

.jpg)
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|
|
|
Keep Sinus Floor Intact
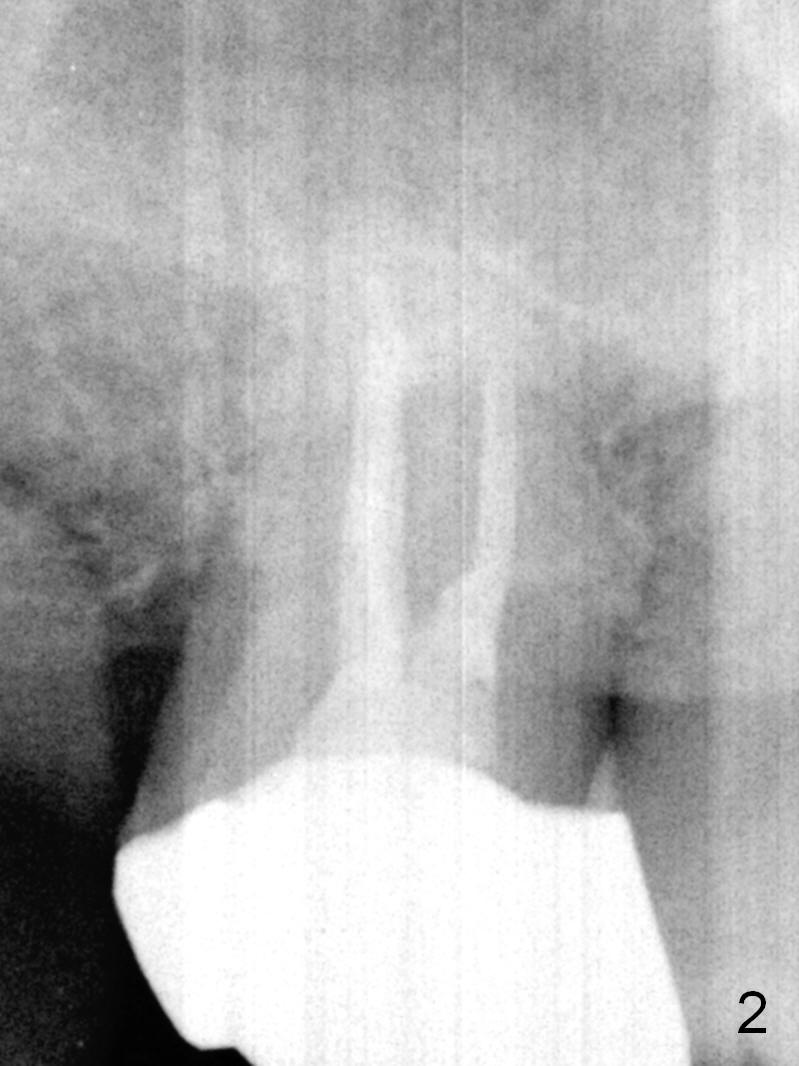
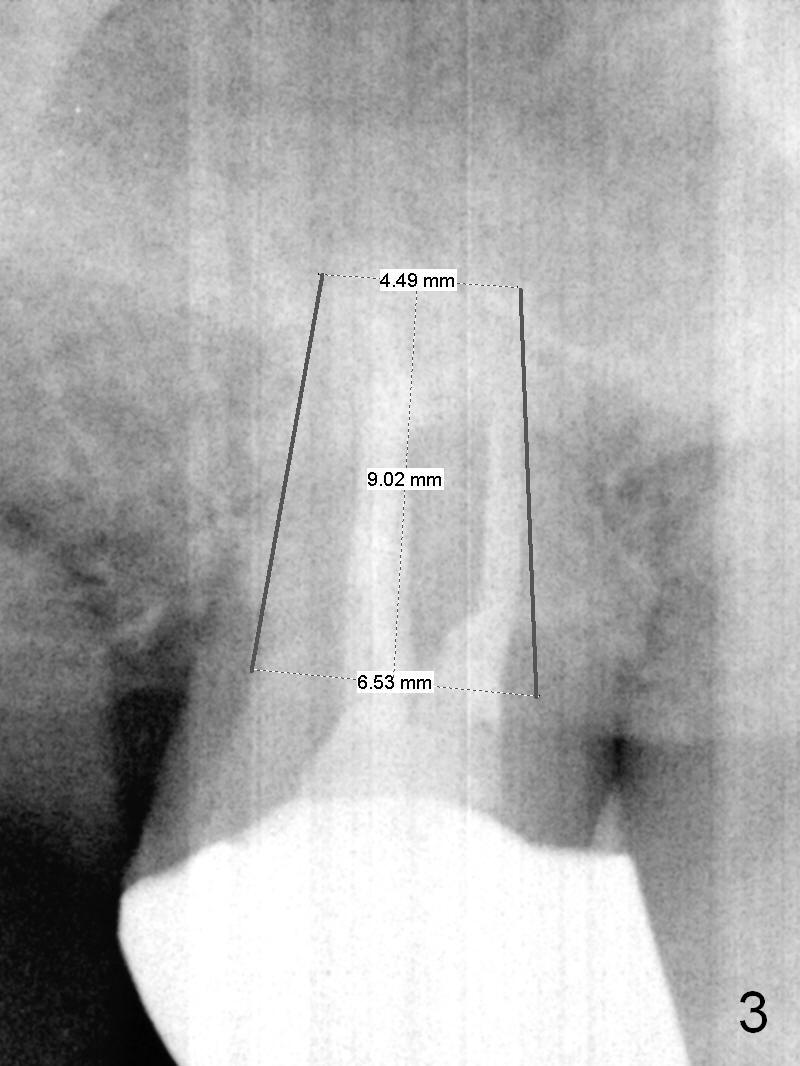
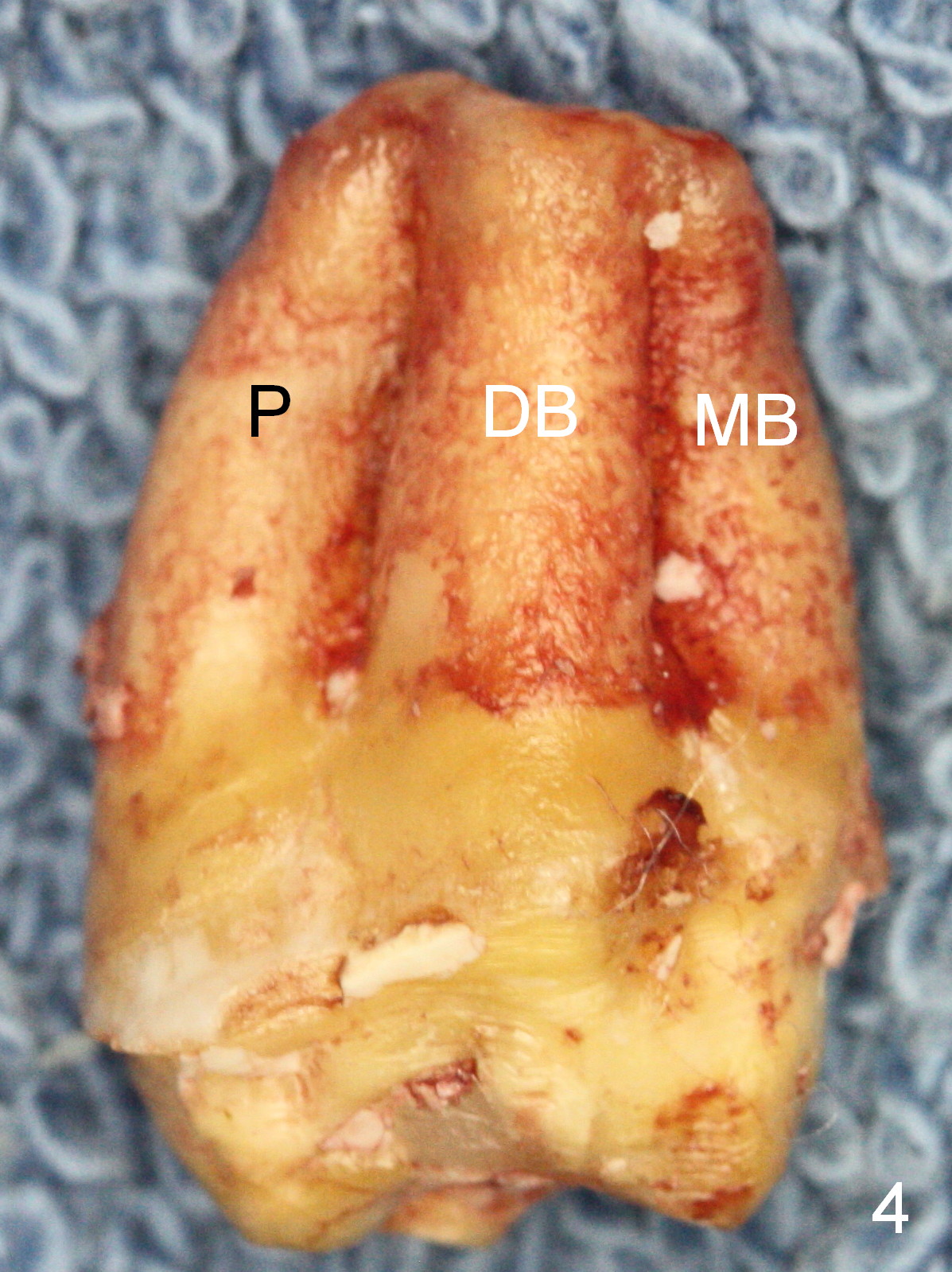
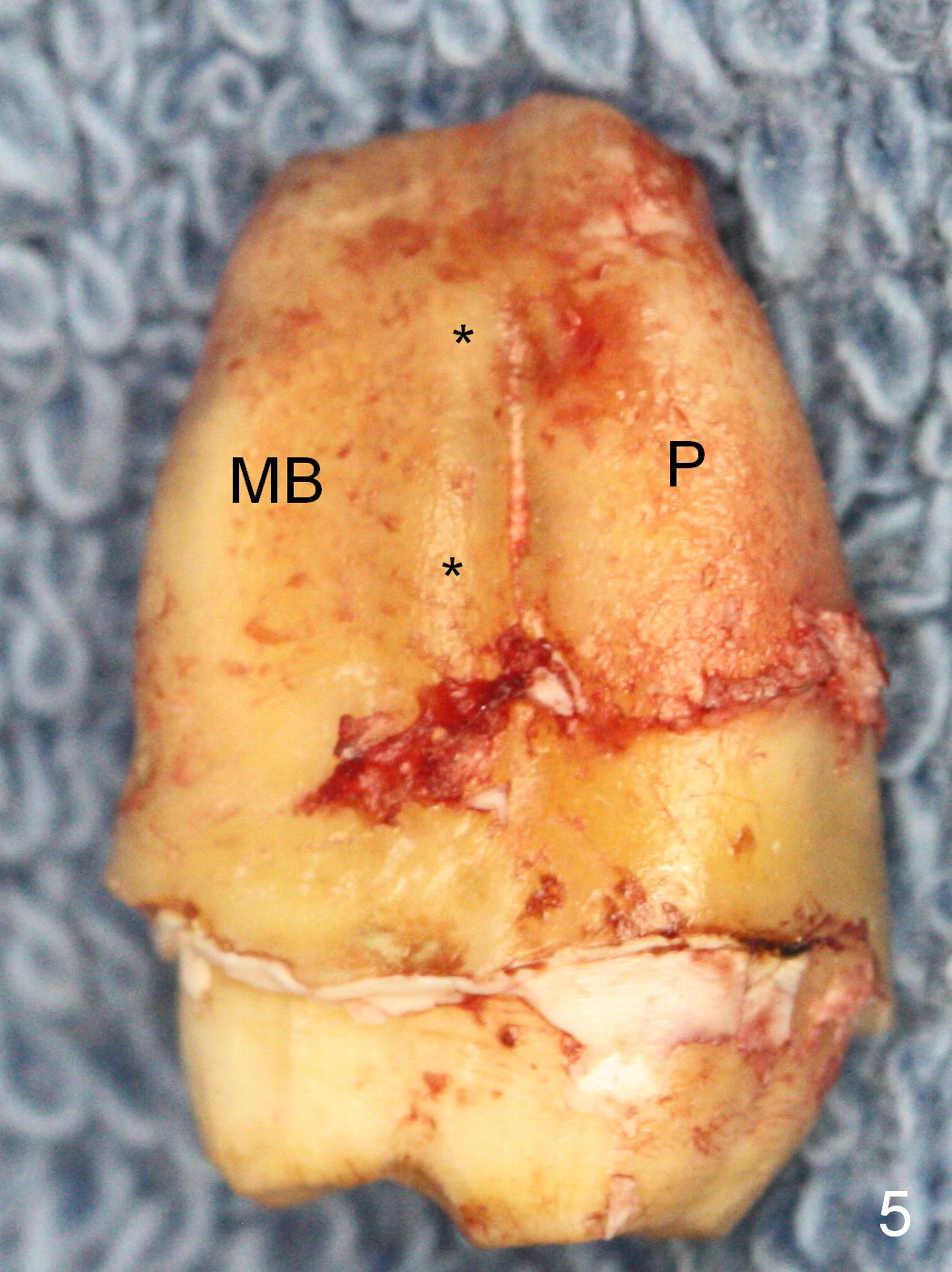
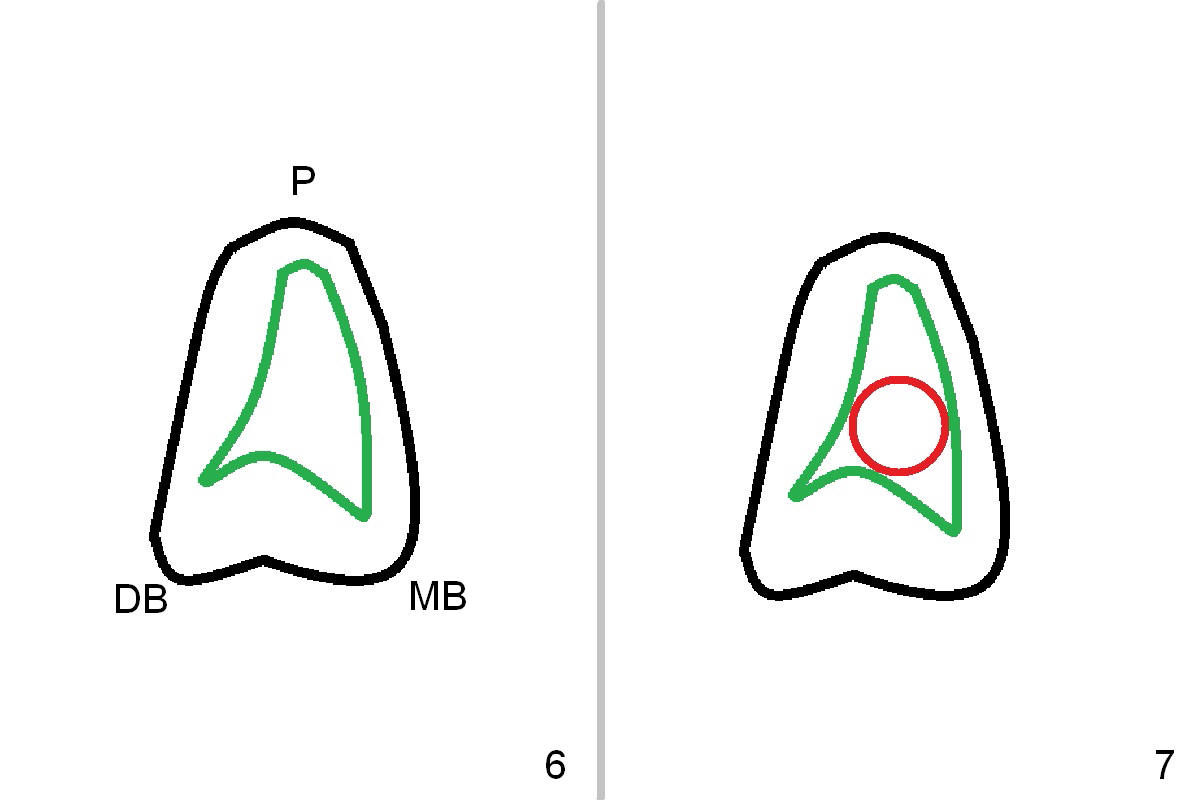
A 52-year-old man has had mild cold sensitivity for the last 3 years since RCT was done at the tooth #2 (3 canals, MB2 not found, Fig.1 (preop), 2 (taken today, pain more severe)). After