%20to%20hold%20perio%20dressing.jpg)
%20(not%20secure)%20to%20hold%20perio%20dressing.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
||
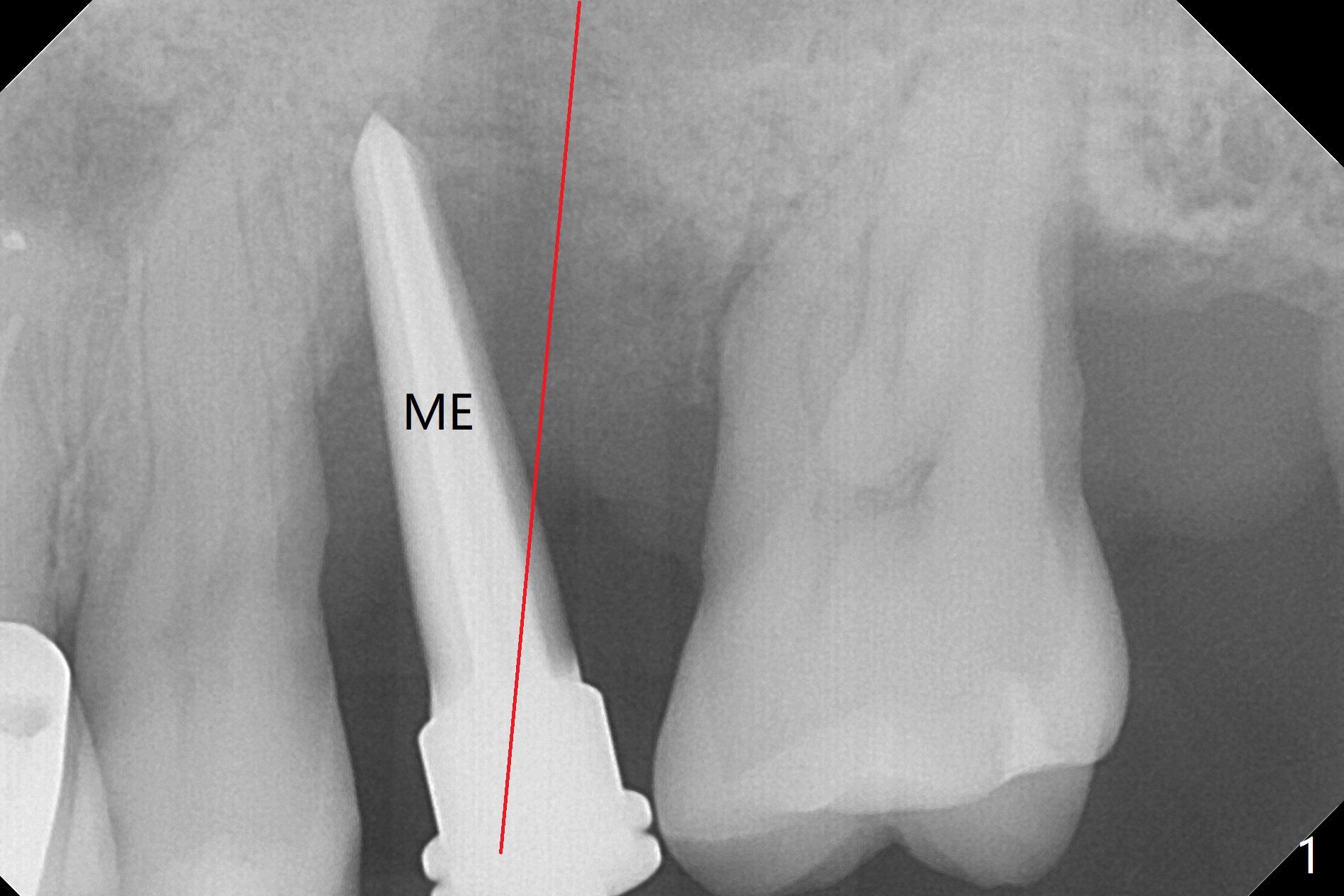
Reduced Buccopalatal Width Post Socket Preservation
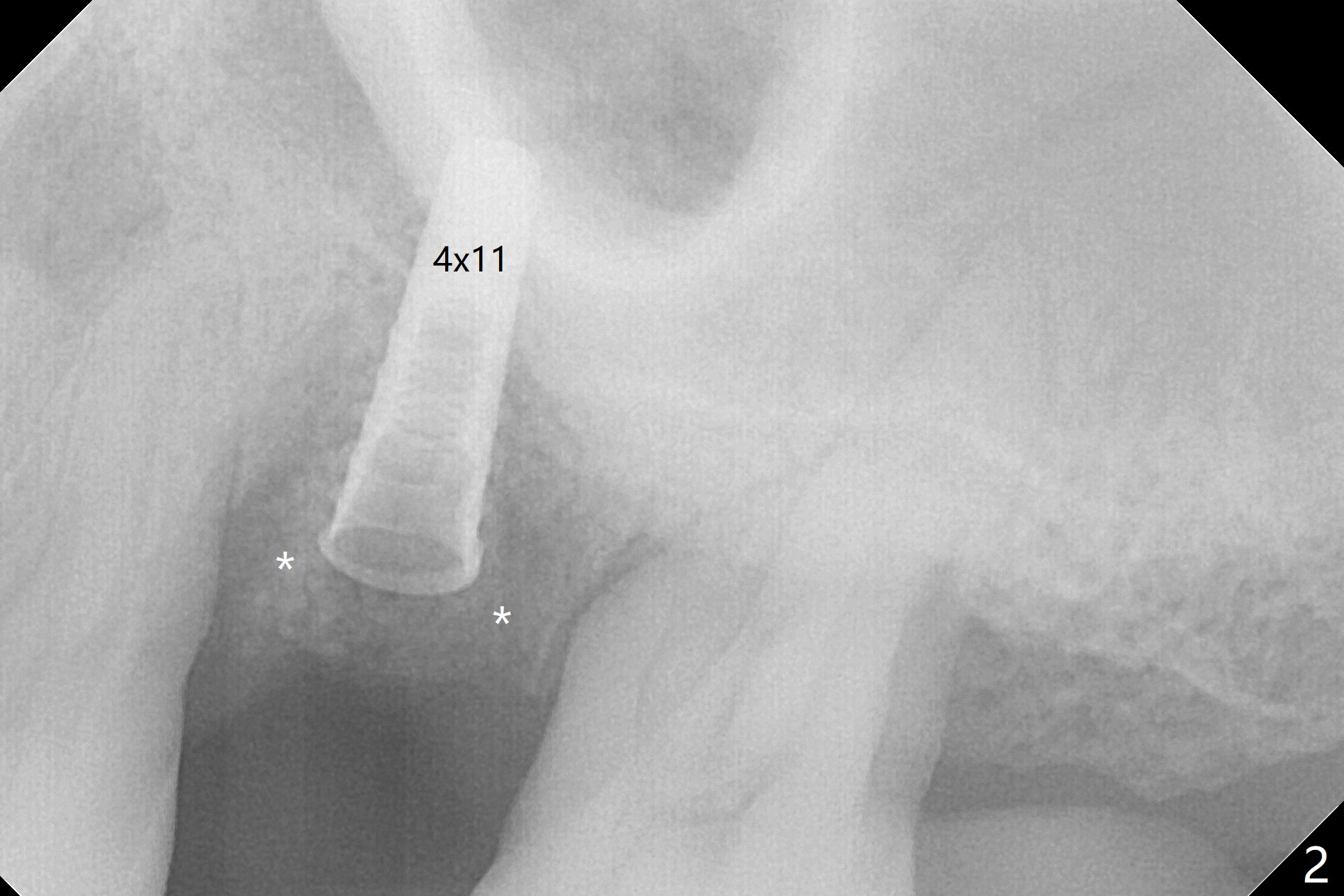
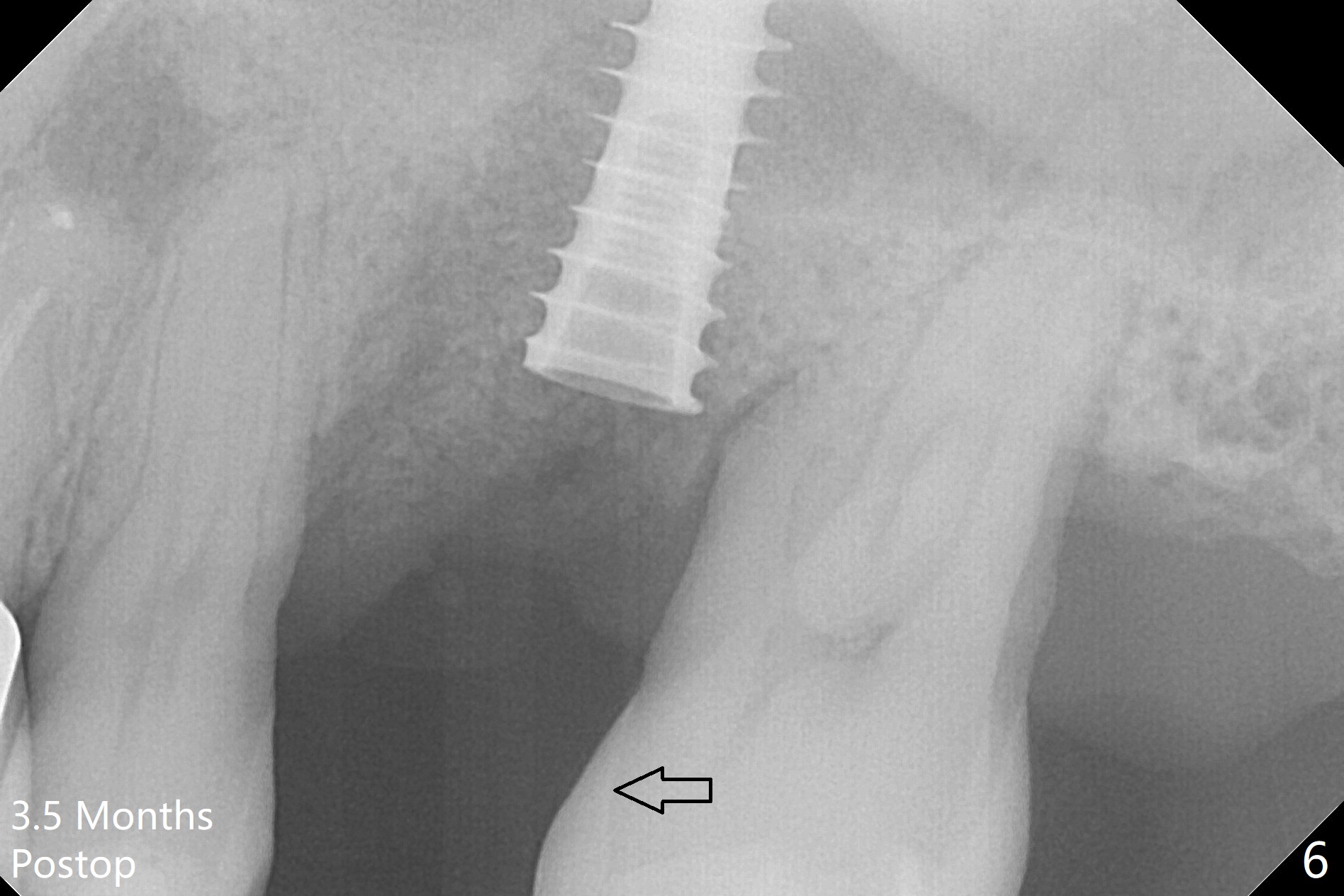
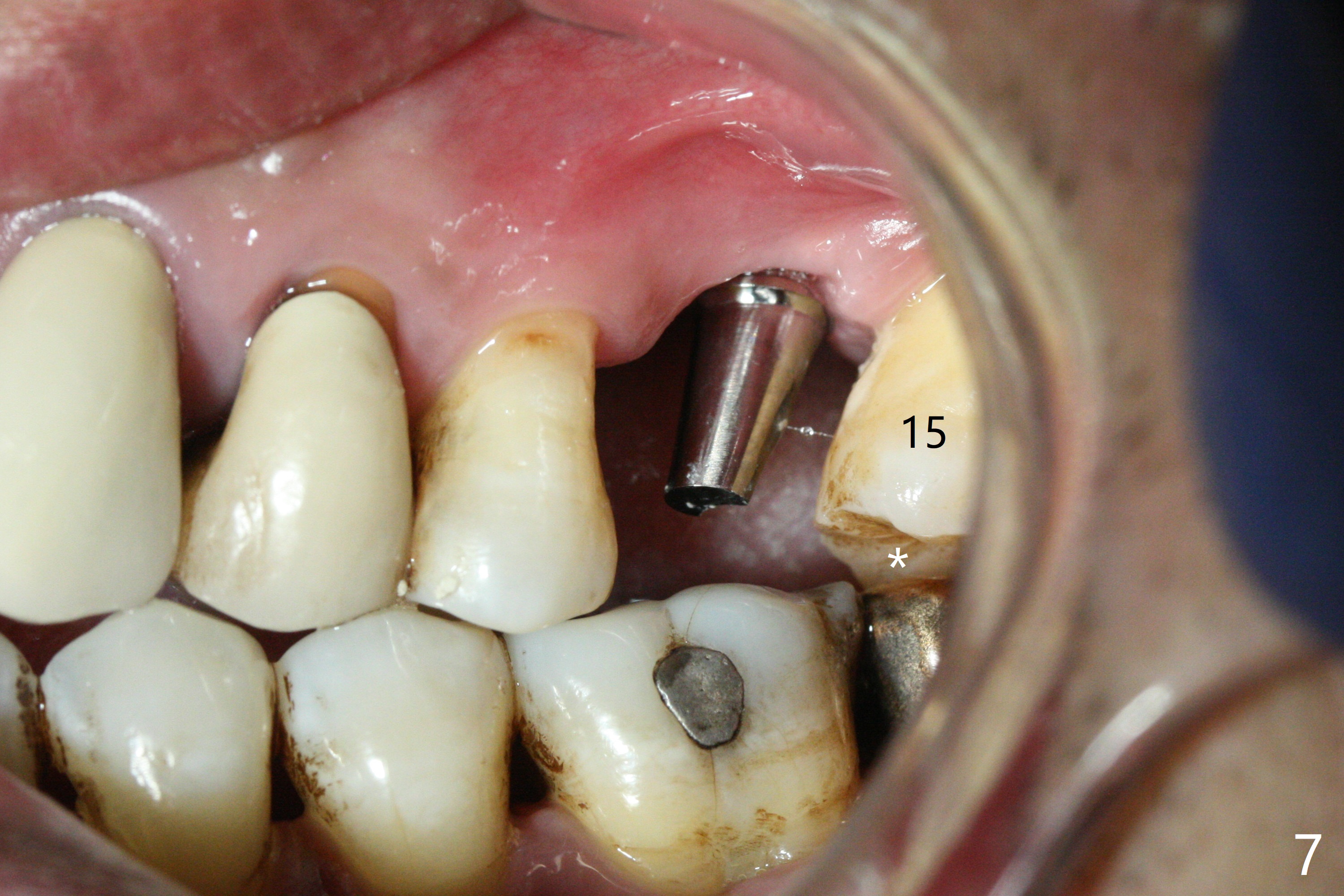
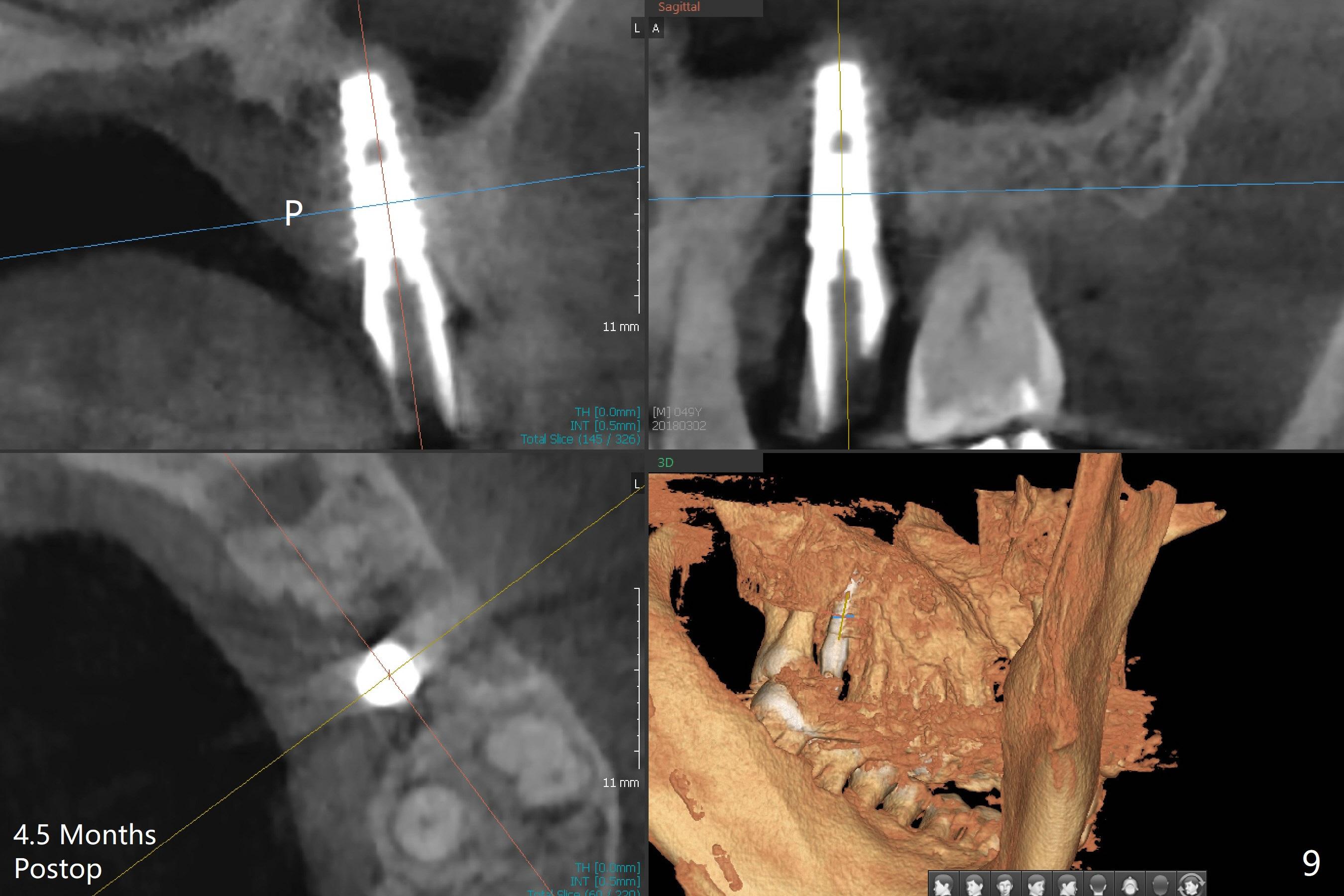
