

,%203x16(4)%20mm.jpg)
,%204x7.5(3),%204x5.7(2).jpg)






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1- vs. 2-Piece Implants for Lower Incisors
As mentioned previously, the teeth #24-26 have exfoliated (Fig.1). After extraction of #23, osteotomies are initiated at #23 and 26 with 1.5 and 1.2 mm drills (12 mm deep, Fig.2). It appears that the osteotomy at #23 is close to the neighboring tooth (*). Lindermann bur is used to mesialize the osteotomy before placing 3x16(4) and 2.5x14(4) mm 1-piece implants with bone graft (Fig.3 >).
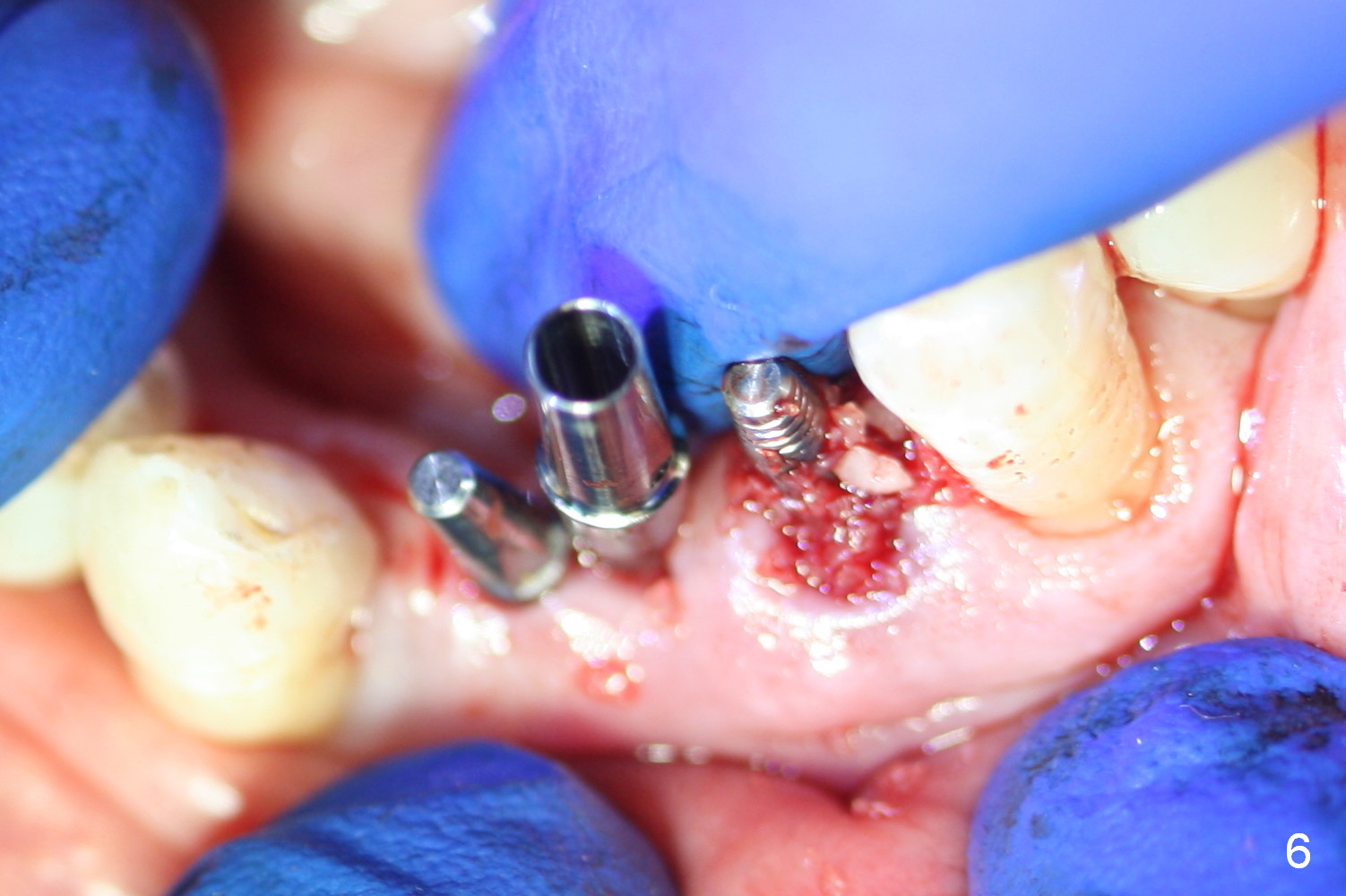
Fig.4 compare the diameter of the abutment of a 3x14(2) mm 1-piece implant with two of pair abutments for 2-piece IBS implants (the smallest ones: 4x7.5(3) and 4x5.7(2) mm). It appears that the 4 mm pair abutment is too large for the lower incisor restoration (Fig.5,6).