discussion of treatment options (including RCT retreat), the patient chooses extraction and implant. The planned implant is 6.5x9 mm (Fig.3). As expected, the 3 roots are fused (Fig.4). The socket is single and triangular (Fig.6 green outline (black one: gingival margin)). What is not really expected is the presence of the possible MB2 canal (Fig.5 *). The mesiodistal width of the buccal roots and palatal one are 6.5 and 4.5 mm, respectively. The diameter of the planned immediate implant is estimated to be 5 mm. The socket depth is 11 and 13 mm to the crest and the gingiva, respectively. After use of Magic Expanders (ME) from 3.0-4.3 mm for sinus lift, a 5x11 mm dummy implant is placed. The implant (Fig.7 red circle) has 3 pointed contact so it is stable, but it is placed apically (Fig.8). After removal of the dummy implant, allograft is placed (.5-1.5 mm) before insertion of a 5.5x11 mm implant with satisfactory stability (Fig.9). Postop, the patient reports light bloody nasal discharge with bone graft. Ideally with the narrow mesiodistal socket, it is unnecessary to penetrate the sinus floor with ME. A 5x9 mm dummy implant should have been placed with well-controlled implant placement depth. It is followed by inserting an implant .5 mm larger for the maxilla. IBS implants are easy to achieve primary stability. Insertion torque of 20 Ncm is sufficient to load abutment (5x4(4) mm) and immediate nonfunctional provisional.