Osteotomy is initiated with Magic Split and 3 mm Magic Expander (ME, flapless) nearly 3 months post socket preservation. To improve the trajectory, the ME is redirected (Fig.1 red line). After use of 3.8 mm ME, Vanilla Graft is placed in the buccal and mesial aspects of the osteotomy. Following reuse of 3 and 3.8 mm MEs, a 4x11 mm dummy implant is inserted with stability (Fig.2 (*: allograft)). More of allograft is placed prior to placement of 5x11 mm IBS implant (Fig.3,4 (~30 Ncm)). The latter is placed palatal. Last the allograft is placed palatal. A 5x4(2) mm abutment is placed to hold periodontal dressing in place. When the ridge is narrow, the implant should be small; 4 mm probably the most appropriate in this case. There is a buccal gap 2 weeks postop (i.e., after dislodgement of periodontal dressing, Fig.5). The implant and abutment appear to be loose ~ 1.5 months postop. The pair abutment is changed to a healing one (5x3mm). The implant seems to be osteotointegrated 3.5 months posotp (Fig.6). Because of the mesial shift of the tooth #15 (Fig.6 arrow (6 months post #14 extraction; anterior open bite)), an angled abutment (5x4mm, 15 degree) is used (Fig.7). Limited orthodontic treatment has to be initiated because the mesially shifted #15 has no occlusal contact mesially (Fig.7 *). A provisional is fabricated with light supra-occlusion. A separator is placed between #14 and 15. Once a space is created in a week, acrylic is added to the distal surface of the provisional and the separator is re-used. In fact the implant is found to be unstable 4.5 months postop (Fig.8,9). The palatal (P) plate is thin and incomplete. The provisional is reduced infraocclusal. Two months the implant remains unstable and is removed.
Return to Upper Molar Immediate Implant Similar Case Next Day Course 2 3 4 Xin Wei, DDS, PhD, MS 1st edition 10/27/2017, last revision 05/05/2018