



|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Intraop Modification of Immediate Provisional M
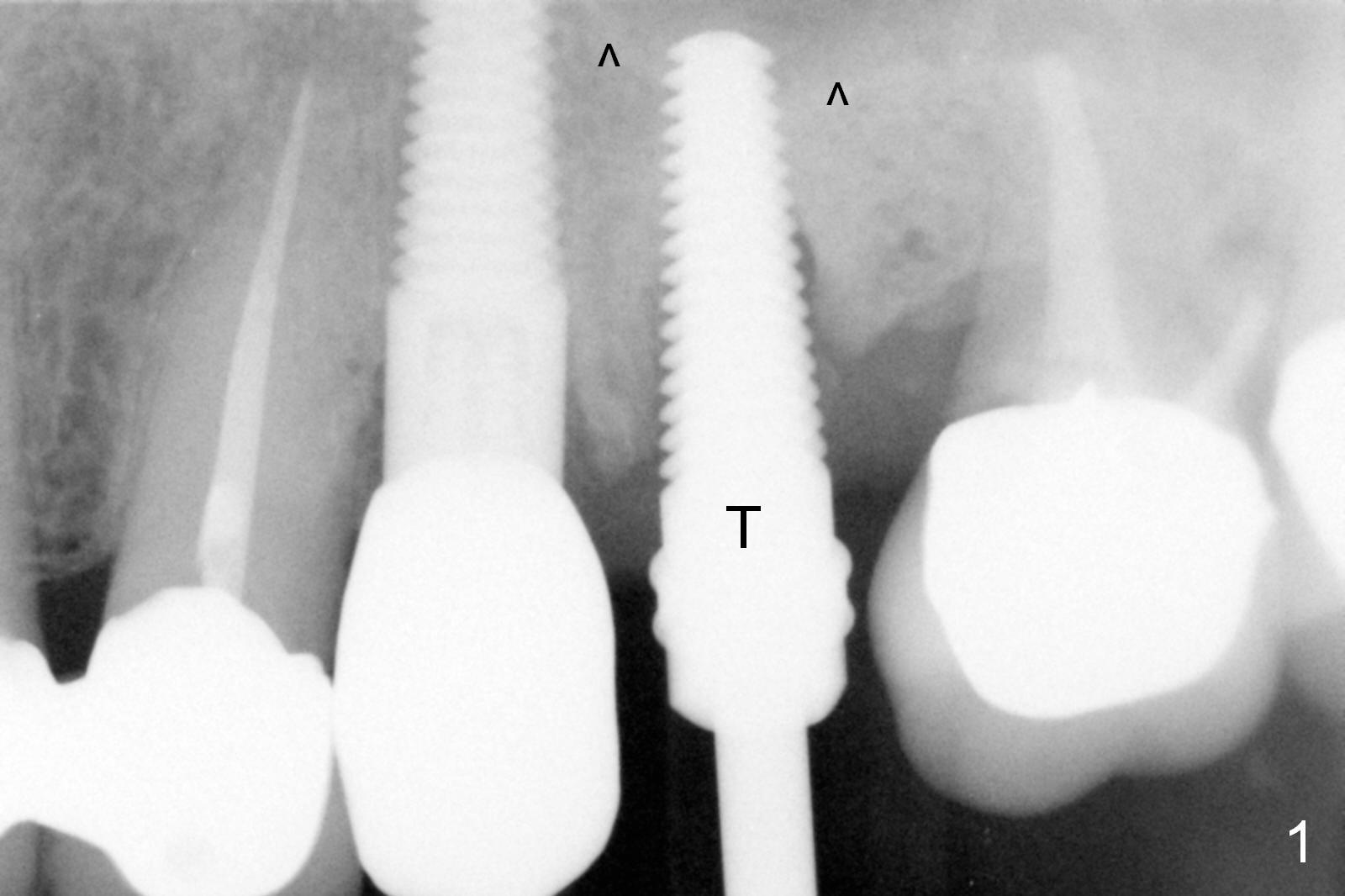
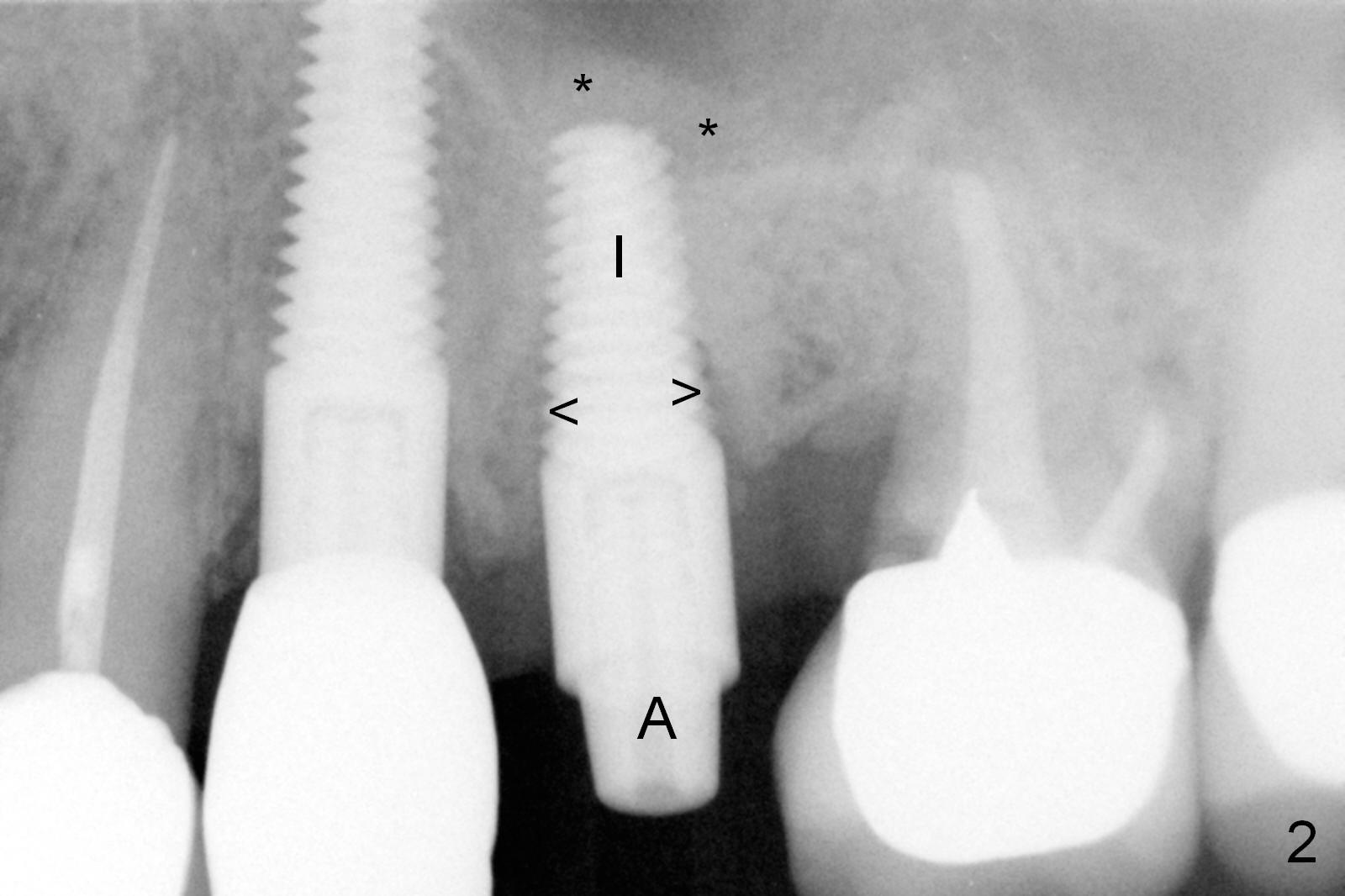
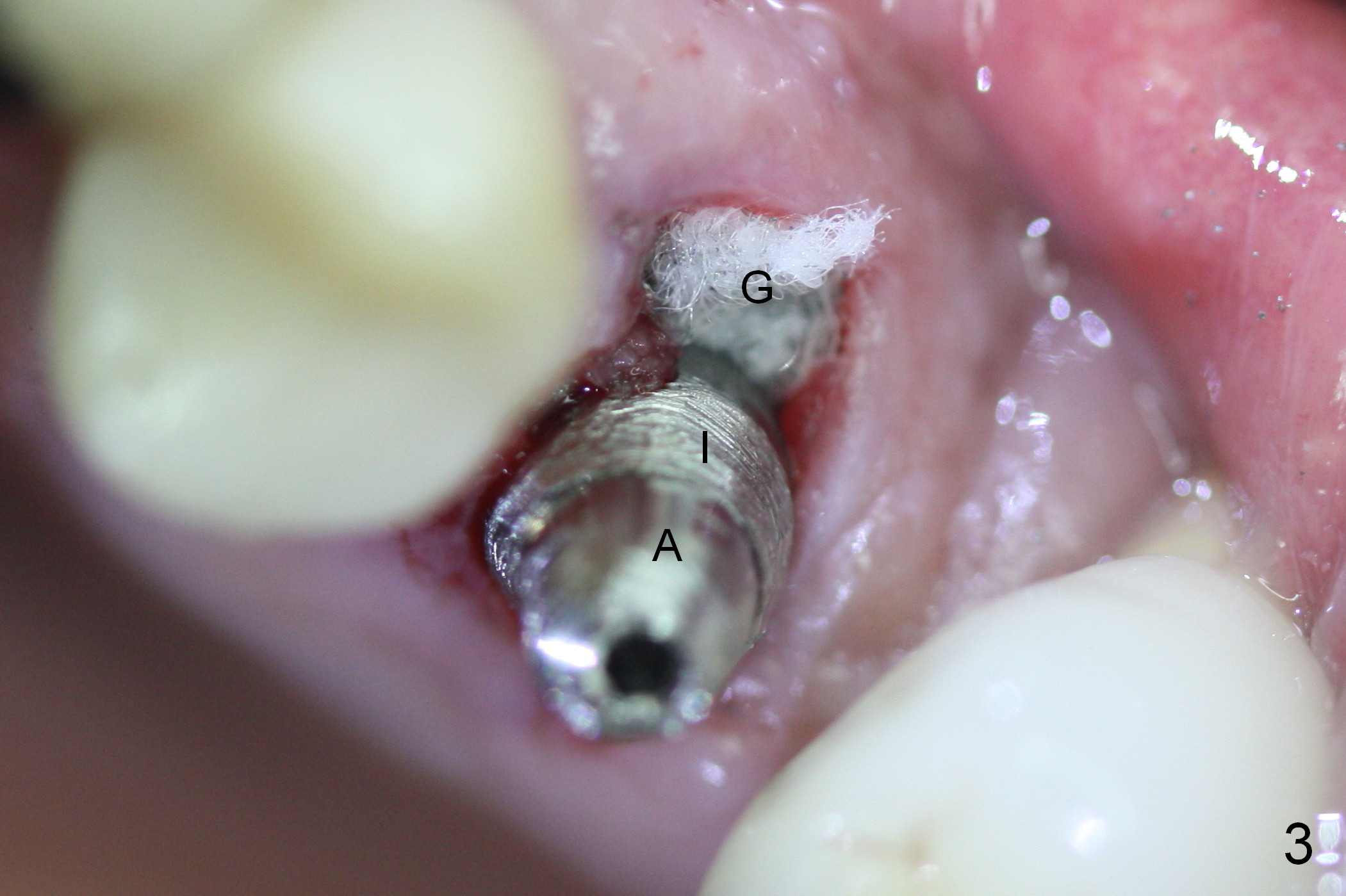
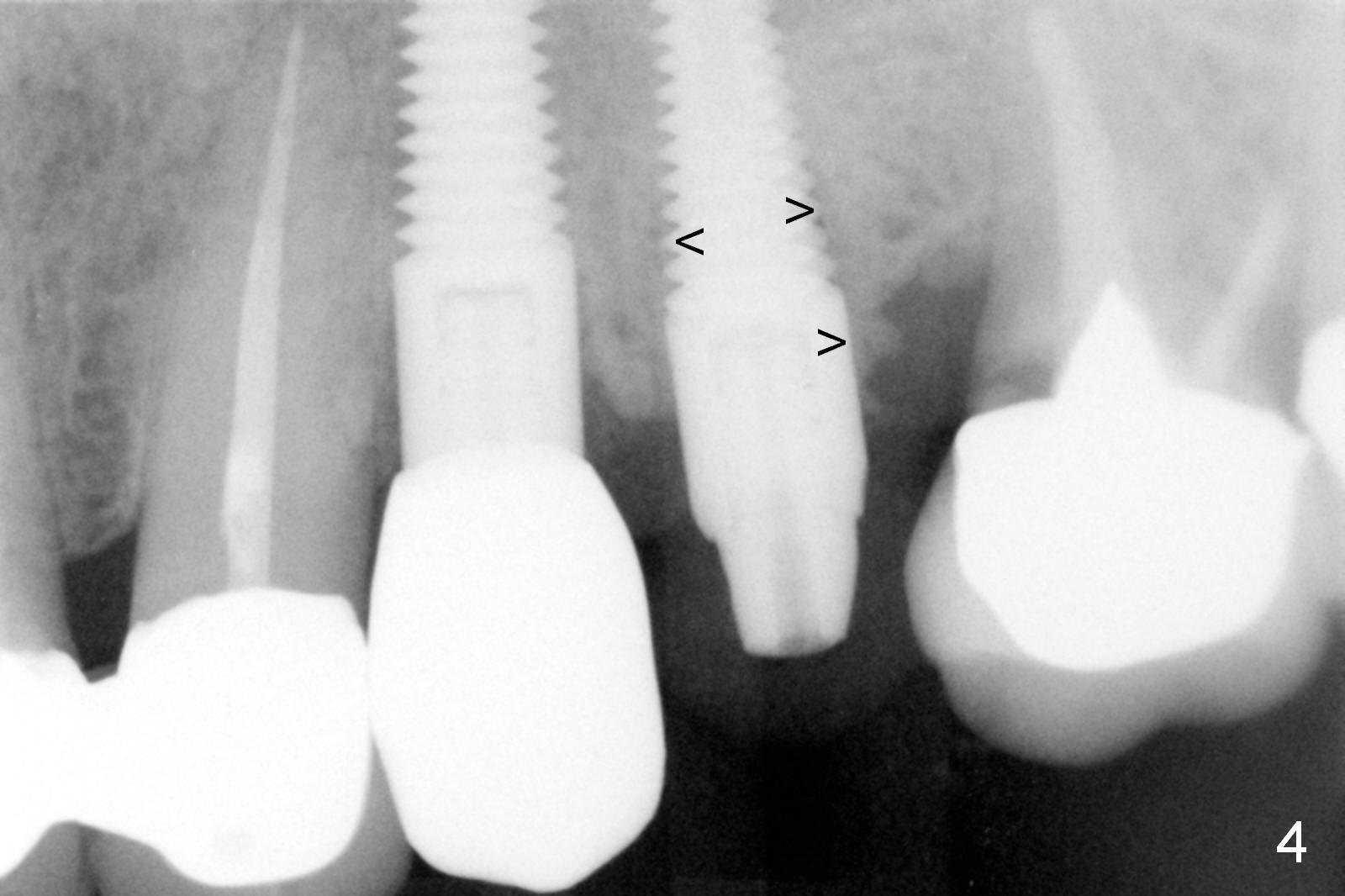
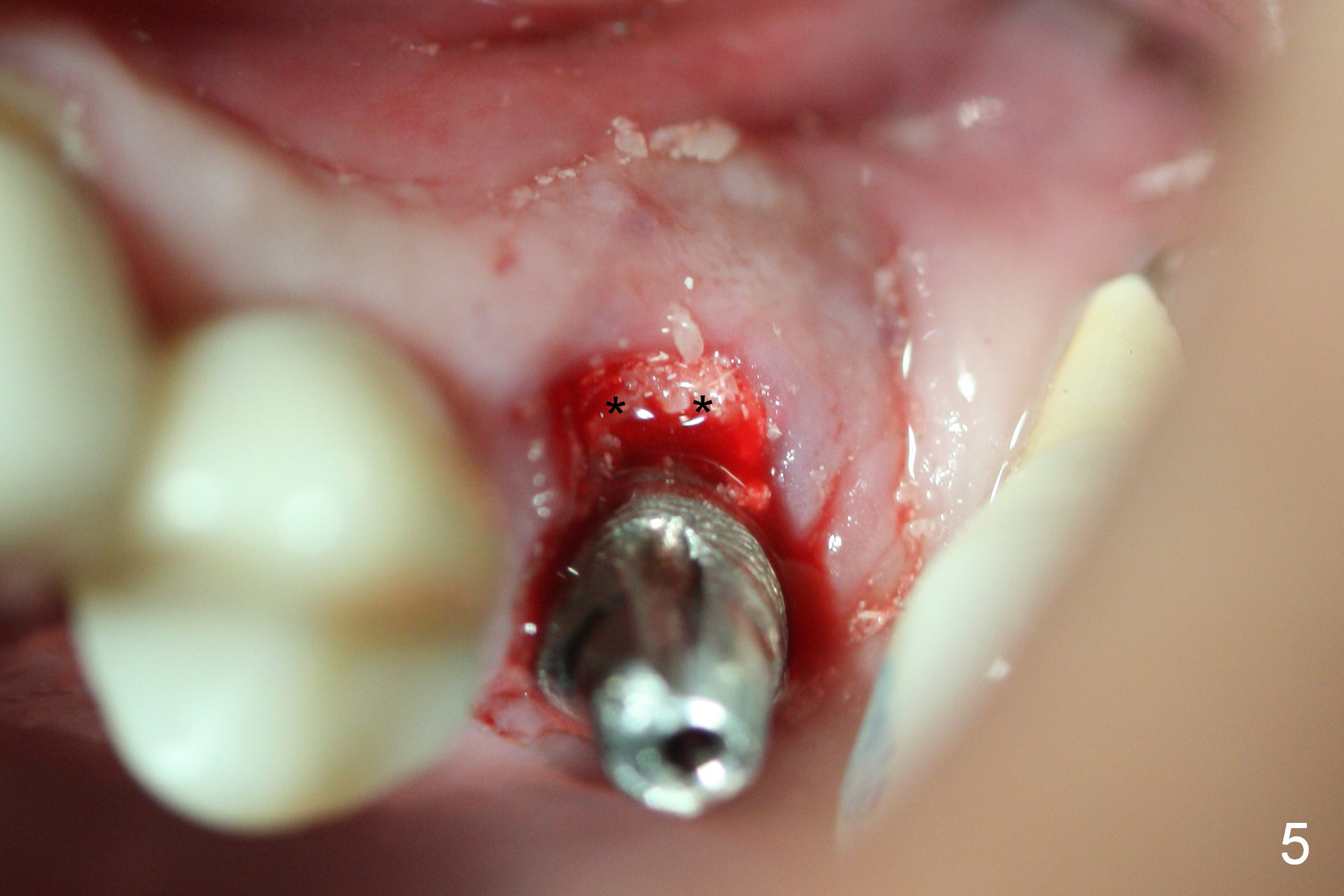
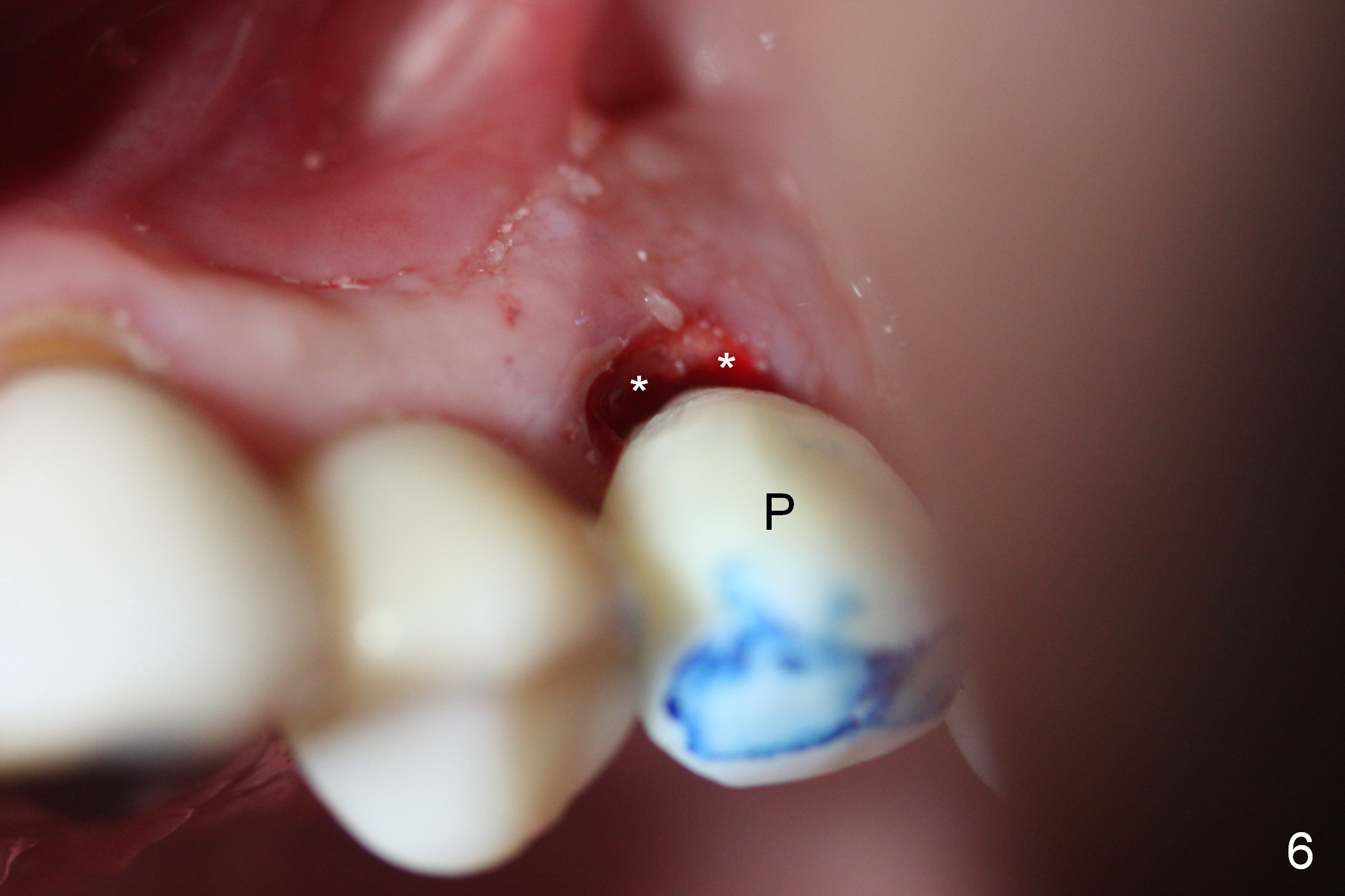
Extraction of the affected 2nd premolar is easy; the apical bone is so hard that drill and reamers have to be used for osteotomy, followed by insertion of a 4.5 mm tap with stability (Fig.1 T). The sinus floor (^) is lifted. There is no sign of sinus membrane perforation before placement of a 4.5x14 mm implant (Fig.2 I); sinus lift is performed (*: autogenous bone mixed with Mineralized Cancellous Human Allograft, Impladent); an immediate abutment (3.5x3 mm) is placed (A). With gauze placed in the buccal gap (Fig.3 G), the margin of the implant (I) is prepared for an immediate provisional fabrication. Mixture of autogenous bone (from reamers), allograft and Osteogen is placed in the remaining socket (Fig.4,5 *). When the relined (1st modification), trimmed and polished provisional is reseated (Fig.6 P), the bone graft (*) is not completely covered. New acrylic (2nd modification) is added to the margin of the provisional (Fig.7 *) for containment of the graft. There is almost no buccal plate; Osteotape (collagen membrane with Osteogen) is placed against the buccal wall of the socket prior to bone grafting. The remaining small pieces of the Osteotape (Fig.7 <) are laid over the bone graft before reseating the final provisional. With "complete socket seal", perio dressing is unnecessary.