Two months post op, the temporary crown has slight mobility. The pair abutment is changed to a 6x2 mm healing abutment.
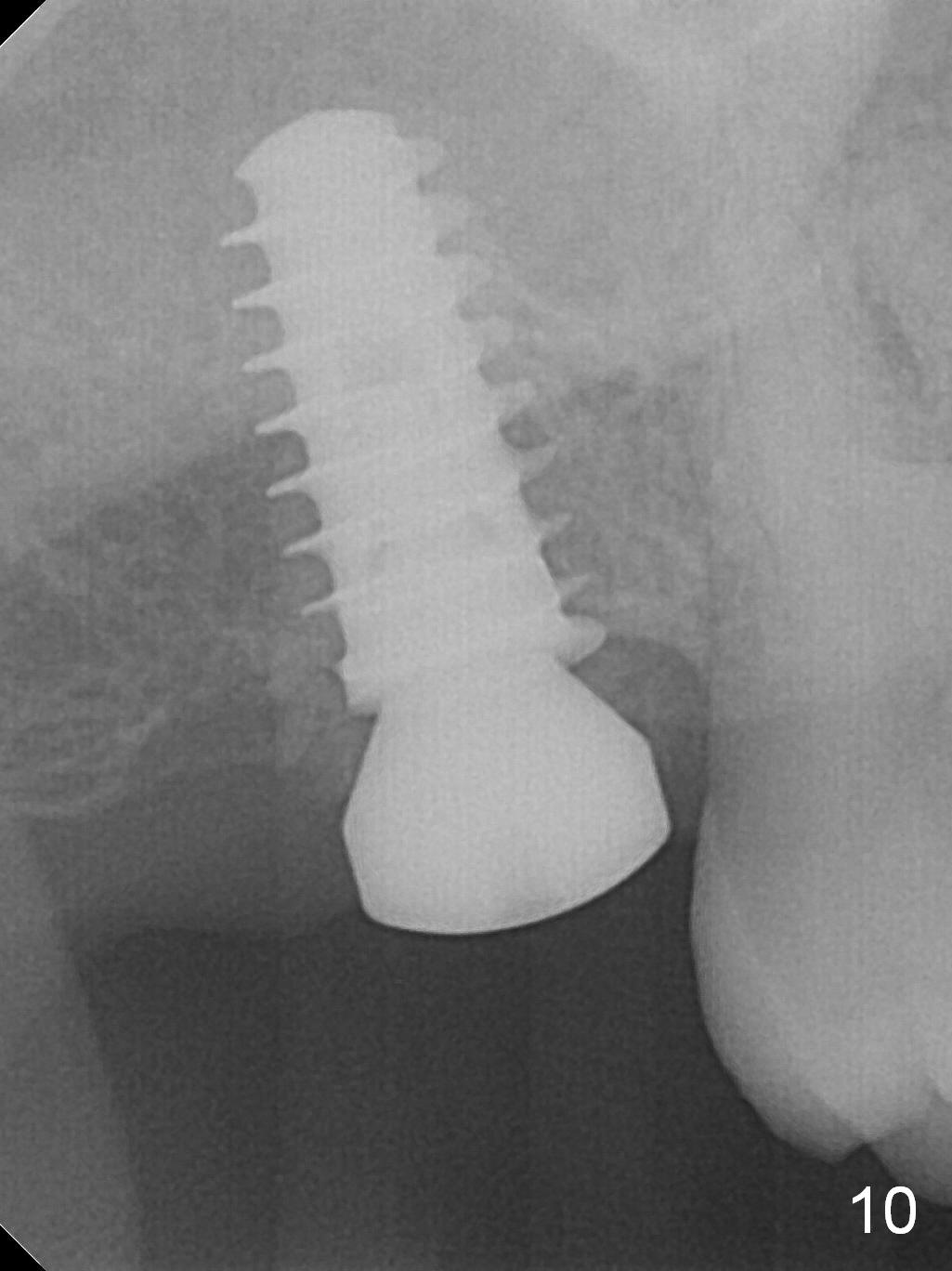
Five months post op, the healing abutment has mobility with light tenderness. The space between the bone and implant is larger than normal (Fig.10).
