

|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
Immediate Provisional Completely Seals Socket
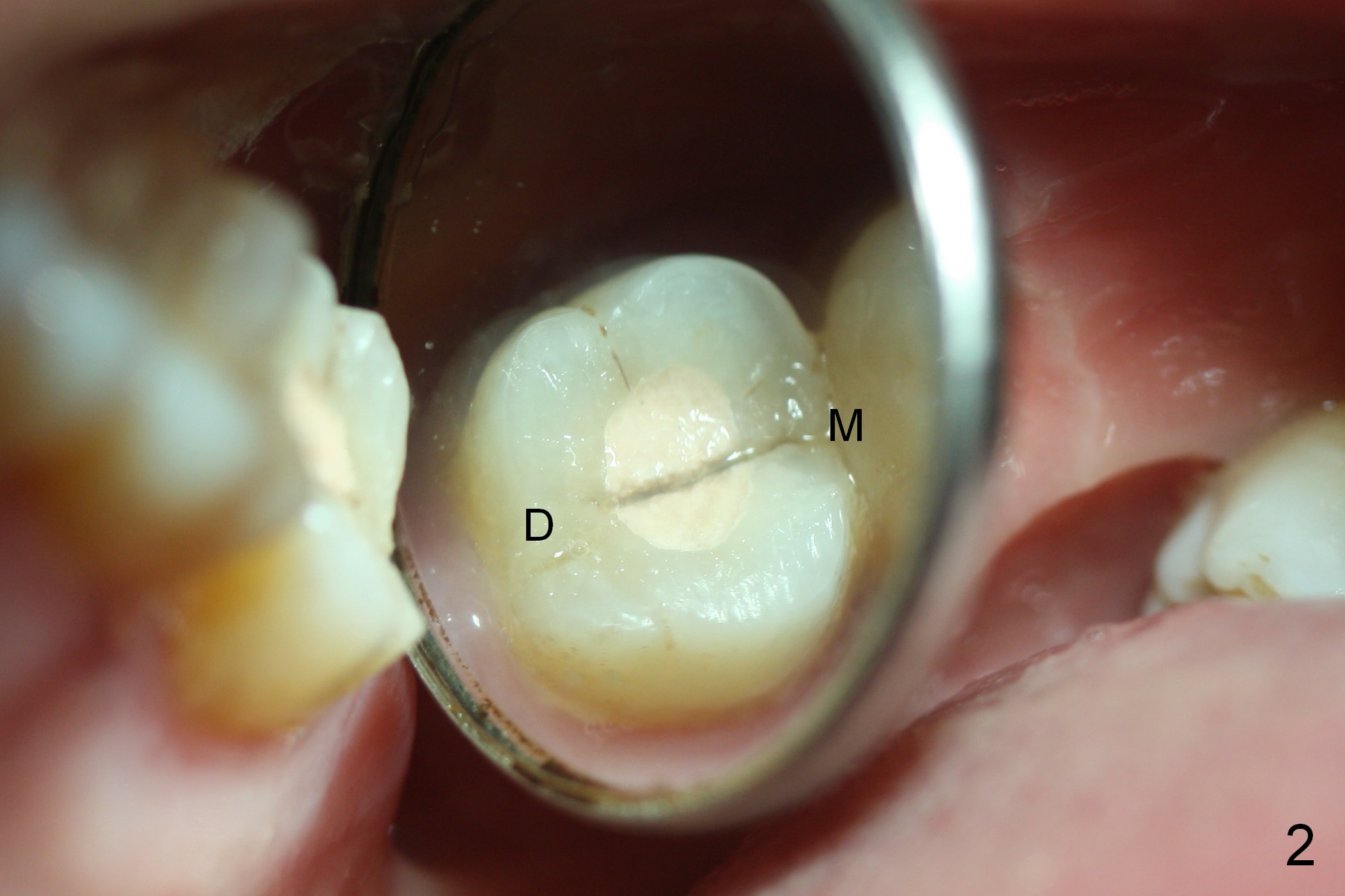
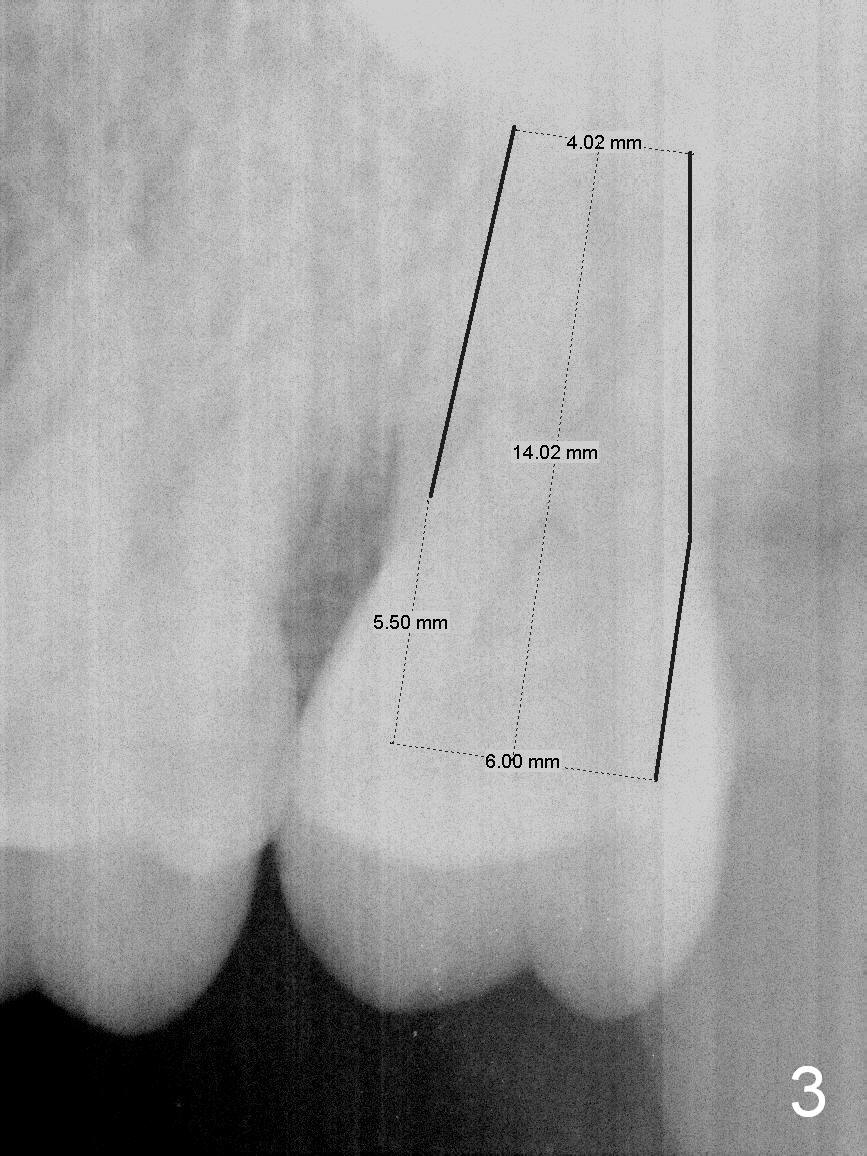
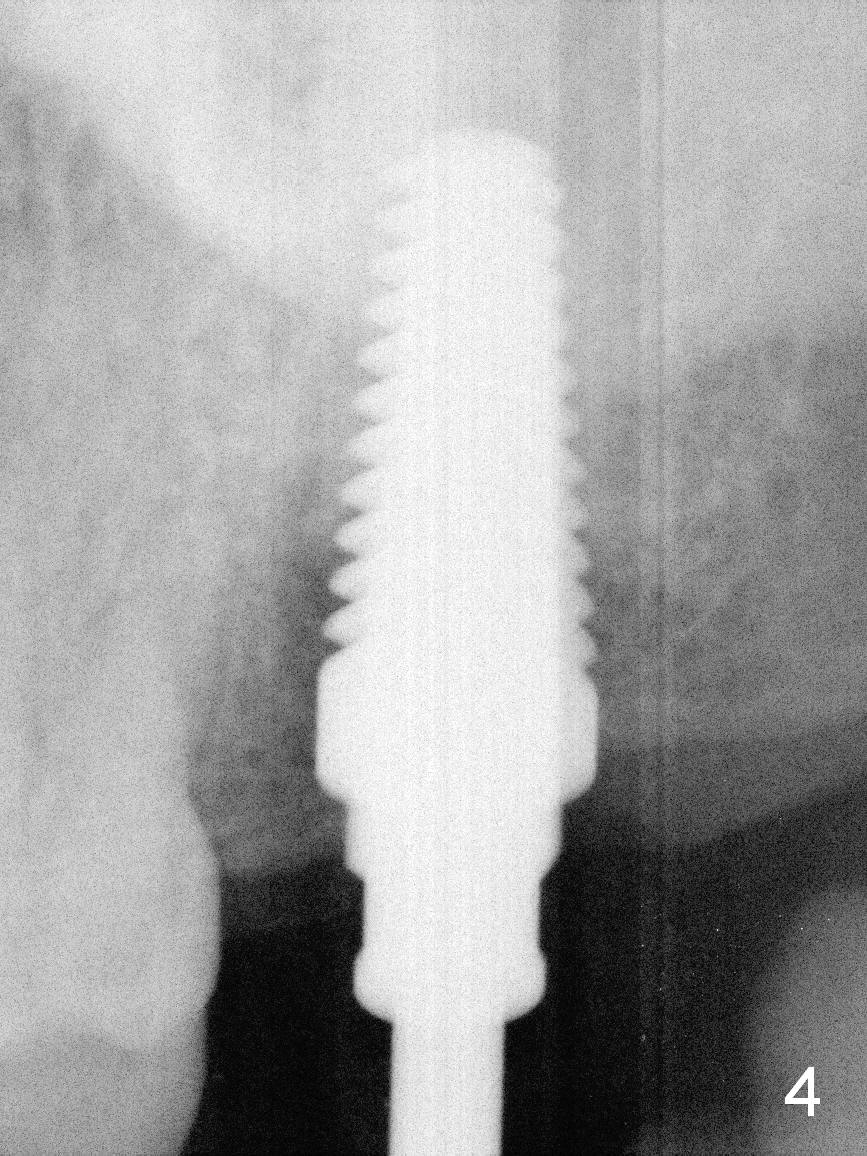
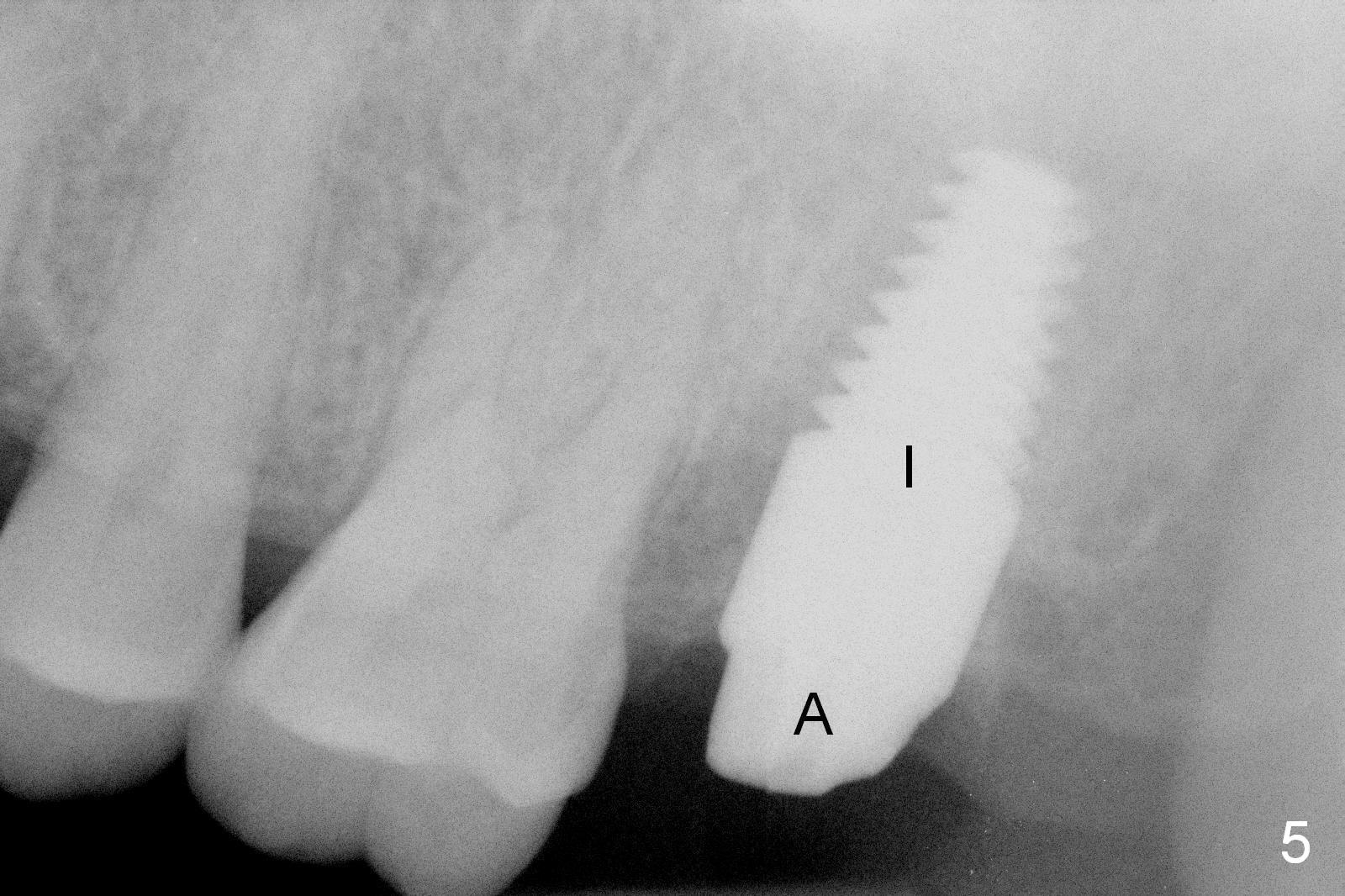
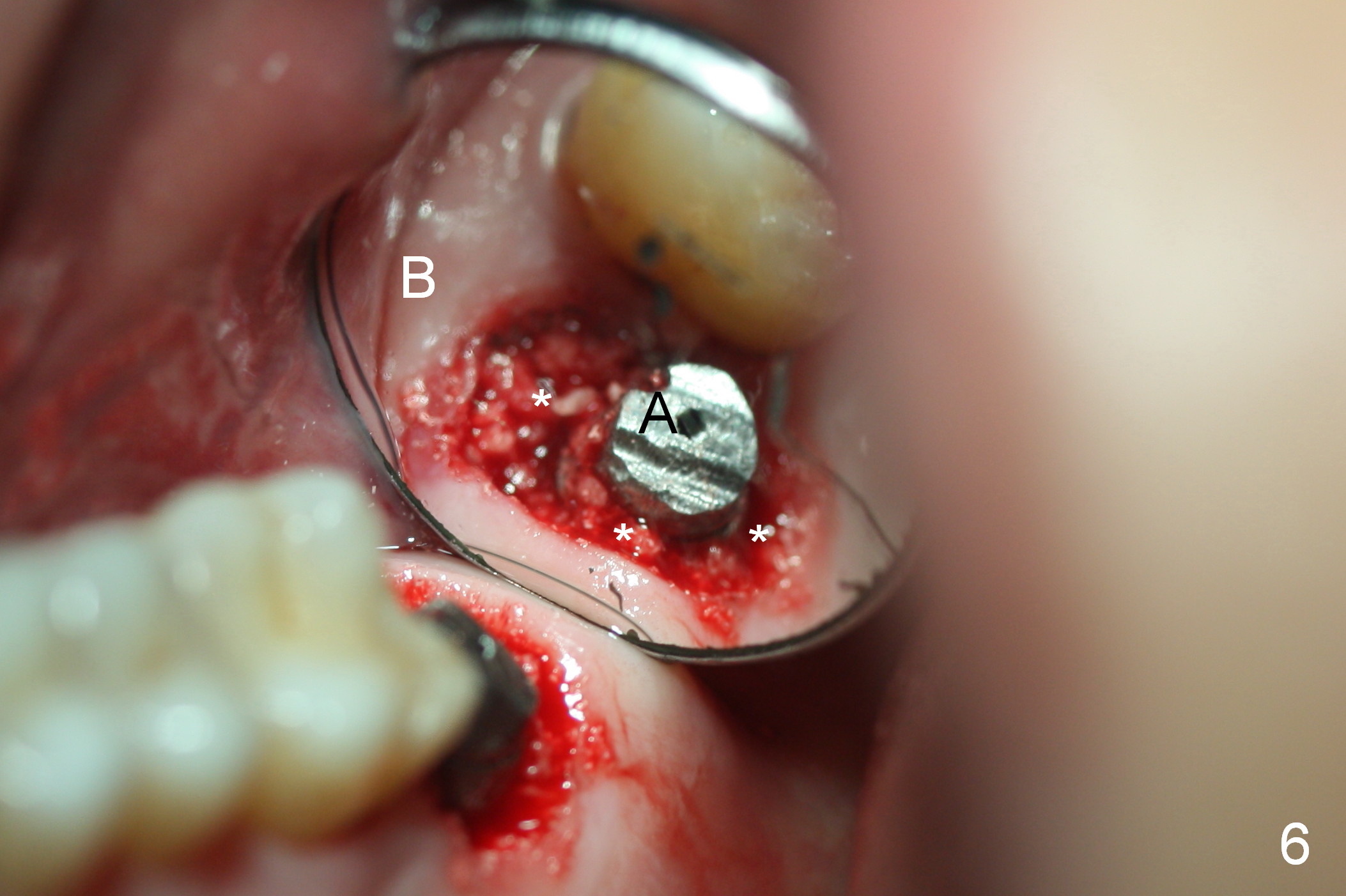
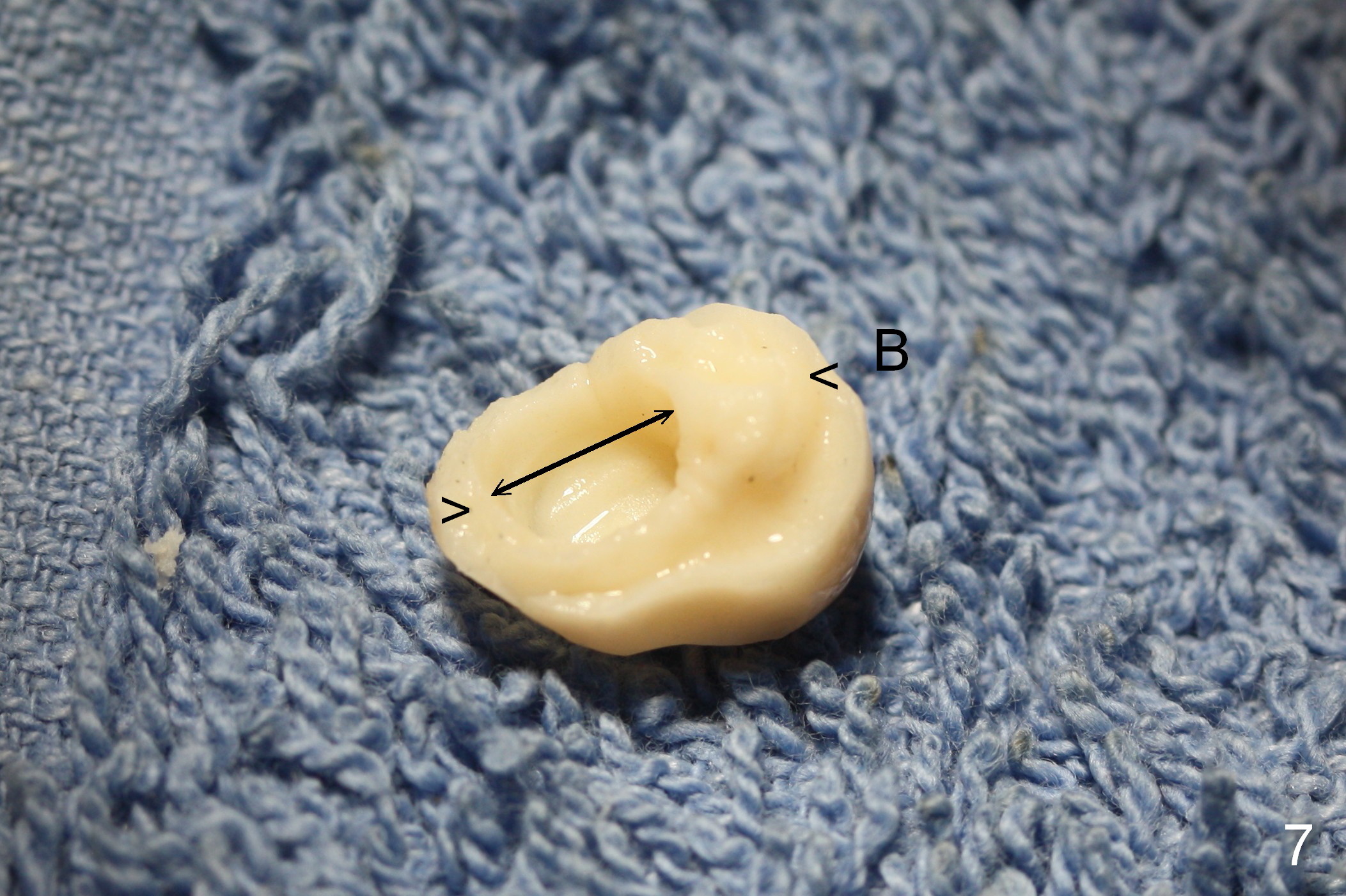
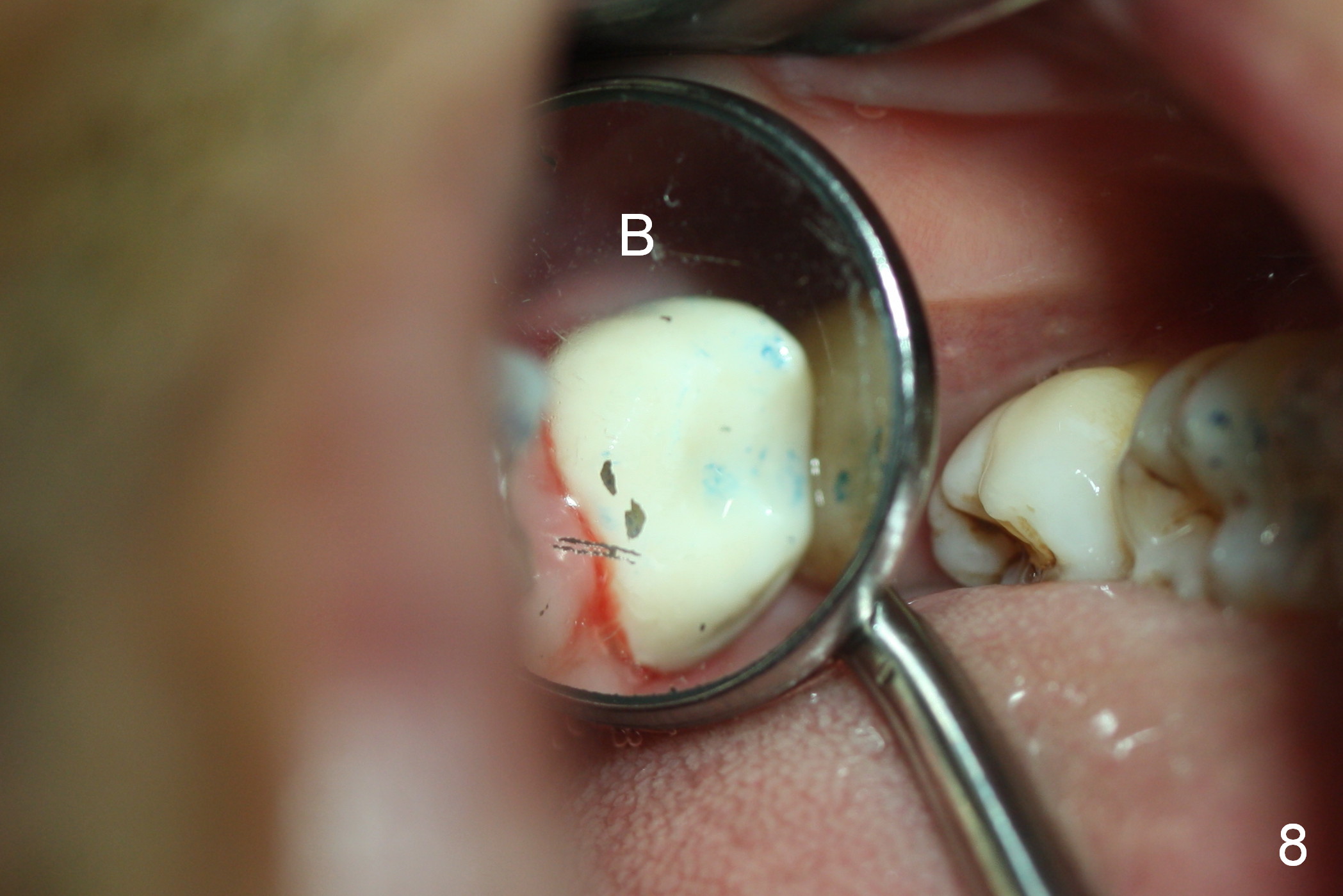
