|
|
|
Improvement on Immediate Implant/Bone Graft M
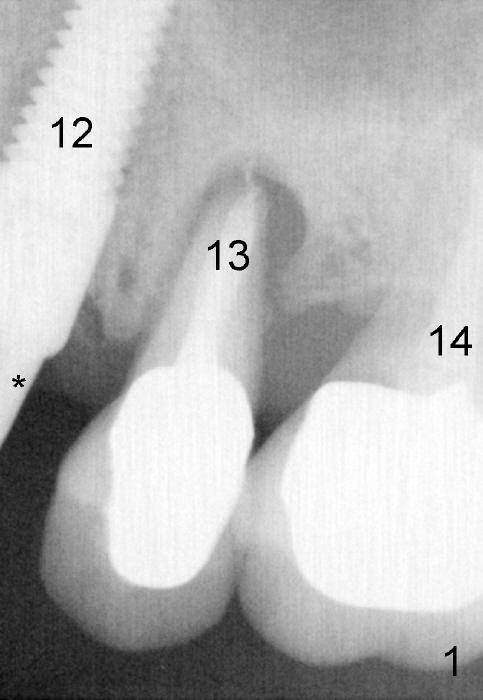
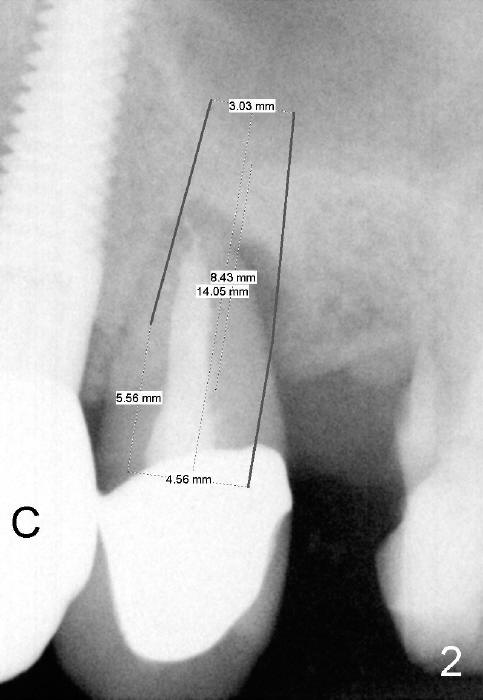
As soon as the tooth #12 is extracted and replaced with immediate implant, the patient feels that pain shifts to the tooth #13 (Fig.1 taken 3 months post implantation of #12; *: abutment). By the 7th months postop (Fig.2 C: crown), the patient agrees to have a 2nd implant for the tooth #13. Thorough debridement of the socket is planned. Sinus lift is expected. Take preop PA and photos.
To place bone graft efficiently, prepare 4 small pieces of gauze in a dap pen dish. Dissolve Clindamycin with 2% Xylocaine (or 4% Septocaine) with 1:50,000 Epinephrine. Use 3 pieces of gauze as usual, followed by normal saline irrigation. Thoroughly debride the socket, since there is a fistula buccodistally. Finish sinus lift and bone expansion/condensation with RT2,3, followed by 4.5x17 mm tap at the depth 14 mm. The first intraop PA is taken. If the bone is dense, use a 2 mm pilot drill to start osteotomy.
Use the last piece of the gauze for hemostasis before bone grafting. Wet the bone graft lightly with blood squeezed from the last gauze. Squeeze extra blood out of the bone graft inside the plastic dap pen dish with dry 2x2 and suction tip. Do it as quick as possible so that hemorrhage does not recur before bone grafting. Use 2.5 or 3.0 mm Bicon flat end osteotome to push bone graft into the sinus. A 4.5 or 5x14 mm tapered implant is to be used.
When the patient returned last time, he wanted to do an immediate implant for the lower right 2nd molar first.
Return to Upper Bicuspid Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/23/2014, last revision 02/09/2020