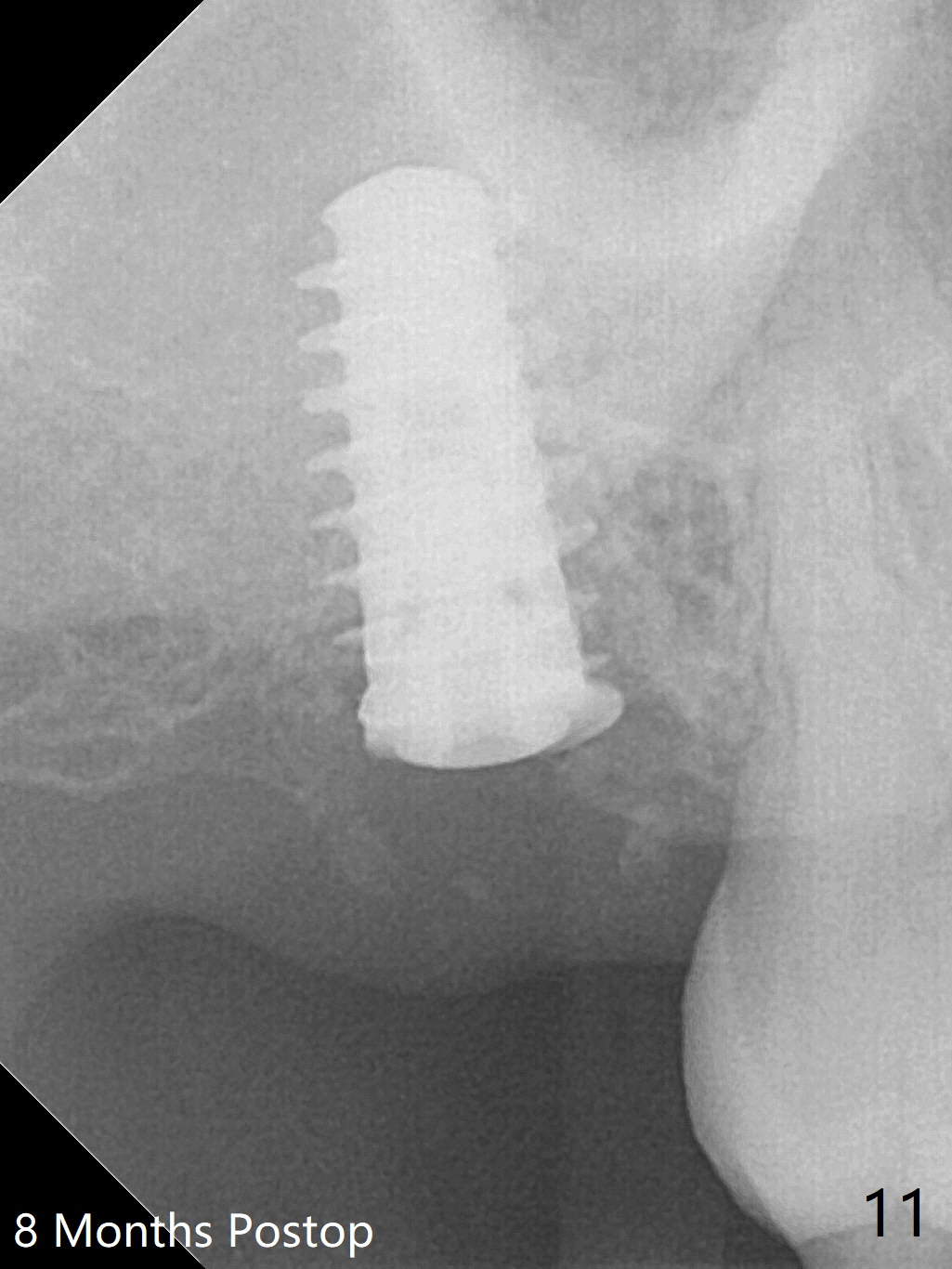
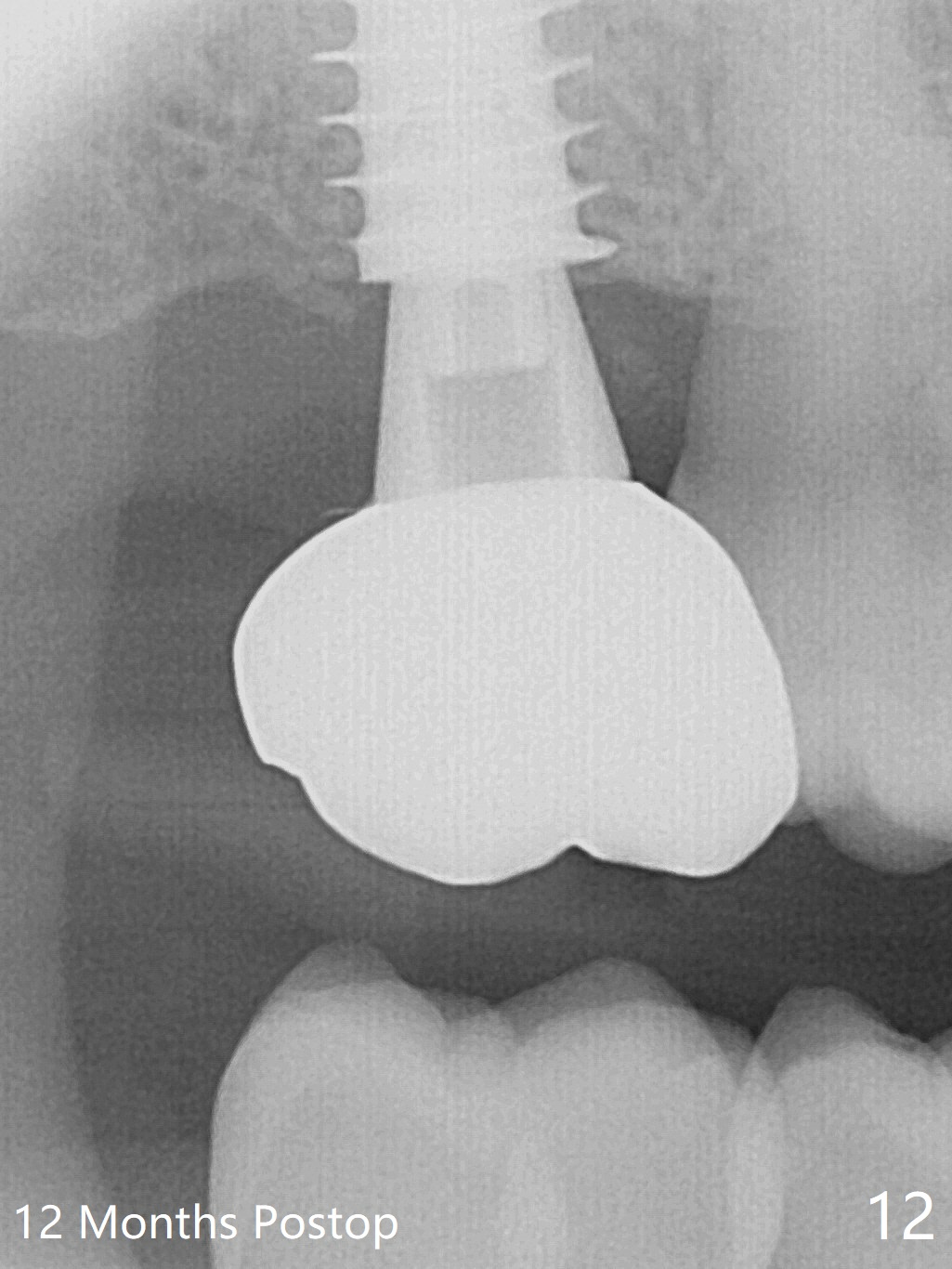
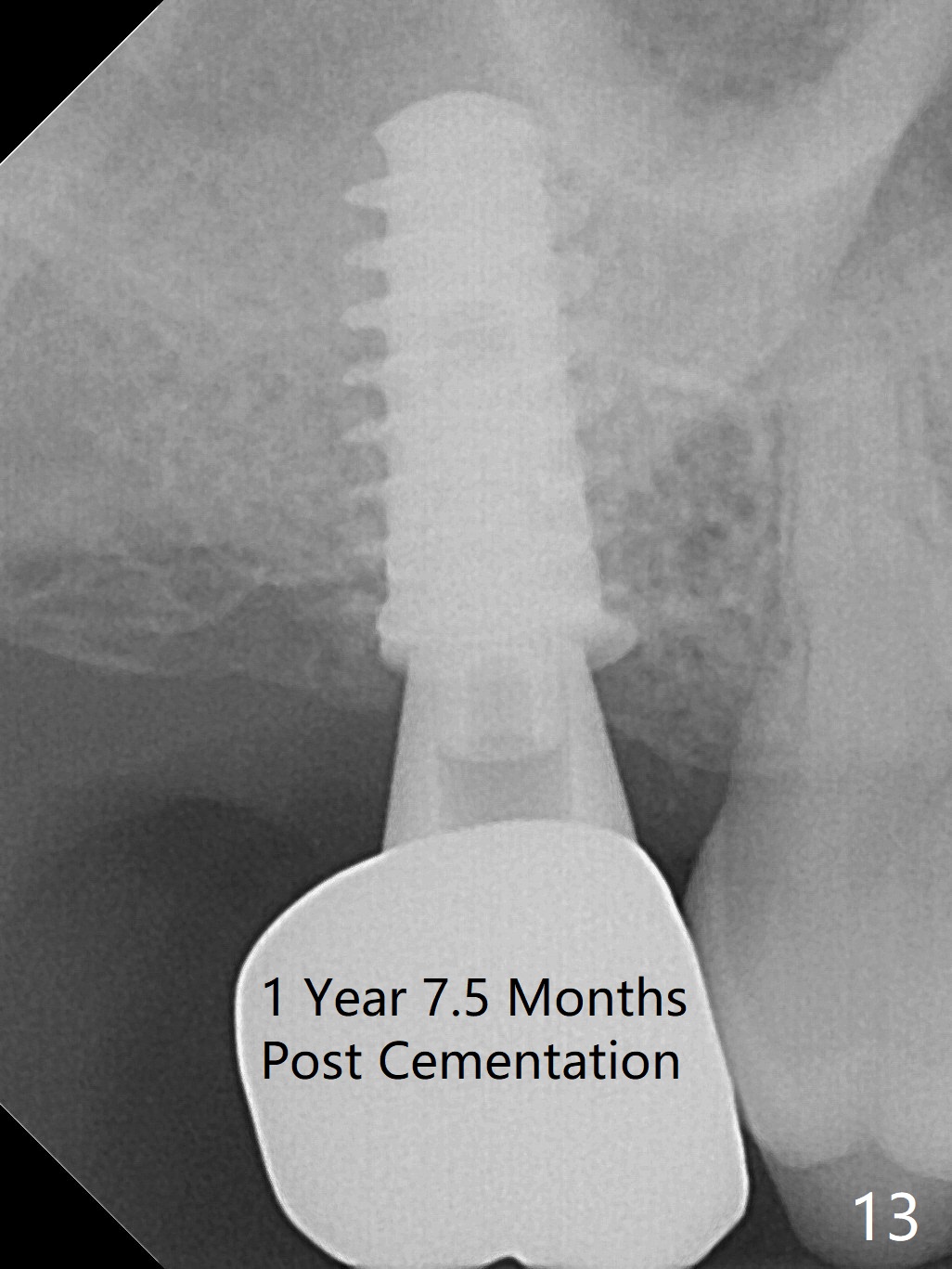
The implant is stable with the healing abutment 8 months postop (Fig.11). There is definitive sign of osteointegration 12 months postop (3 months post cementation, Fig.12). The patient is pleased to have the implant for 1 year 7.5 months post cementation (Fig.13).
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
Metronidazole,
Dr.
Wang's Response
Xin Wei, DDS, PhD, MS 1st edition 10/19/2016, last revision 02/13/2019