A 50-year-old man (TK) had sign & symptom of crack tooth at #15 (Fig.1) and chose to have root canal therapy done by a specialist. One month later, he returns for crown; exam reveals a crack line mesiodistally (Fig.2). The patient agrees to have immediate implant (Fig.3 design: 6x14 mm). The buccal roots fracture upon luxation. Osteotomy starts in the septum with a 2 mm pilot drill and deviates to the palatal socket, followed by 2, 3, 4 mm tapered osteotomes. A series of taps are placed: 6x17 mm one achieves stability (Fig.4). When the latter is removed, there is no sign of sinus air leakage. A 6x14 mm implant (Fig.5 I) and a 5x3 mm abutment (A) are placed. After abutment height adjustment, an immediate provisional is fabricated. Allograft with Osteogen is placed in the remaining sockets and gaps (Fig.6 *). Fig.7 shows the inner side of the provisional with double arrows indicating the dimension of the abutment, whereas arrowheads the dimension of the socket buccopalatally. When the provisional is cemented (Fig.8 P), it completely seals the socket. As long as the provisional stays, bone graft will not be lost.
The patient returns for follow up 1 week and 1 month postop. The provisional remains in place. It is removed for margin modification 1 month postop: the bone graft having been apparently incorporating into the socket concentrically (from periphery of the socket to the implant) (Fig.9).
The provisional fractured and lost 4 months postop when the patient returned for definitive restoration. The gingiva does not seem normally when gingival retraction cords are packed.
