





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Stick to Basic Principle
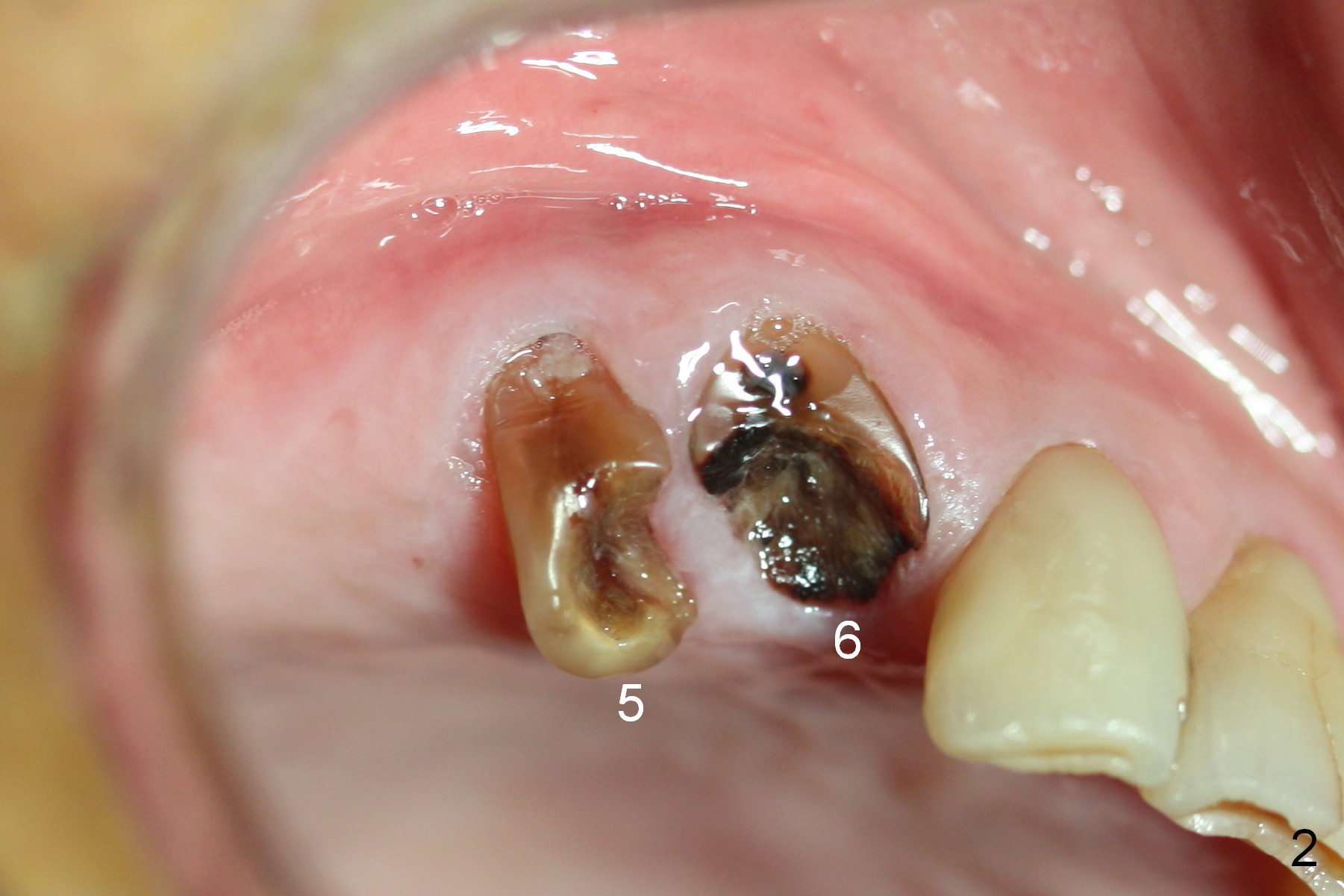
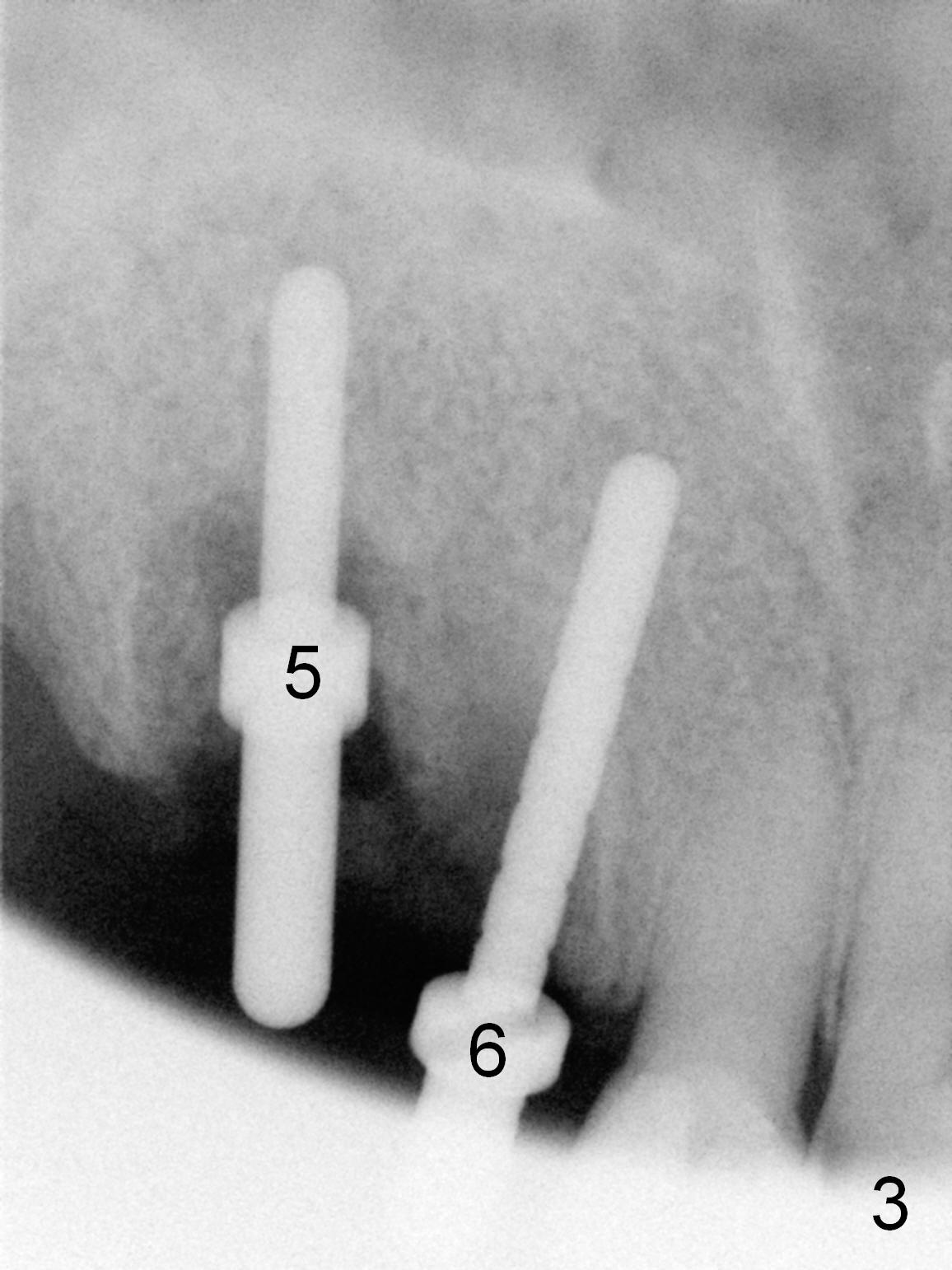
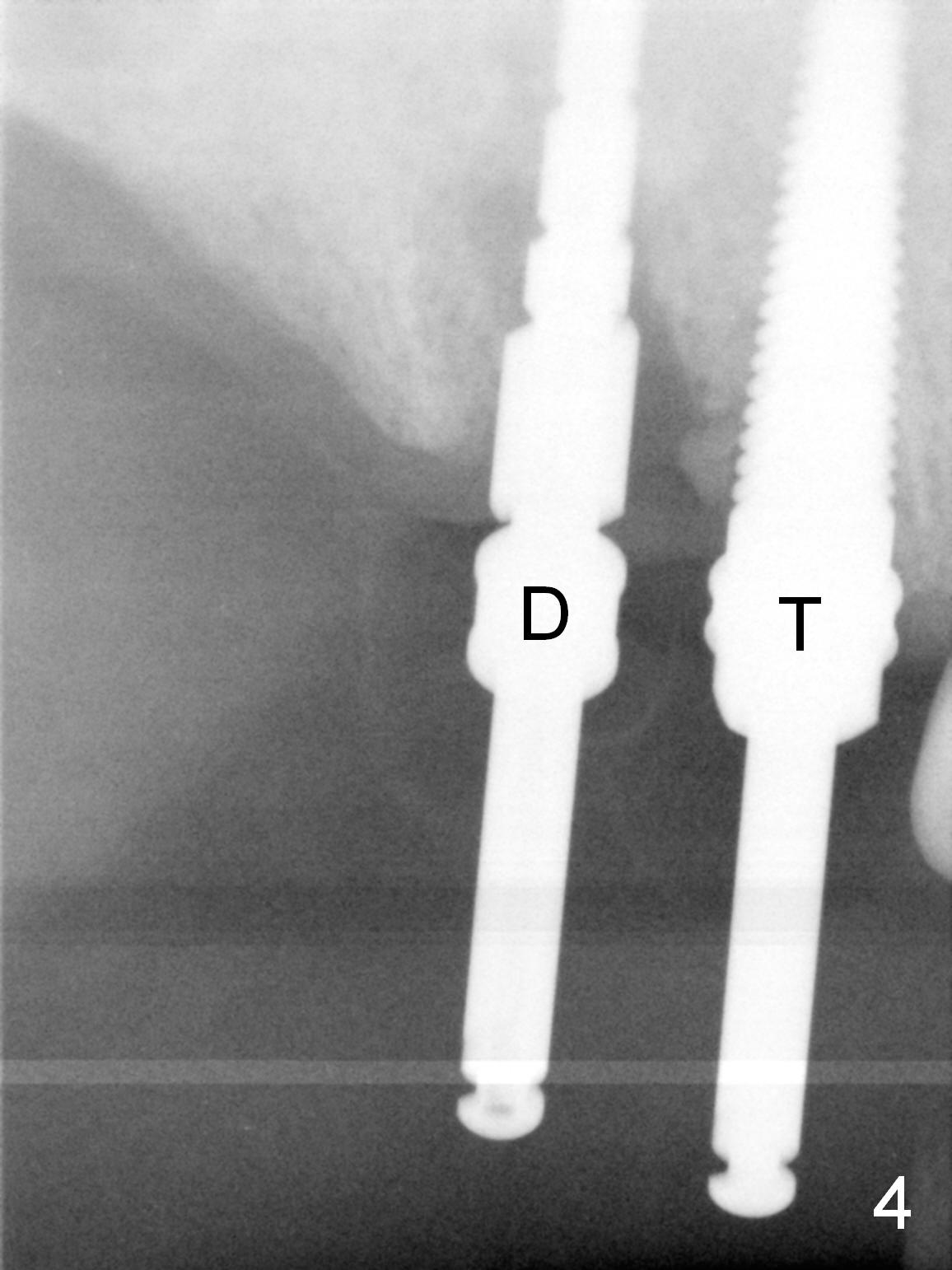
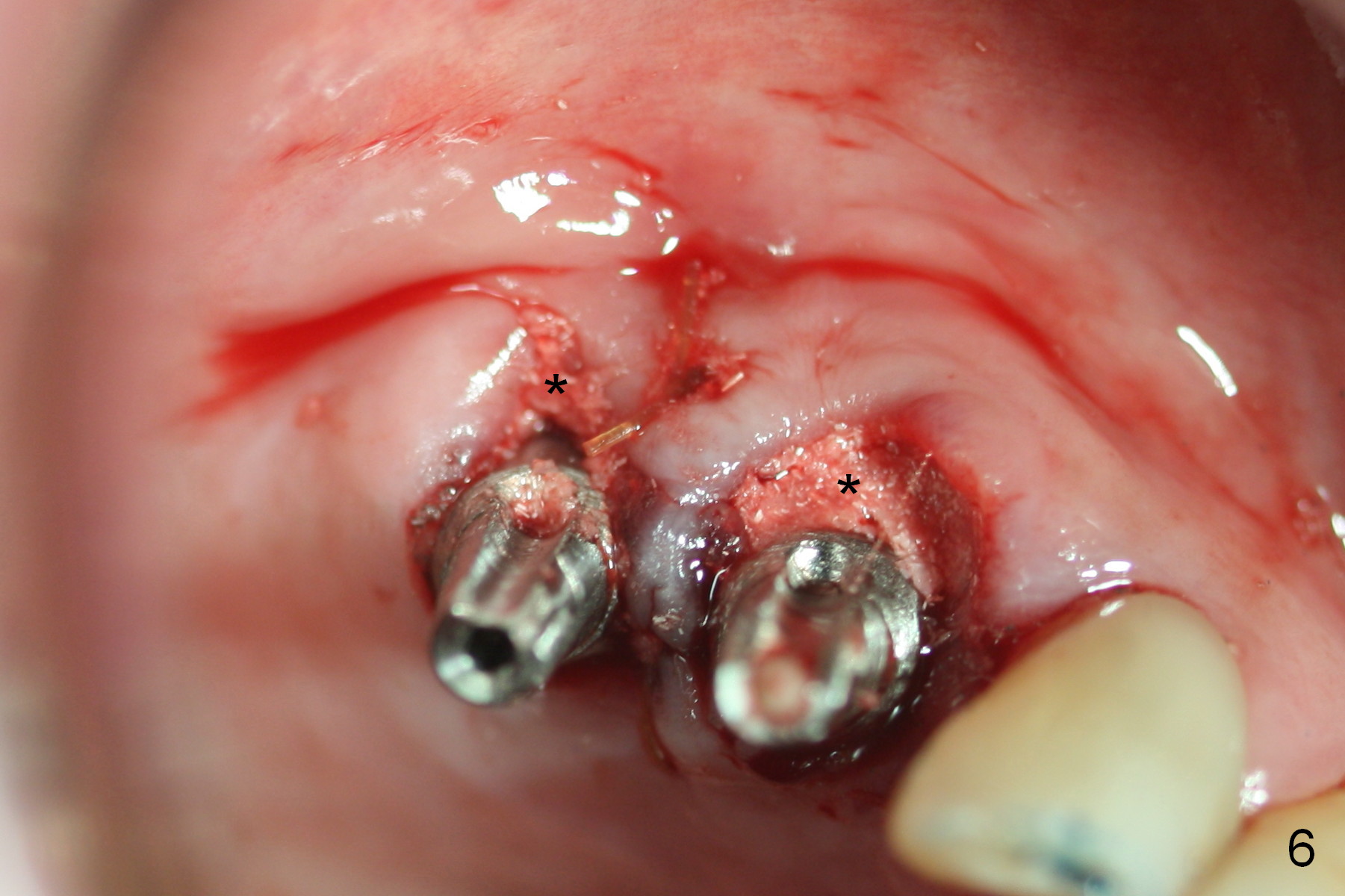
Several of CK's upper teeth (apparently in cross bite) are to be restored with implants (Fig.1). The first two are #5 and 6; note the oval roots (Fig.2). After extraction, and curettage, osteotomy starts in the palatal aspect of each socket. The 1st intraop PA shows that the trajectory at #6 is incorrect (Fig.3). After adjustment, osteotomies look parallel (Fig.4: D: 3.5x20 mm drill; T: 4.5x20 mm tap). This suggests how important it is to use parallel pins to check initial osteotomies for neighboring implants (Fig.3). The trajectory of the implants remains acceptable (Fig.5: 4.5x20 mm with insertion torque »60 Ncm); so is the position of the implants (as palatal as possible; Fig.6 (*: bone graft)). Immediate provisionals are fabricated in cross bite.