The patient returns 7 days postop, reporting that the provisional has been dislodged several times. The gingiva adapts to the provisional with occlusal clearance (Fig 8 *). The rough surface of the implant is exposed (Fig.9,10 *). It appears that some of bone graft has been lost. The provisional should be trimmed so that the gingiva may be able to grow over the rough surface.
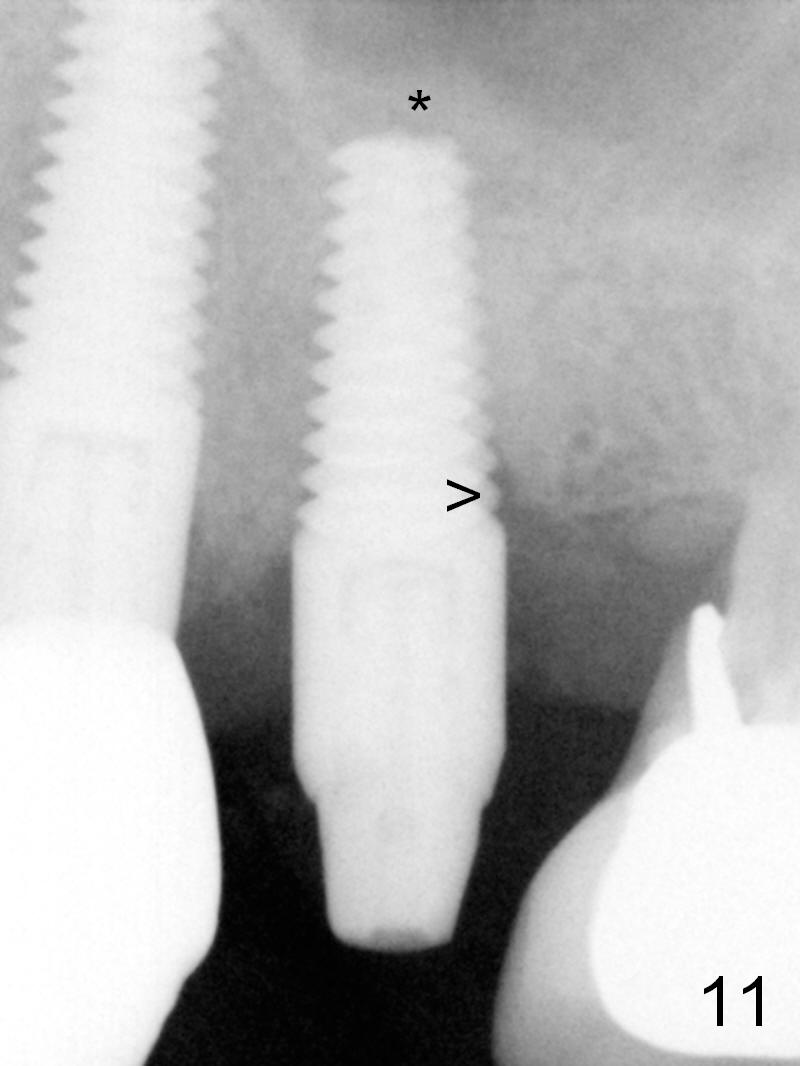
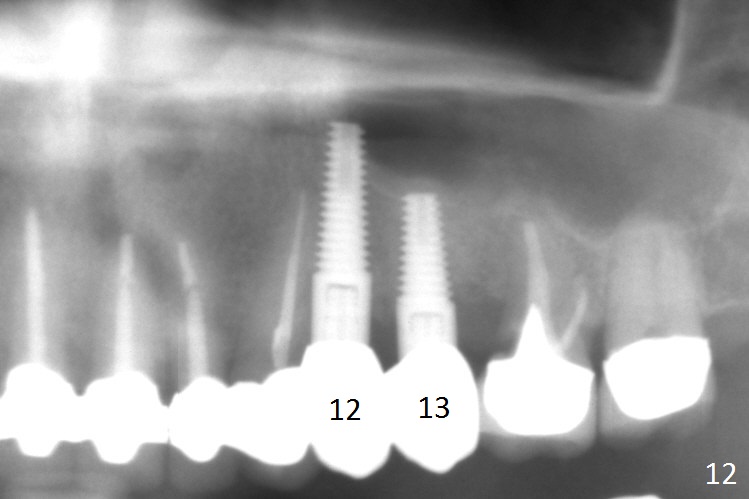
