
.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
Engagement of Non-Immediate Implant into the Sides of the Sinus Floor
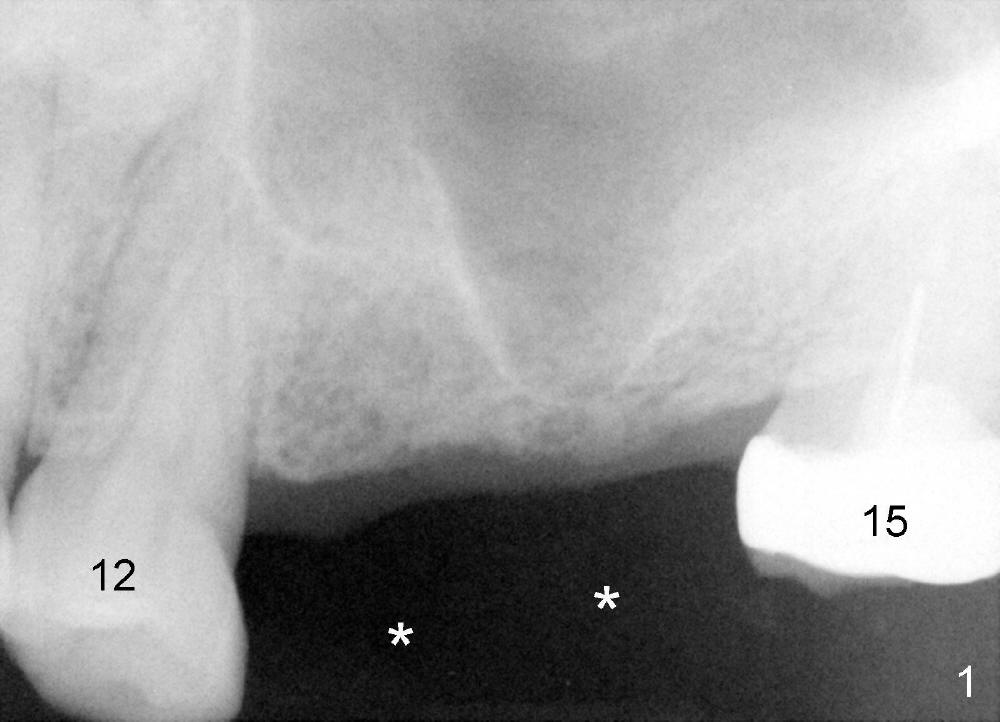
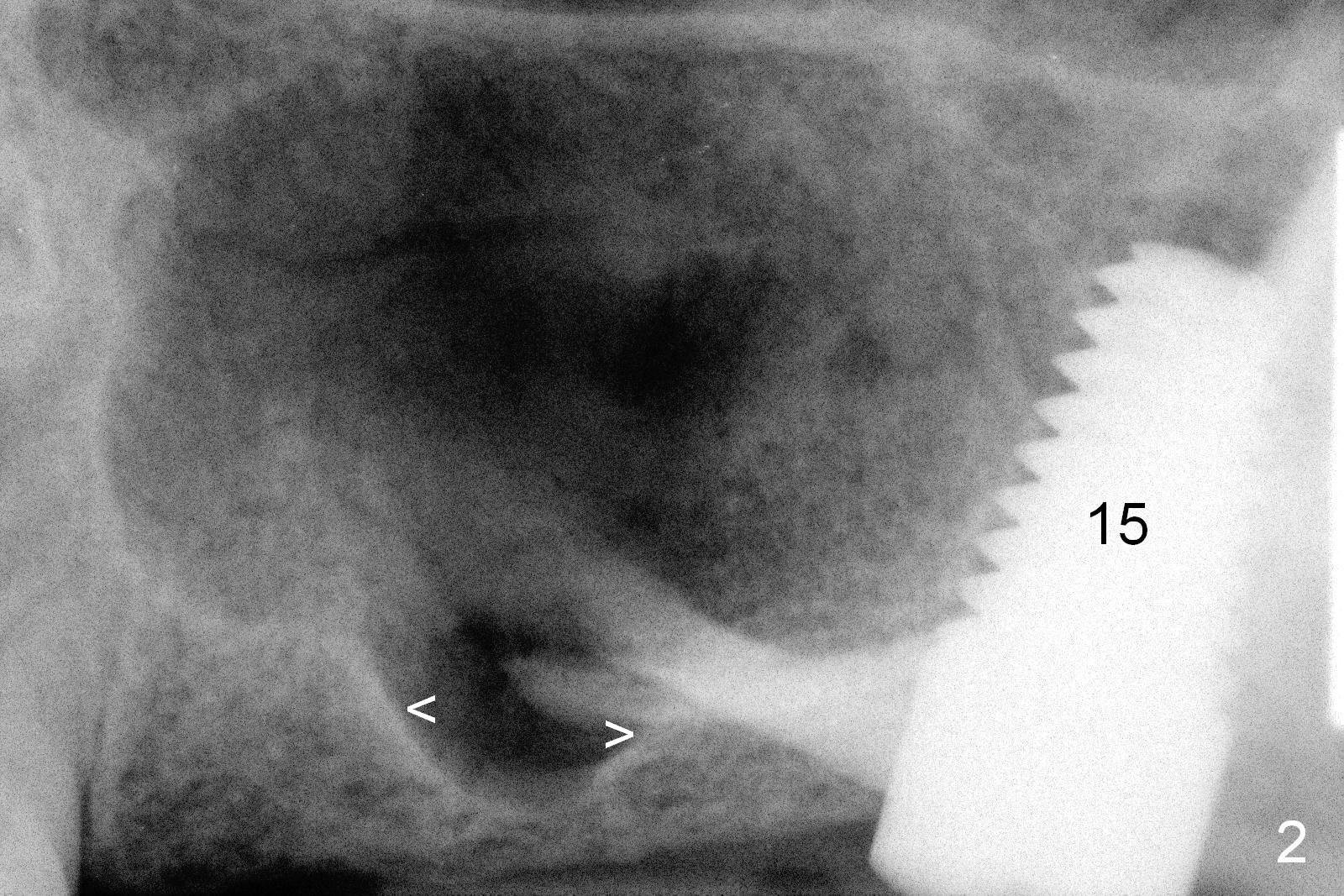
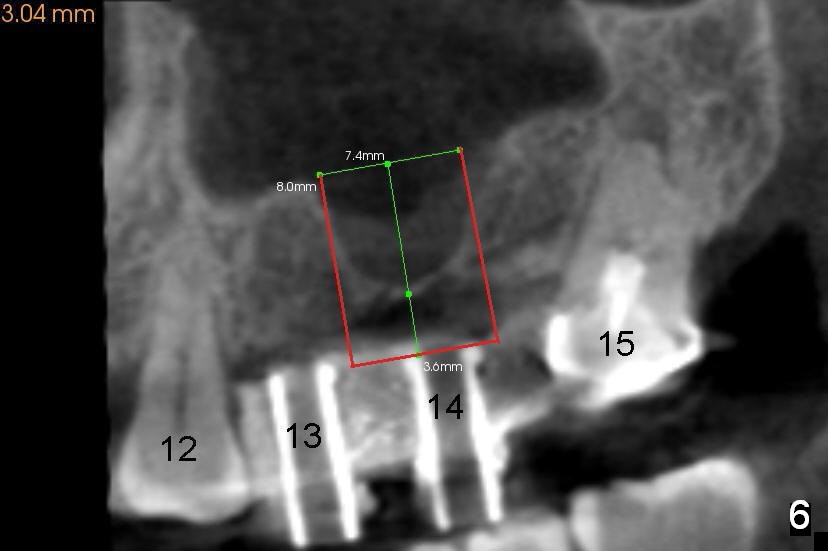
A man in his 70s had a partial denture in the upper left quadrant (Fig.1) prior to loss of #15, which was replaced by an implant (Fig.2). Lateral window sinus graft was tried without success in preparation for $14 implant placeement. Recently the partial was lost. Two missing teeth are going to be restored by implants with sinus lift in the crestal approach. Although the bone height is limited (2 mm), the implant at the site of #14 is able to obtain primary stability by engaging into the sides of the sinus floor (Fig.2 arrowheads).