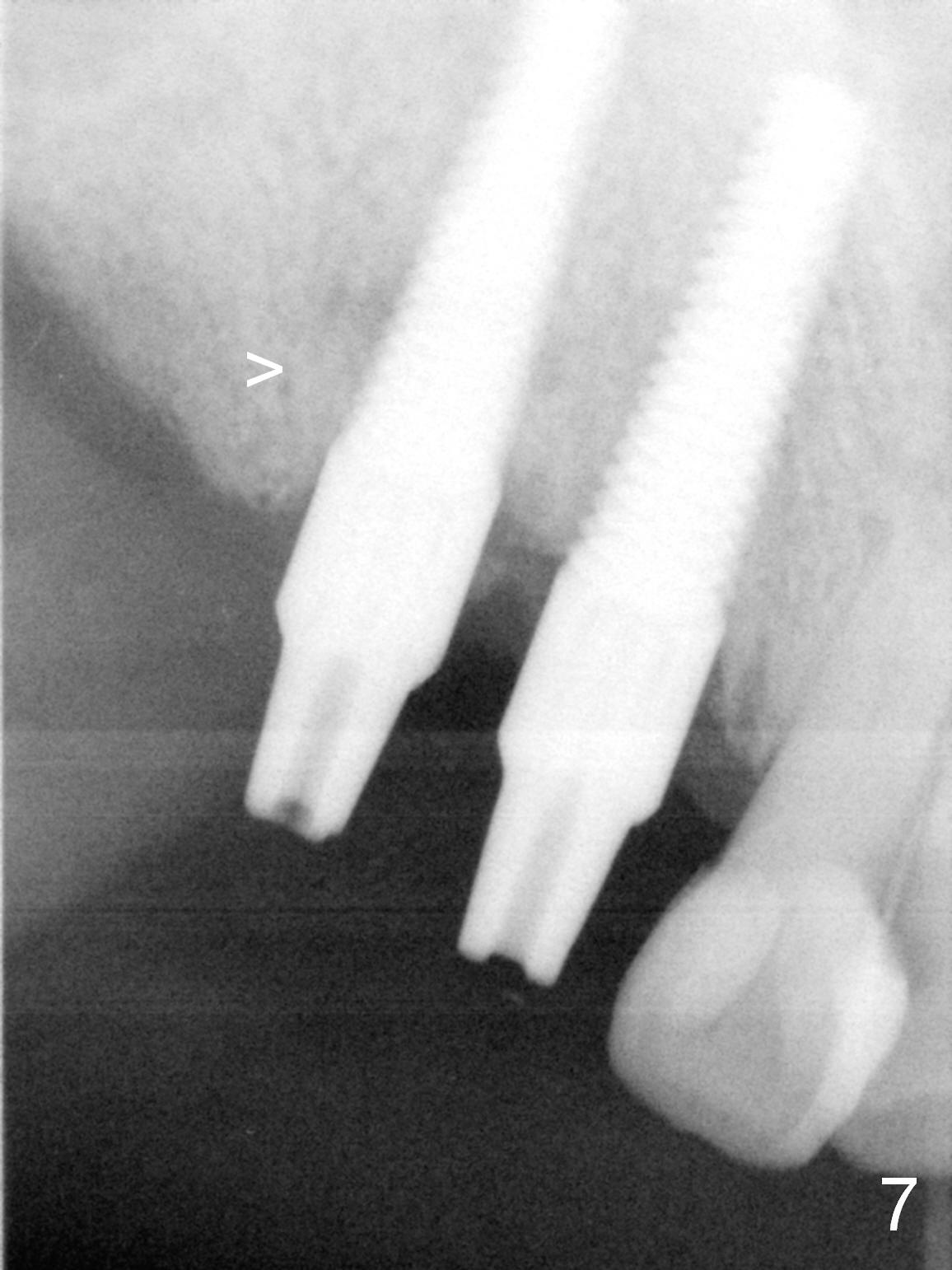
Bone density in the distal gap of #5 appears to have increased 3 months postop (Fig.7). Prior to definitive restoration cementation (3.5 months postop), the buccal plate does not collapse (Fig.8). There is no occlusal contact of the new restorations (Fig.9 *), probably due to bite discrepancy (Fig.10,11).
Return to Upper Arch Immediate Implant,
Technicians
Xin Wei, DDS, PhD, MS 1st edition 11/16/2015, last revision 03/01/2016