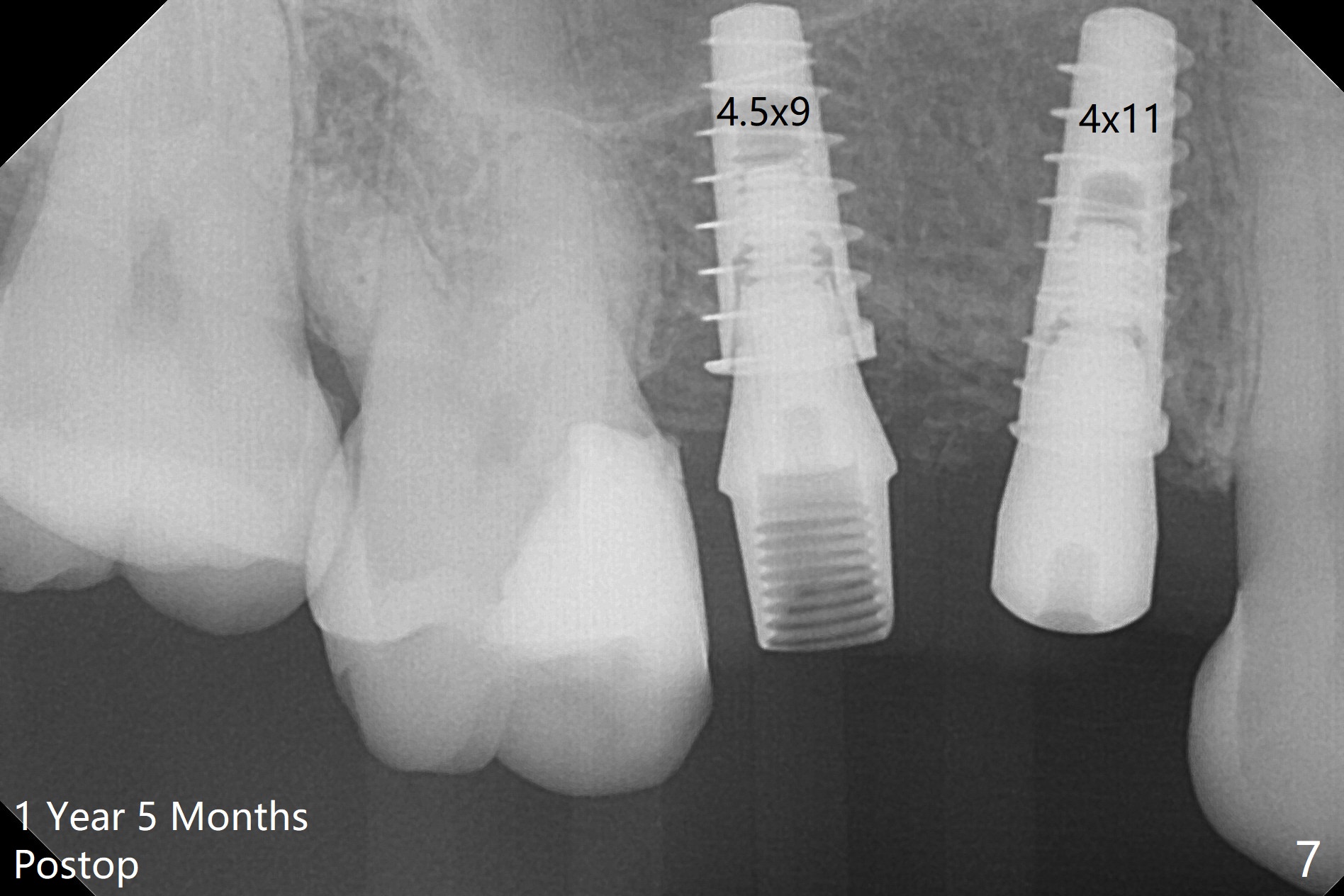
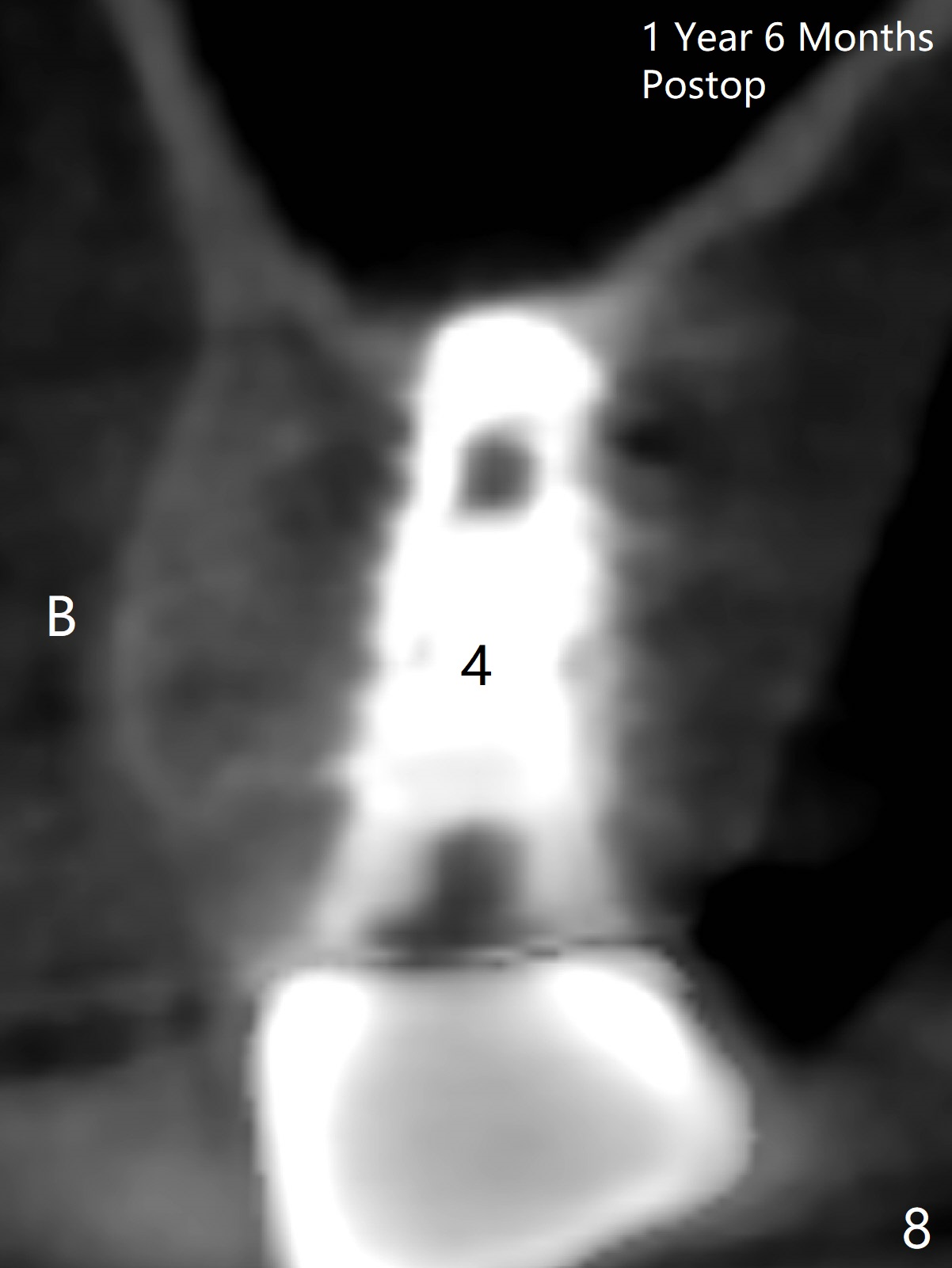
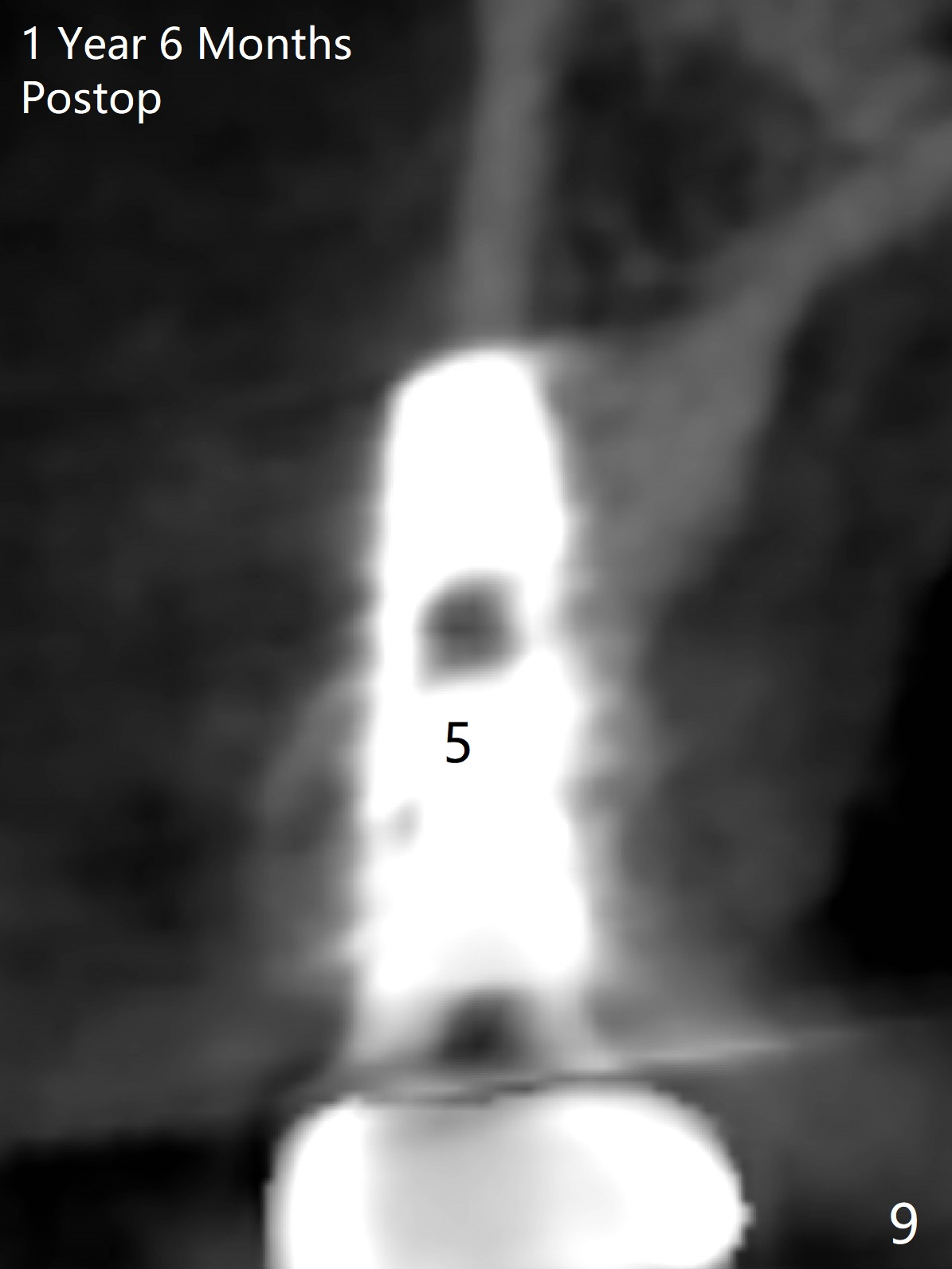
At the healed site (#5), insertion torque of a 4x11 mm implant is >50 Ncm (Fig.4). Because of supraeruption of the tooth #28 (Fig.6 arrow), a healing abutment (4x2 mm) is placed at #5 (data not shown), while a pair abutment (4.5x4(2) mm) is placed at #4 (Fig.4,6). In fact a splinted provisional is placed at #4 and 5 with a low occlusal table. There is no apparent bone loss 1 years 5 months postop (Fig.7). In fact the implants either perforate the palaatal or buccal (B) plate, as revealed by CBCT (1 year 6 months postop, immediately post cementation, Fig.8,9). It appears necessary to have guided surgery and smaller implant in the narrow ridge.
Return to
Upper
Premolar Immediate Implant
1st Year
Xin Wei, DDS, PhD, MS 1st edition 02/22/2017, last revision 09/01/2018