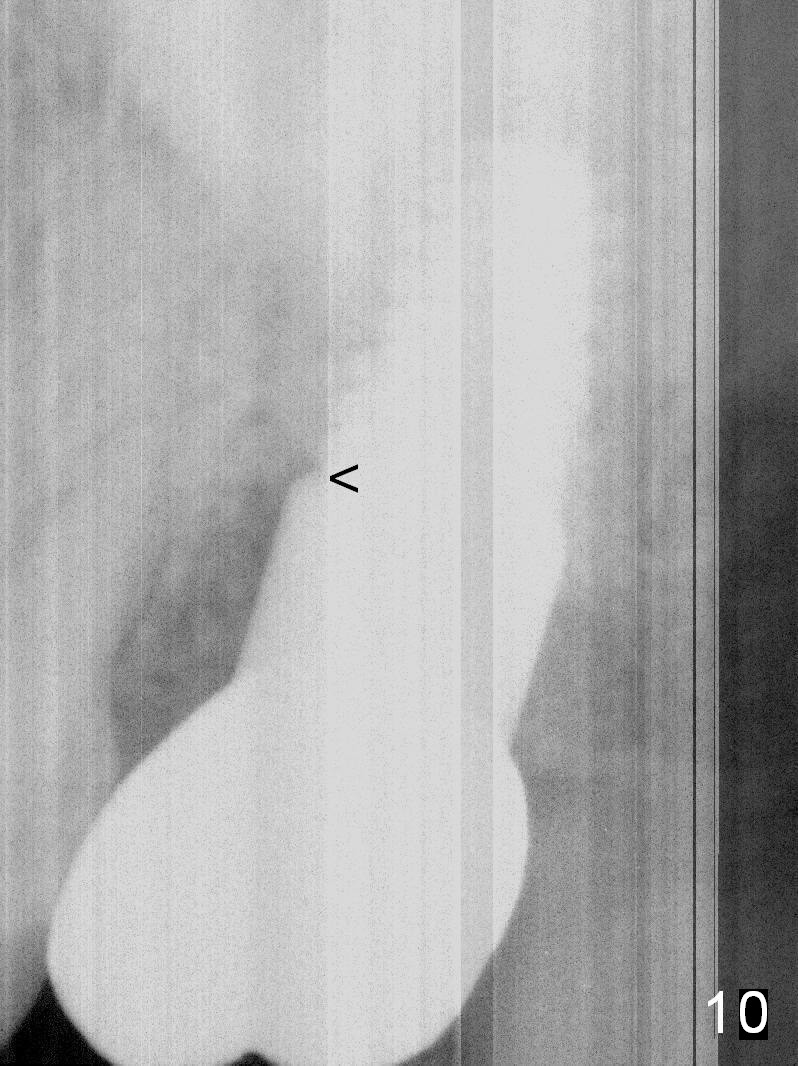
Three months post cementation (10 months postop), the patient complains of gingival bleeding while masticating. There appears bone loss mesially (Fig.10). The gingiva appears erythematous around the implant. Water Pik is recommended. It is better not to process for final impression if there is minimal sign of infection.