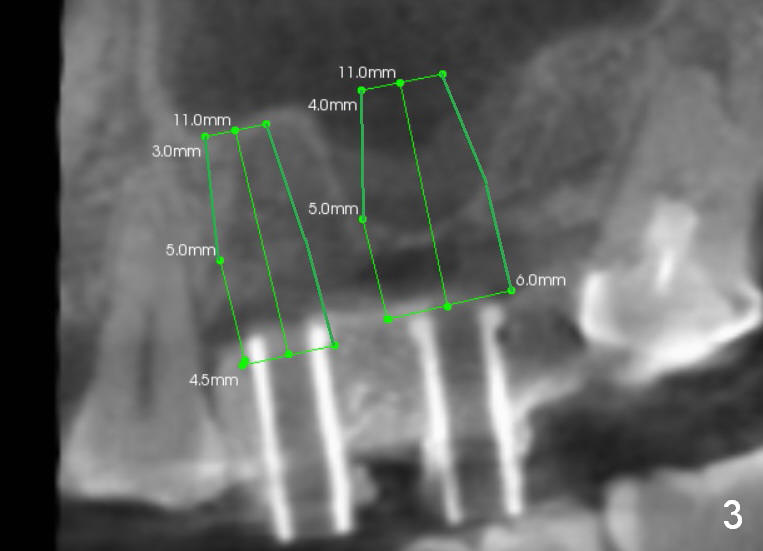
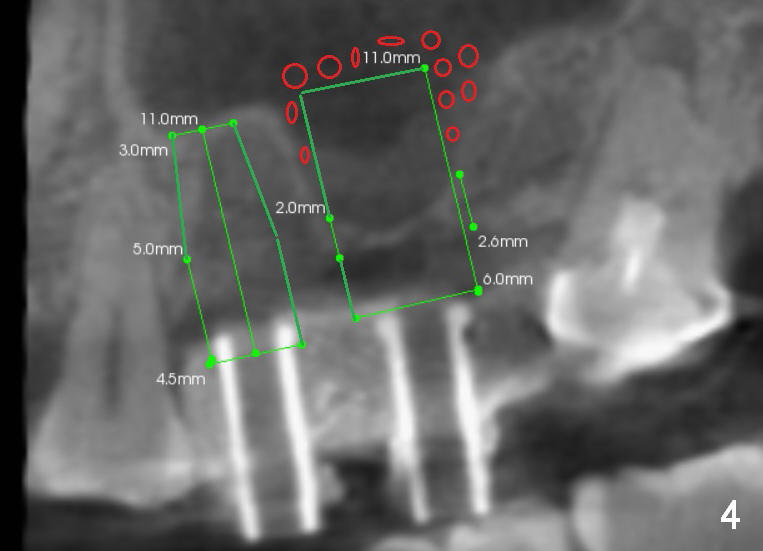
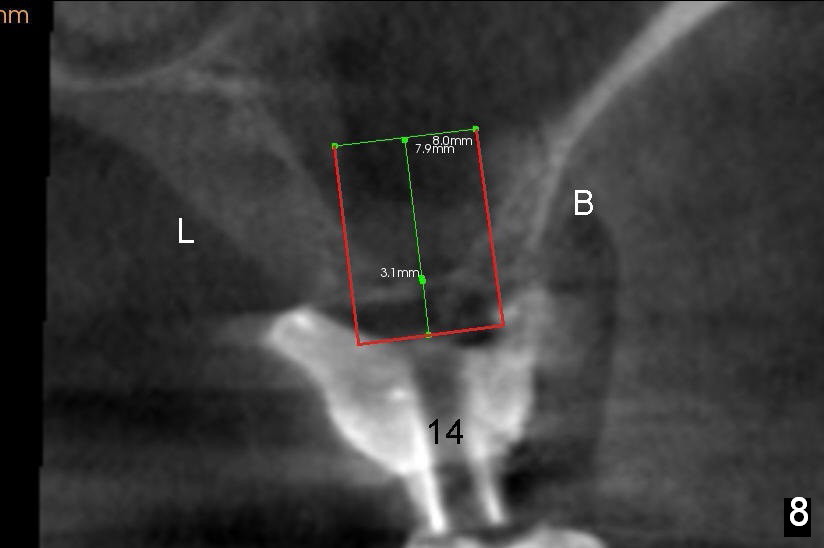
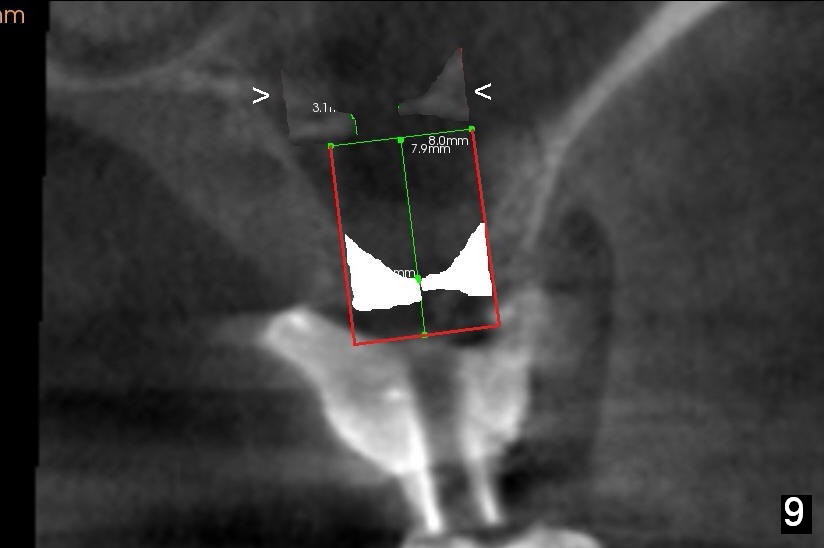
After crestal incision, a 3.5 or 4 mm trephine bur is used for 2 mm at #14. The regional sinus floor is lifted using a Bicon flat-end osteotome, followed by bone graft and taps. If the 6x11 mm tapered tap does not gain stability (Fig.3), use either 6x11 mm round tap (Fig.4) or 7 or 8x11 mm tapered tap (Fig.5). If the last does not