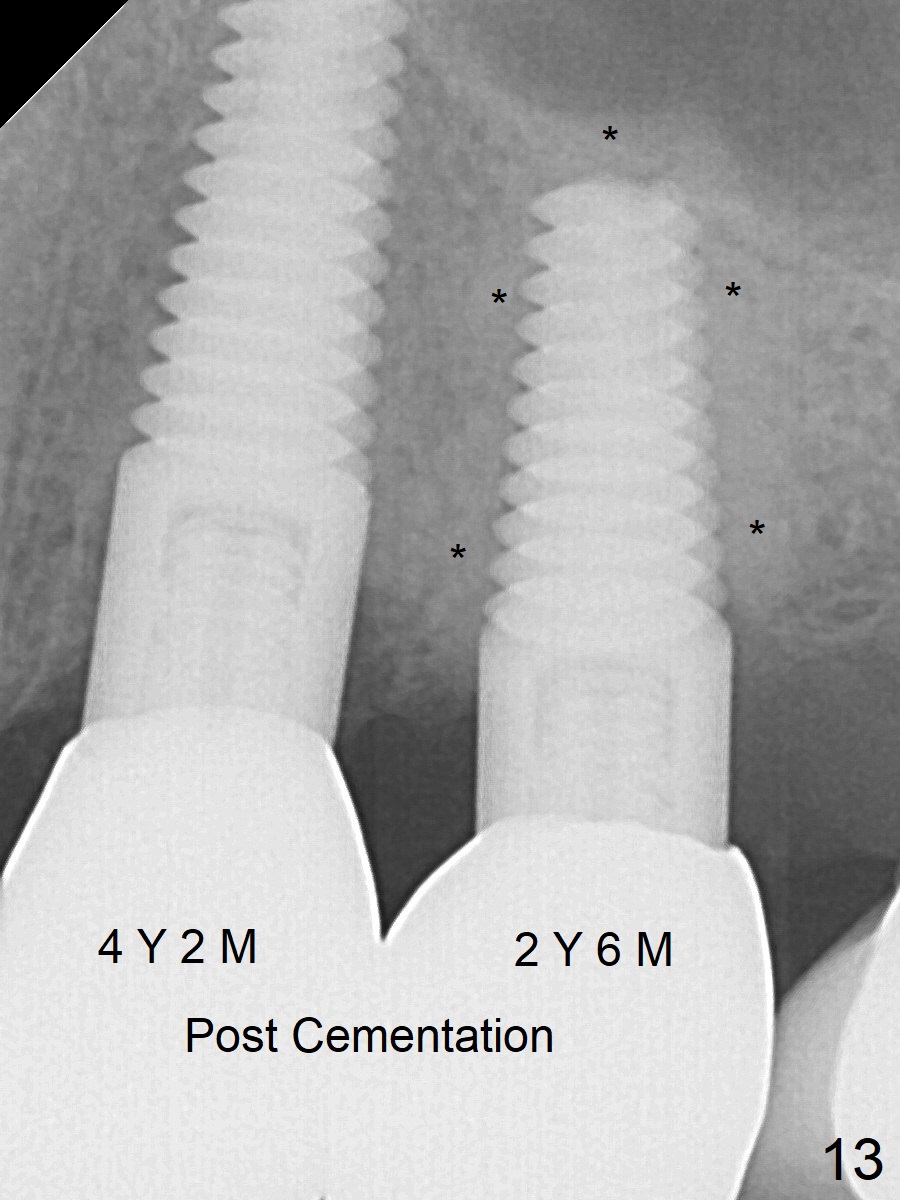
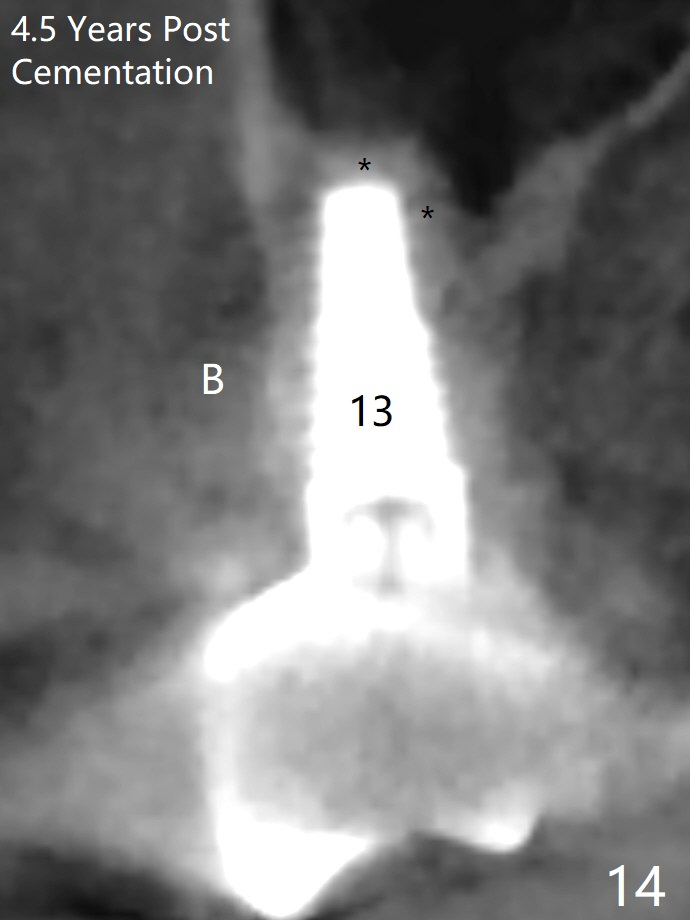
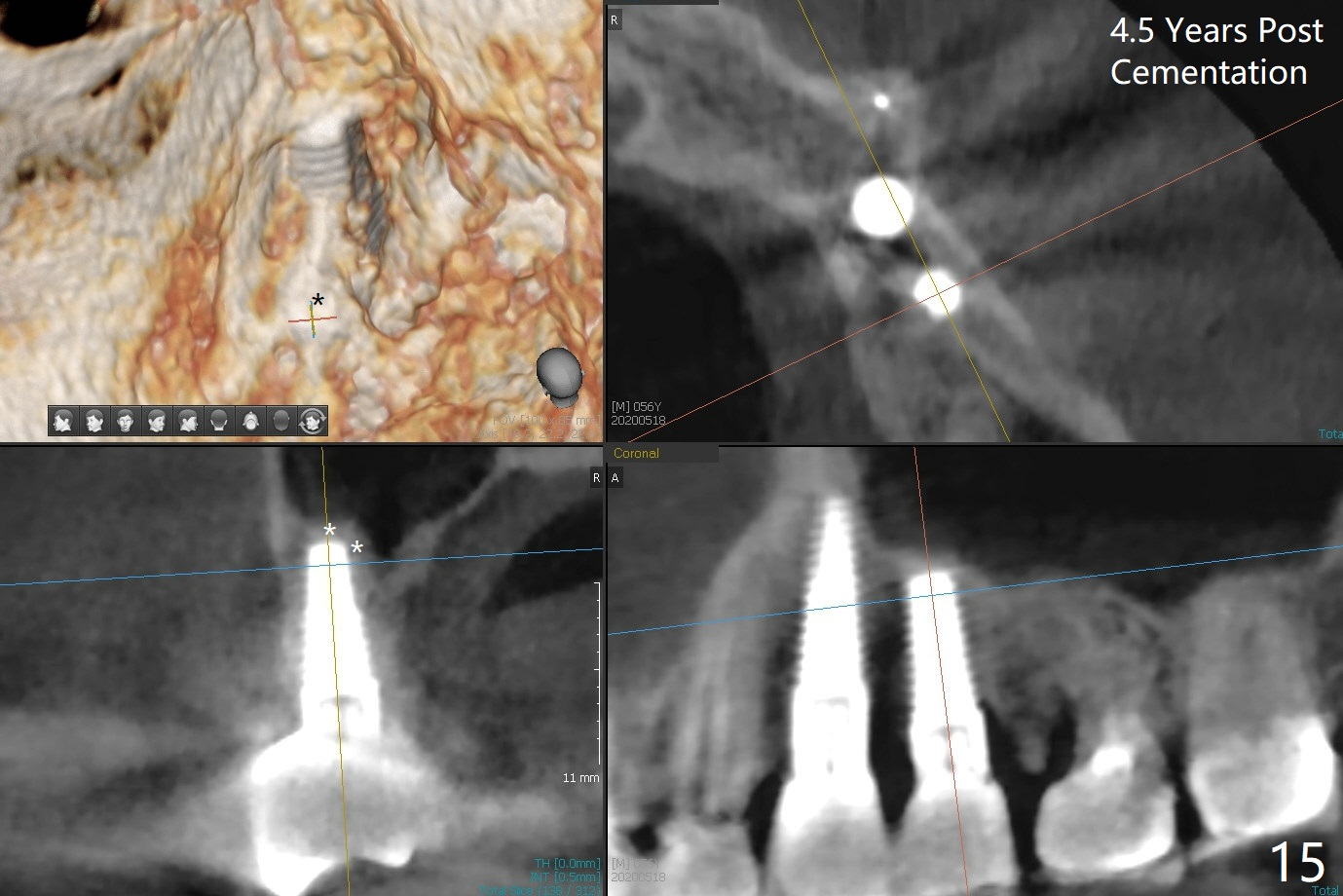
The distal threads appear not covered by the bone 2.5 months postop (Fig.11 >). His oral hygiene is excellent with healthy gingiva around the implant when the permanent crown is cemented. Panoramic X-ray is taken 3 years and 1 year 5 months post cementation for #12 and 13, respectively (Fig.12). The bone density around the implant at #13 increases 2 years 6 months post cementation (Fig.13 *). The bone density of the sinus lift (Fig.14,15 *) is essentially the same as that of the bone buccal (B) and palatal to the implant 4.5 years post cementation. The upper left panel is a 3D view from the sinus.
Return to Upper Bicuspid Immediate Implant,
Posterior Immediate Implant,
Clindamycin,
12,
31,
3/4
Xin Wei, DDS, PhD, MS 1st edition 07/30/2015, last revision 05/18/2020