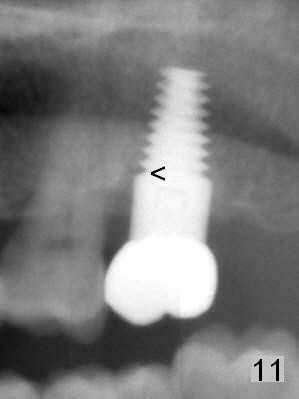
In fact the oral hygiene improves by brushing. Six months later, the gingiva is healthy without symptoms, although the mesial bone loss persists with seemingly mesial implant thread exposure (Fig.11 <). Bone loss is more severe in the proximal area. There are 4 potential solutions: place implant low, pack more bone graft and remove the immediate provisional once the socket has heals. The implant should be smaller so that it does not compress the crestal bone, which is more likely resorbed under insertion pressure.
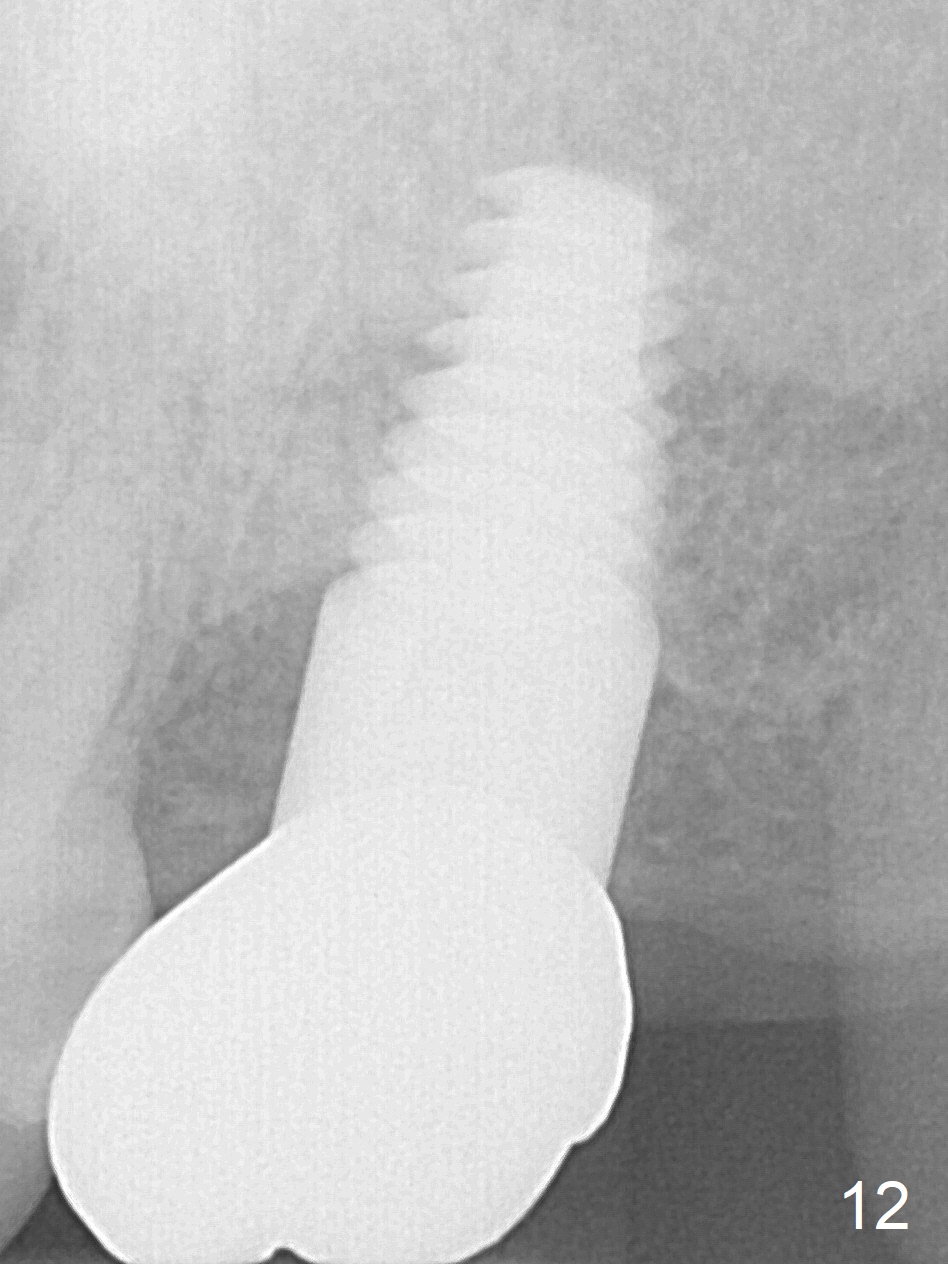