work, try a larger round tap (Fig.6). In all, the sinus floor is pushed upstairs and an implant is inserted to be engaged into the sides of the sinus floor (Fig.7).
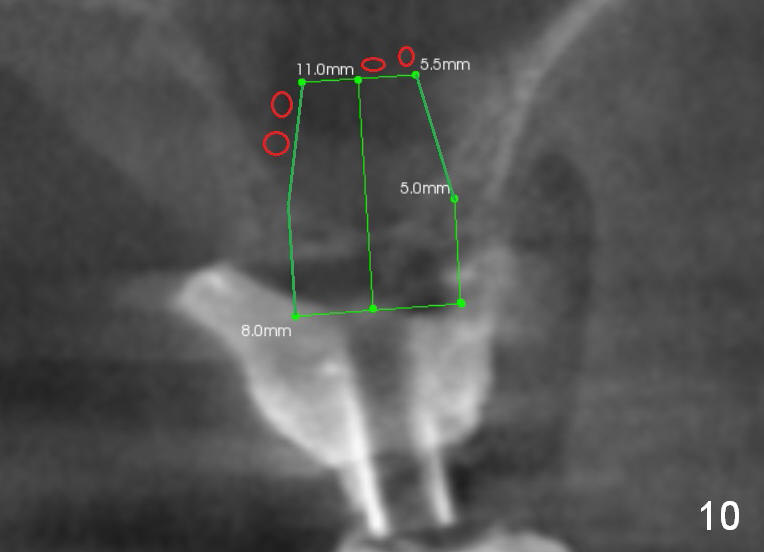
Coronally, a round implant does not appear to obtain more bone contact than a tapered one of the same diameter (Fig.8,10). Internal sinus lift works for this case?
Return to Upper Molar Immediate Implant,
Professionals
Xin Wei, DDS, PhD, MS 1st edition 05/17/2015, last revision 05/20/2015