In contrast, an immediate provisional is fabricated without preparation of the abutments of the 1-piece implants (Fig.7). After application of periodontal dressing (Fig.8,9), the patient is discharged with satisfaction. In all, 1-piece implant is the most stable without complications of loosening abutment or implant or abutment screw fracture. The provisional needs modification once the wound heals initially.
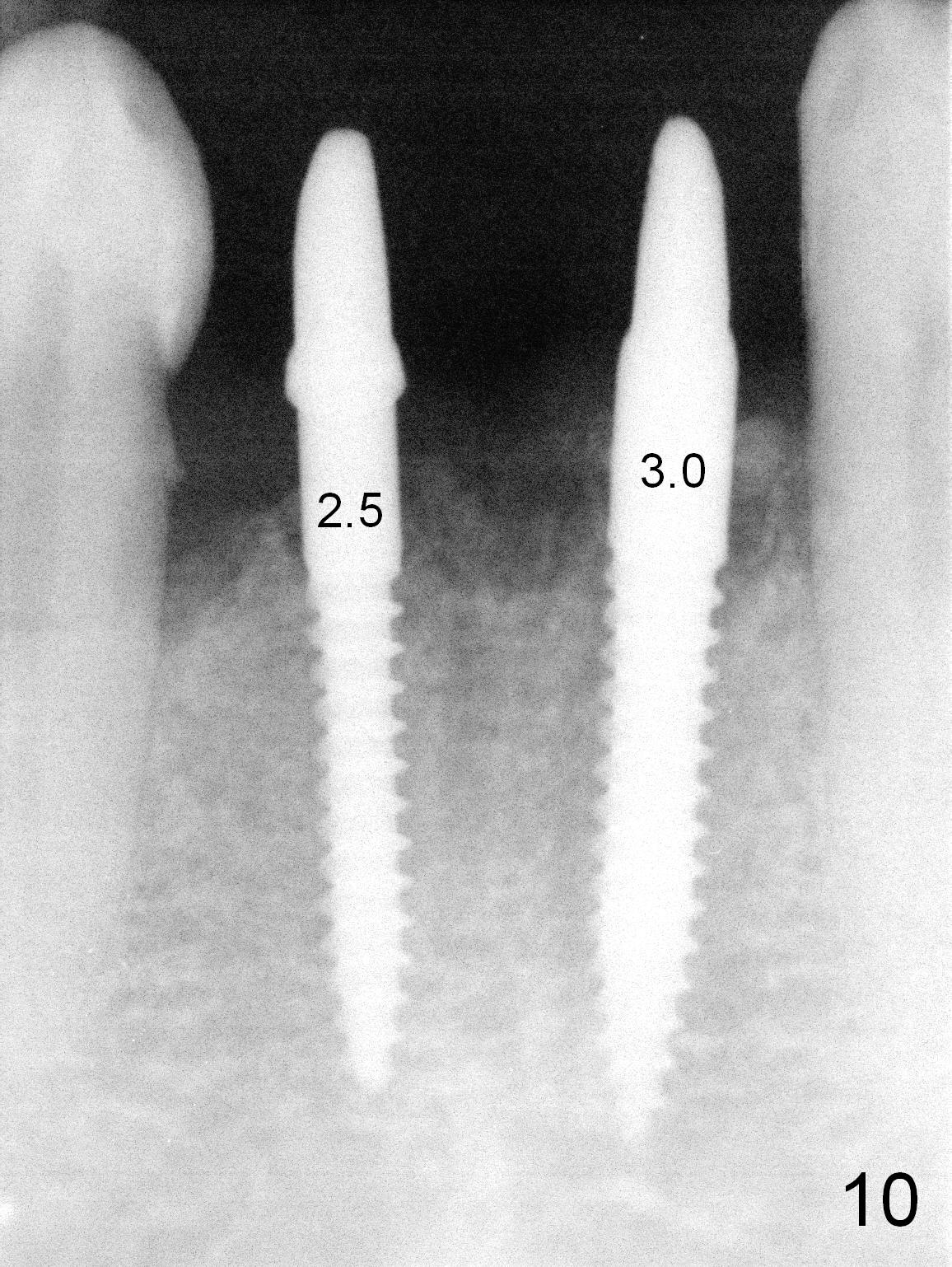
The provisional is partially fractured 2.5 months postop. There is mild bone resorption around the 2.5 mm delayed implant, whereas apparent bone growth around the 3.0 mm immediate implant (Fig.10). The ridge is narrower at the former site than at the latter (Fig.11). The gingiva is healthy around the implants (Fig.11,12).
Remove calculus from the mesial surface of the tooth #27 before bridge bonding. Take PA after cement removal. Check other teeth for mobility.
Return to
Lower Incisor Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 09/01/2016, last revision 12/31/2016