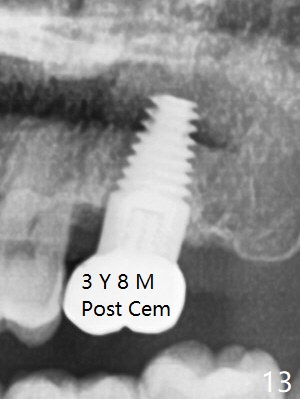
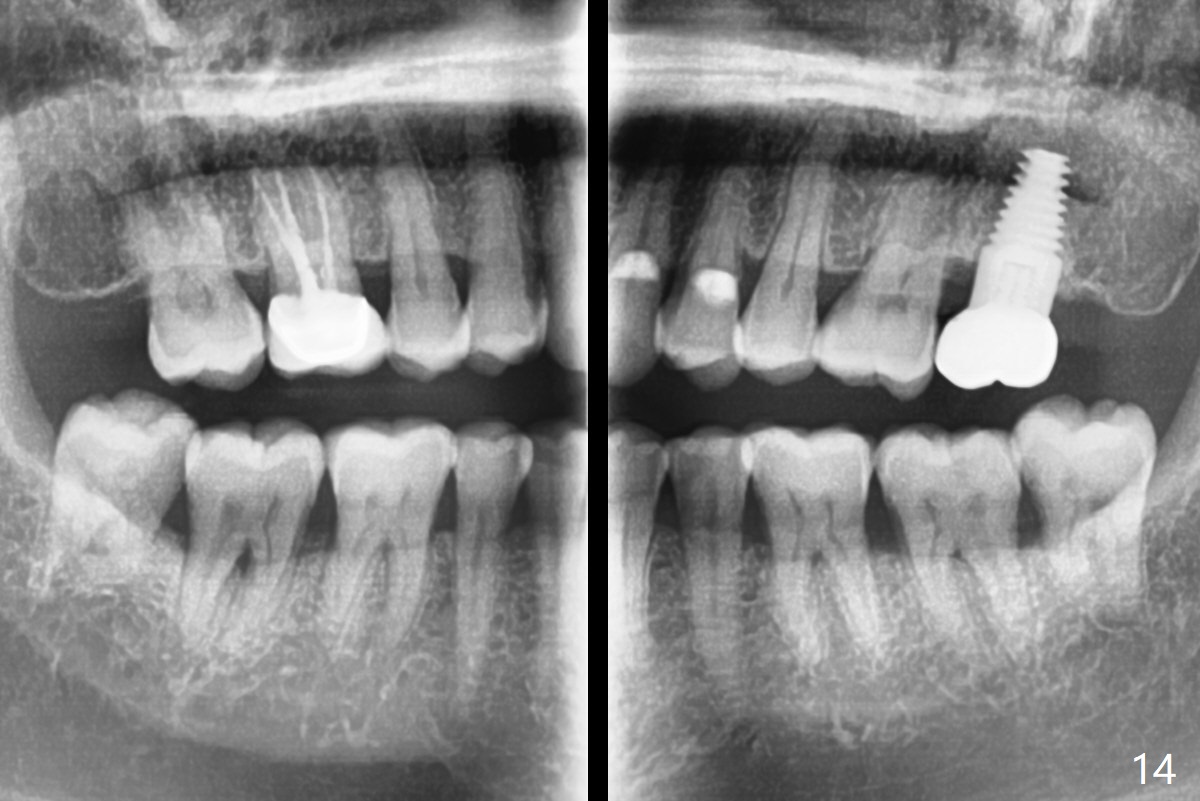
There is no bone loss 17 months post cementation (Fig.12). The patient reports that he has to keep cleaning well to prevent discomfort locally. Clinically, the gingiva is healthy around the implant crown. No bone loss is around the implant 3 years 8 months post cementation (Fig.13), but the natural teeth are not so fortunate (Fig.14).
Return to Upper Molar Immediate Implant,
Antibiotic Study,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 08/13/2015, last revision 09/28/2019