

|
|
|
|
|
|
|
|
|
|
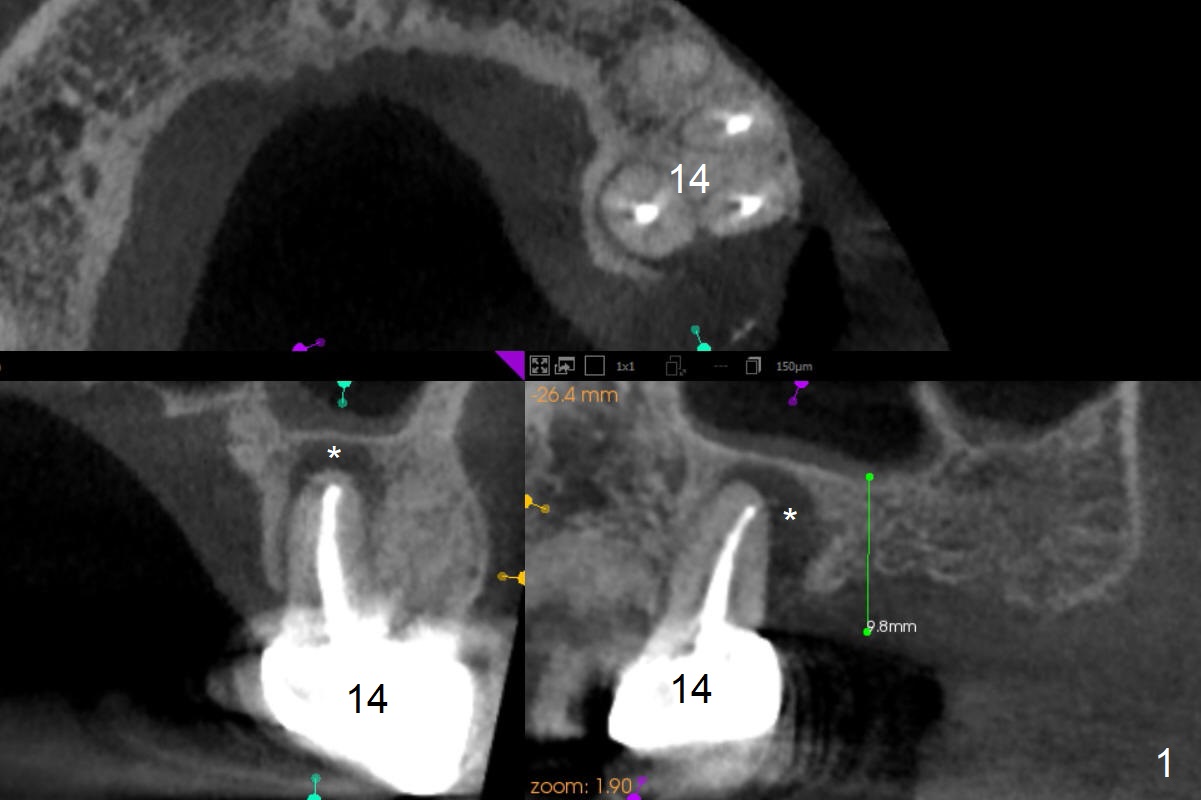
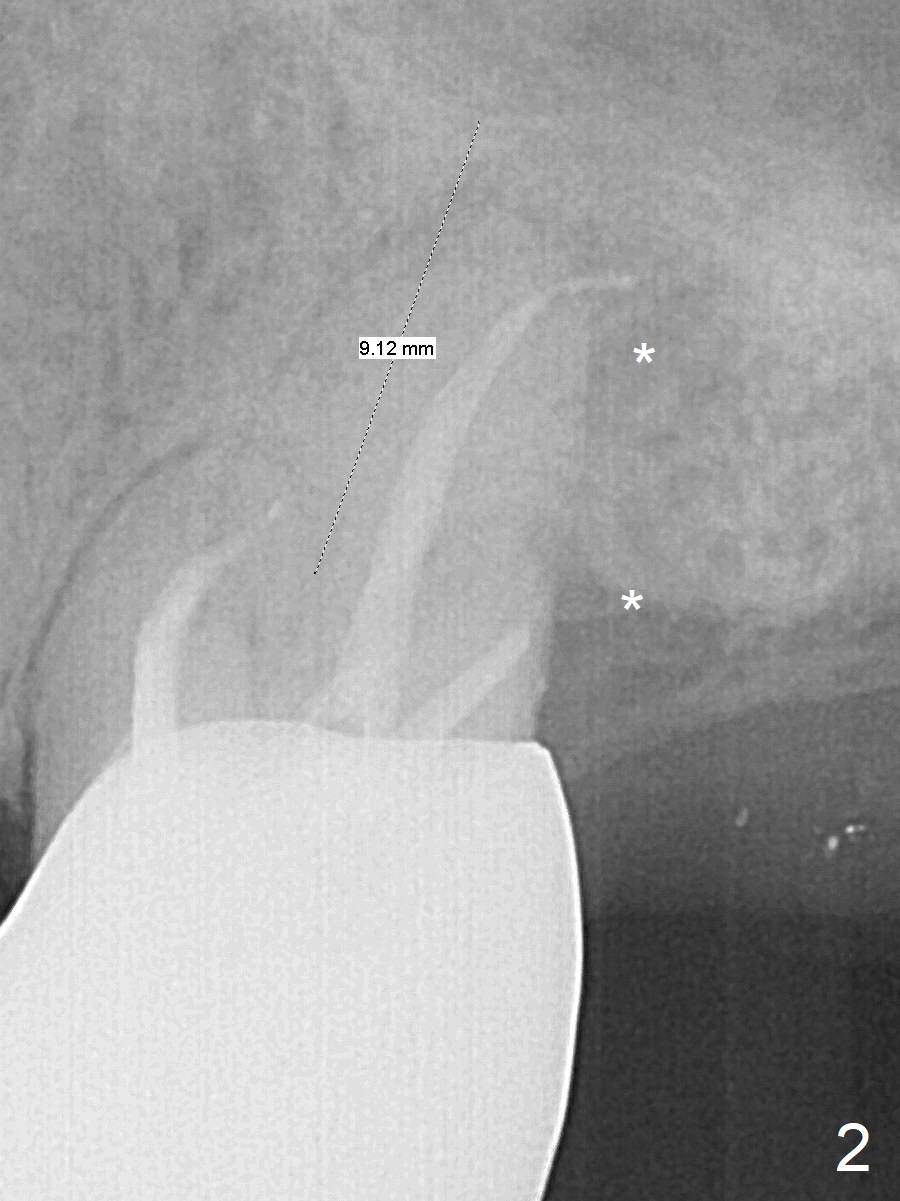
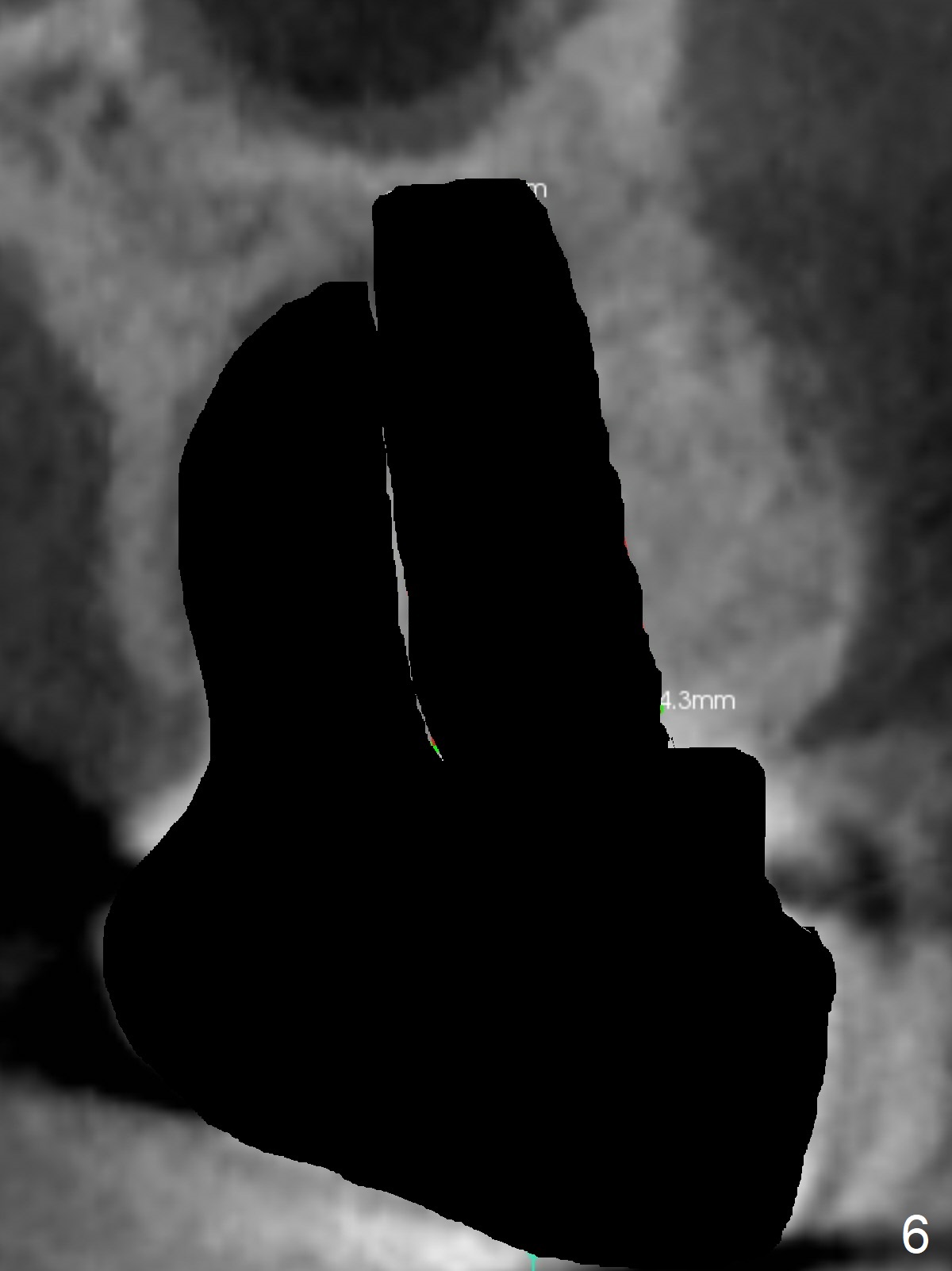
Persistent Radiolucency Post RCT
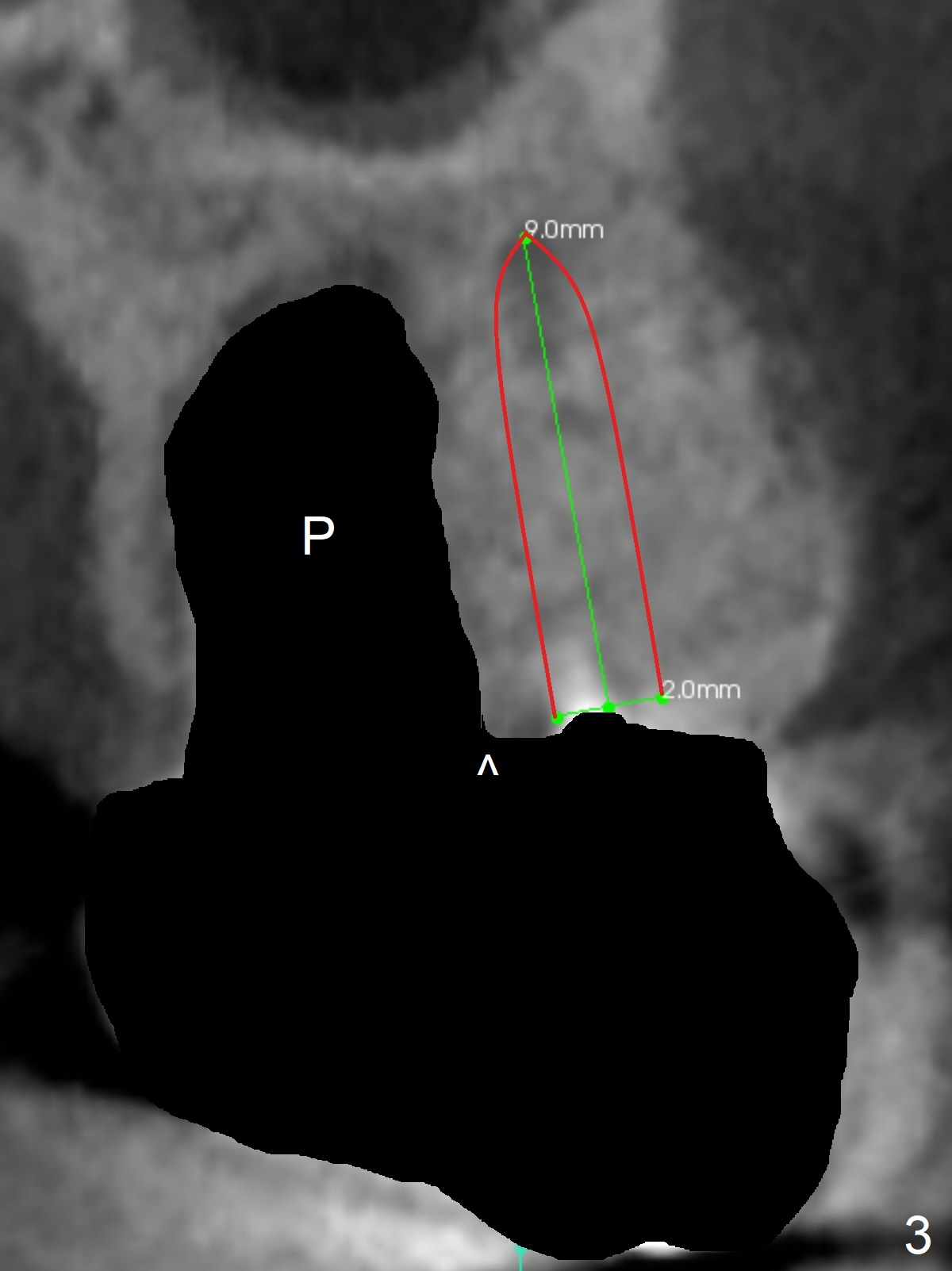
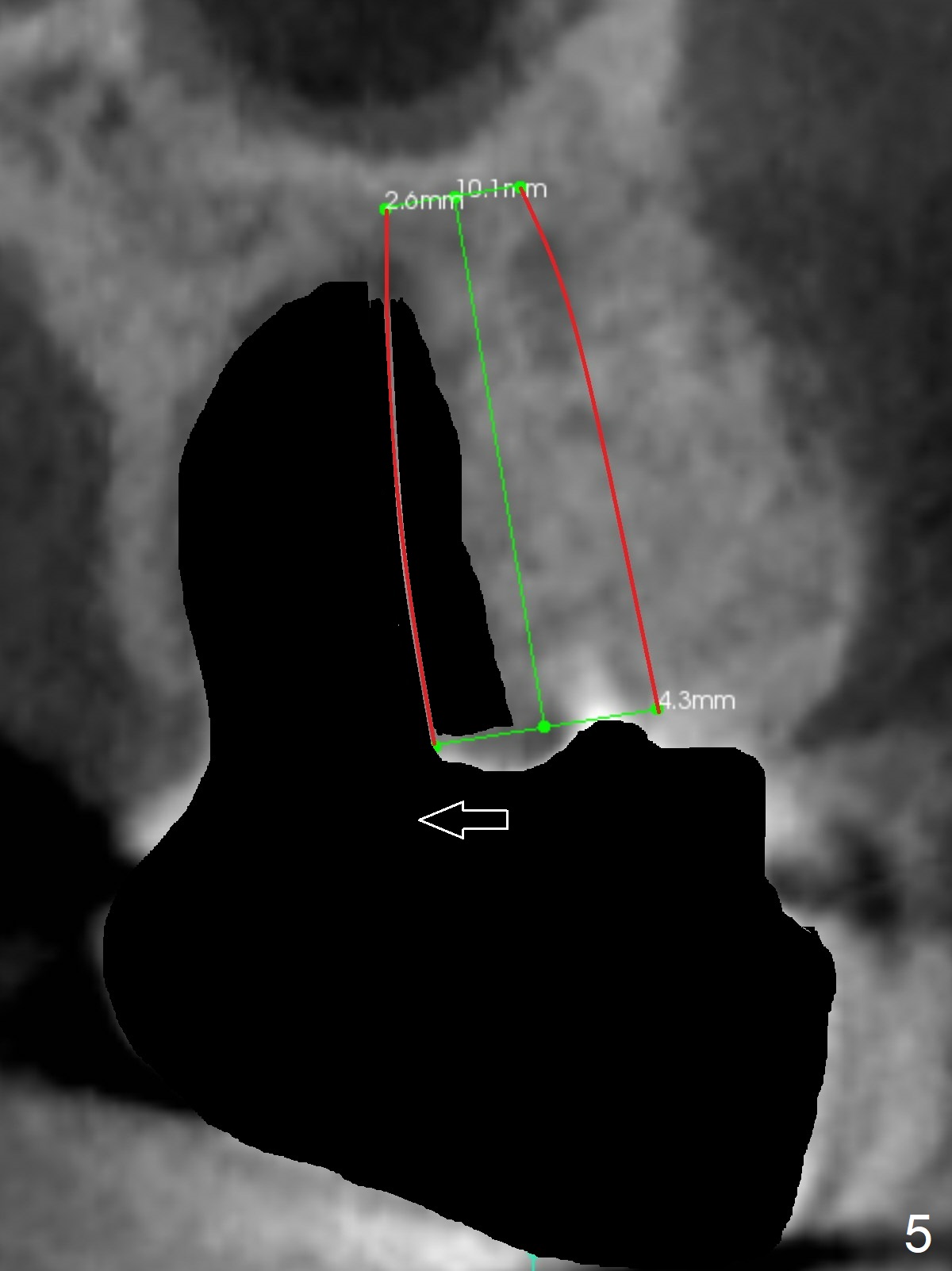
A 53-year-old man cannot chew on the left side with distal abscess in spite of RCT for #14 (* in Fig.1,2 (taken 11 ad 21 months postop, respectively)). After extraction (Fig.3 (CBCT coronal section) black area), start osteotomy with 2 mm drill (red outline) in the septum buccal to the palatal (P) socket). Following 2 mm drill removal (Fig.4), use 4.3 mm Magic Drill (red outline) for ~ 9 mm. When the osteotomy is being done, the osteotomy most likely shifts palatal (Fig.5 arrow) because of thin bone palatally. When the MD is removed (Fig.6), use Magic Sinus Lifter (Fig.7 pink) for sinus lift (arrow). The implant is to be 5x11 mm or larger. Because of the distal defect (Fig.1,2), start osteotomy mesially. Take Alginate impression before surgery for possible orthodontic treatment. Since bone density is high, use higher voltage and longer time for X-ray.
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS,
Metronidazole
Xin Wei, DDS, PhD, MS 1st edition 09/14/2017, last revision 08/15/2018