|
|
|
|
|
|
|
|
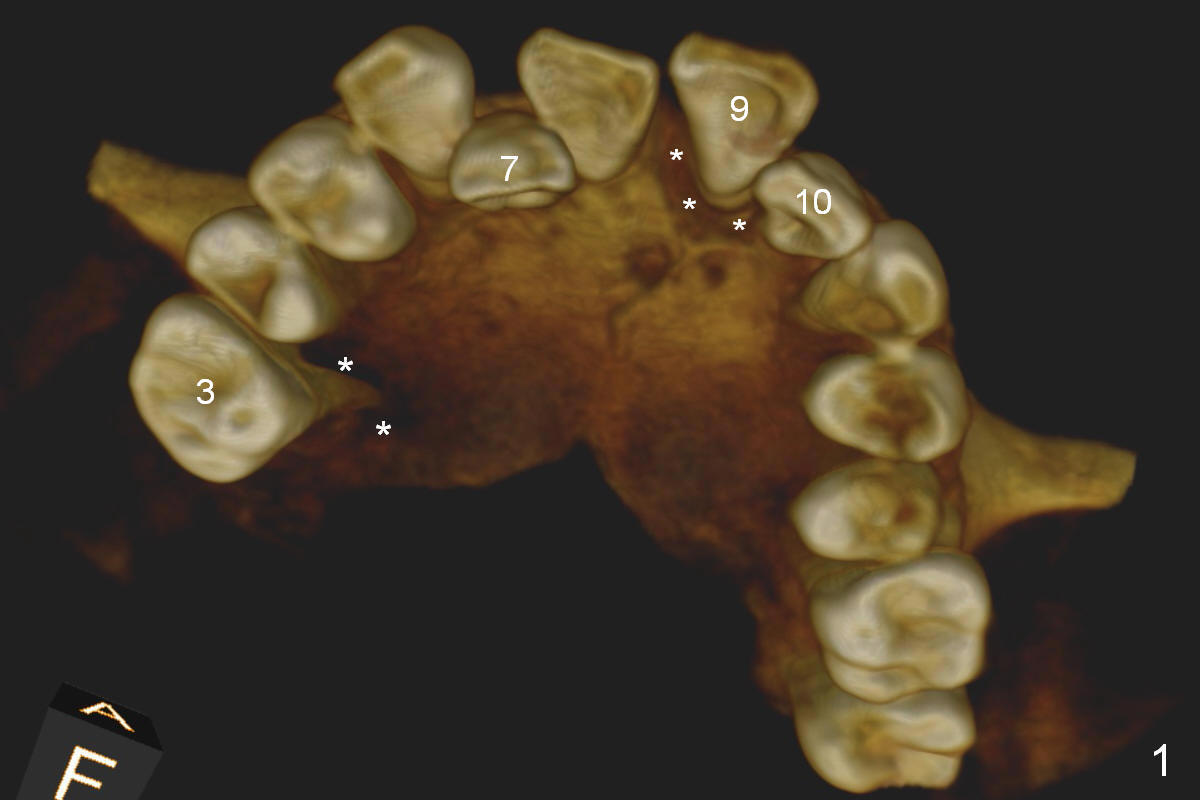
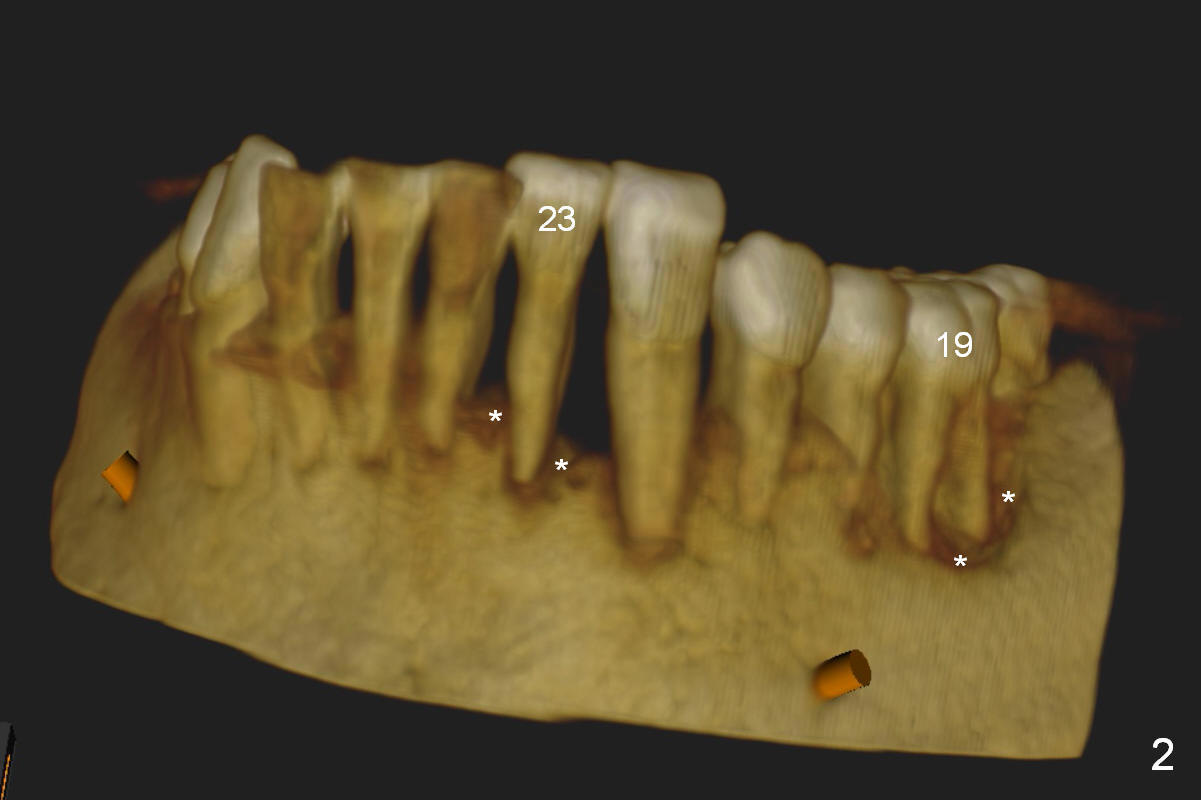
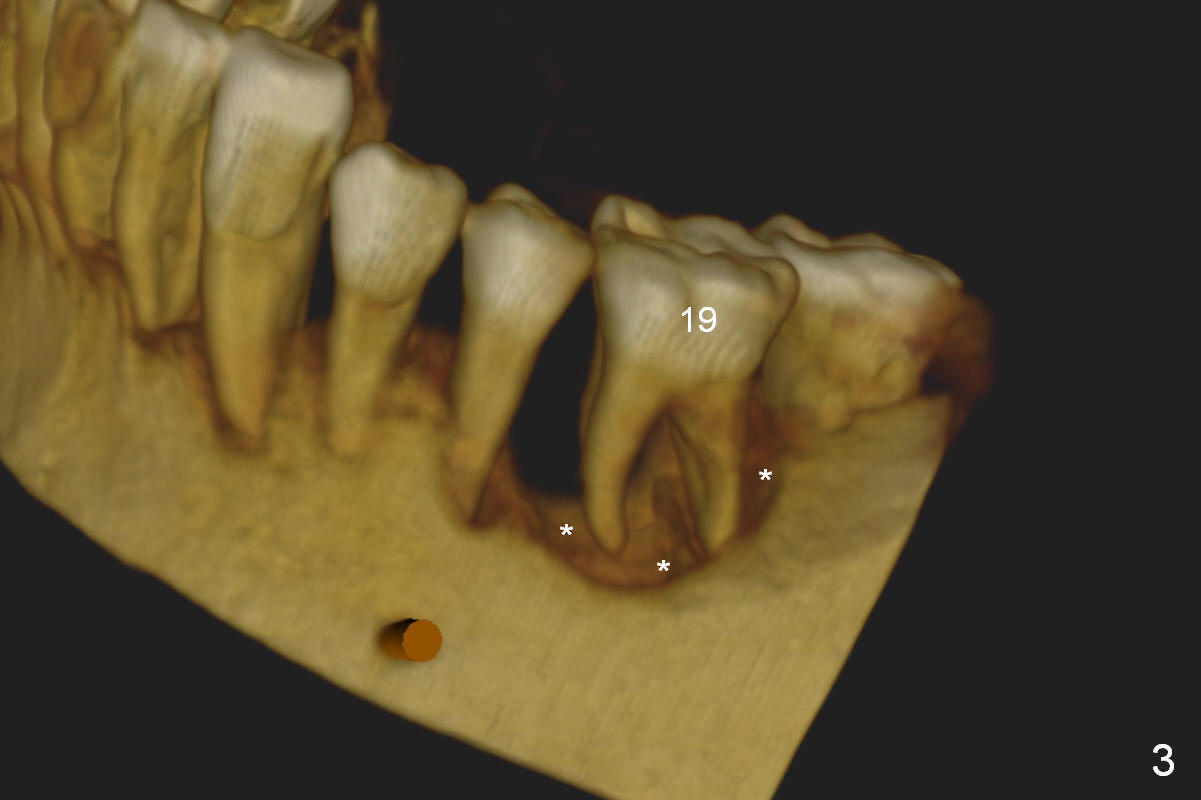
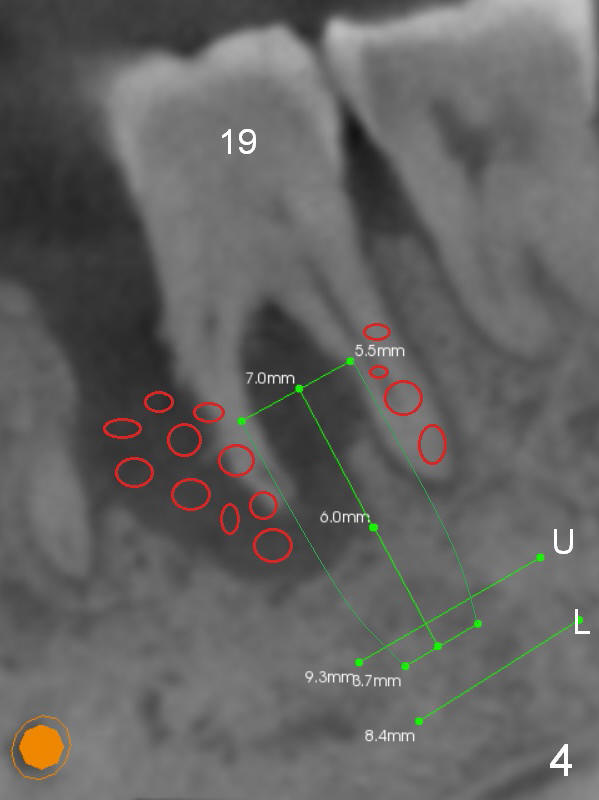
Periodontitis, Bruxism and Malocclusion
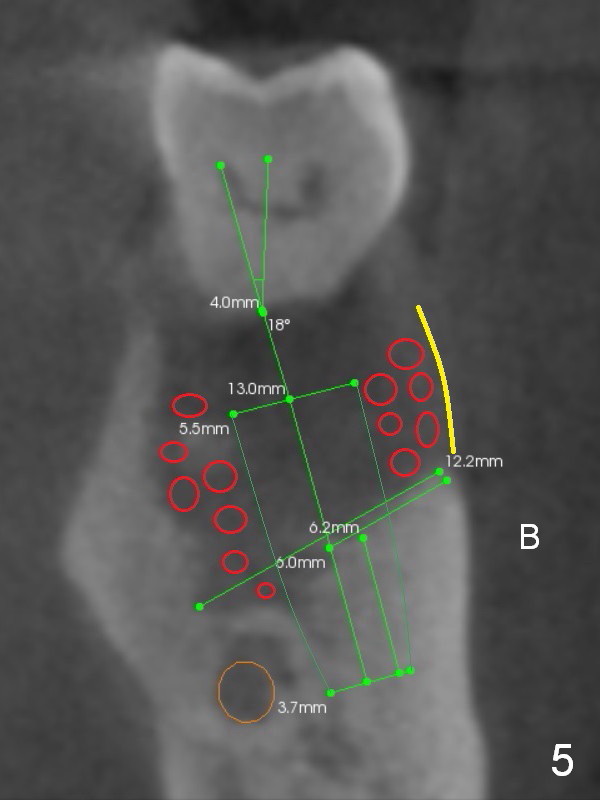
A 45-year-old man (SH) has periodontal (#3,9,19,23 (bone loss: Fig.1-3 *)) and orthodontic (#7,10 cross bite) problems, which he wants to solve at the same times. The tooth #19 is symptomatic (Fig.4,5). Infiltrate the buccal plate with 2% Xylocaine 1:50,000 Epinephrine and Septocaine (away from the Mental Foramen). After extraction and debridement, the socket is treated with Metronidazole. Osteotomy is initiated slightly buccal (B) to the middle of the socket bottom (Fig.5), using Sinus Master Kit drills (6 mm deep). After each drill, gently explore the lingual wall of the osteotomy with a fine curette or an explorer to determine whether the wall is perforated or not. Place a 5.5x13 mm implant (or short) between the buccal plate and the Inferior Alveolar Nerve (brown circle). If the torque is high, use the corresponding drill and tap. A 5.5 mm angled abutment will be used (15 or 25°, will arrive Monday morning). When X-ray is taken, the apex of the osteotomy should be superior to the upper border of the Inferior Alveolar Canal (Fig.4 U) and inferior to the Lower one (L). Bone graft is placed (Fig.4,5 red circles) after placement of PRF buccally (Fig.5 yellow curved line). If visibility is poor, make an incision and insert Epinephrine gauze under periosteum for hemostasis. Take photos when a 2 mm pilot drill in place to show the coronal end of the drill at the lingual cusp instead of the central fossa.
Return to Multiple Tooth Immediate Implant,
3,
9,
19,
23
Xin Wei, DDS, PhD, MS 1st edition 04/16/2016, last revision 04/22/2018