|
|
|
|
Reconstruct Lower Anterior Bridge
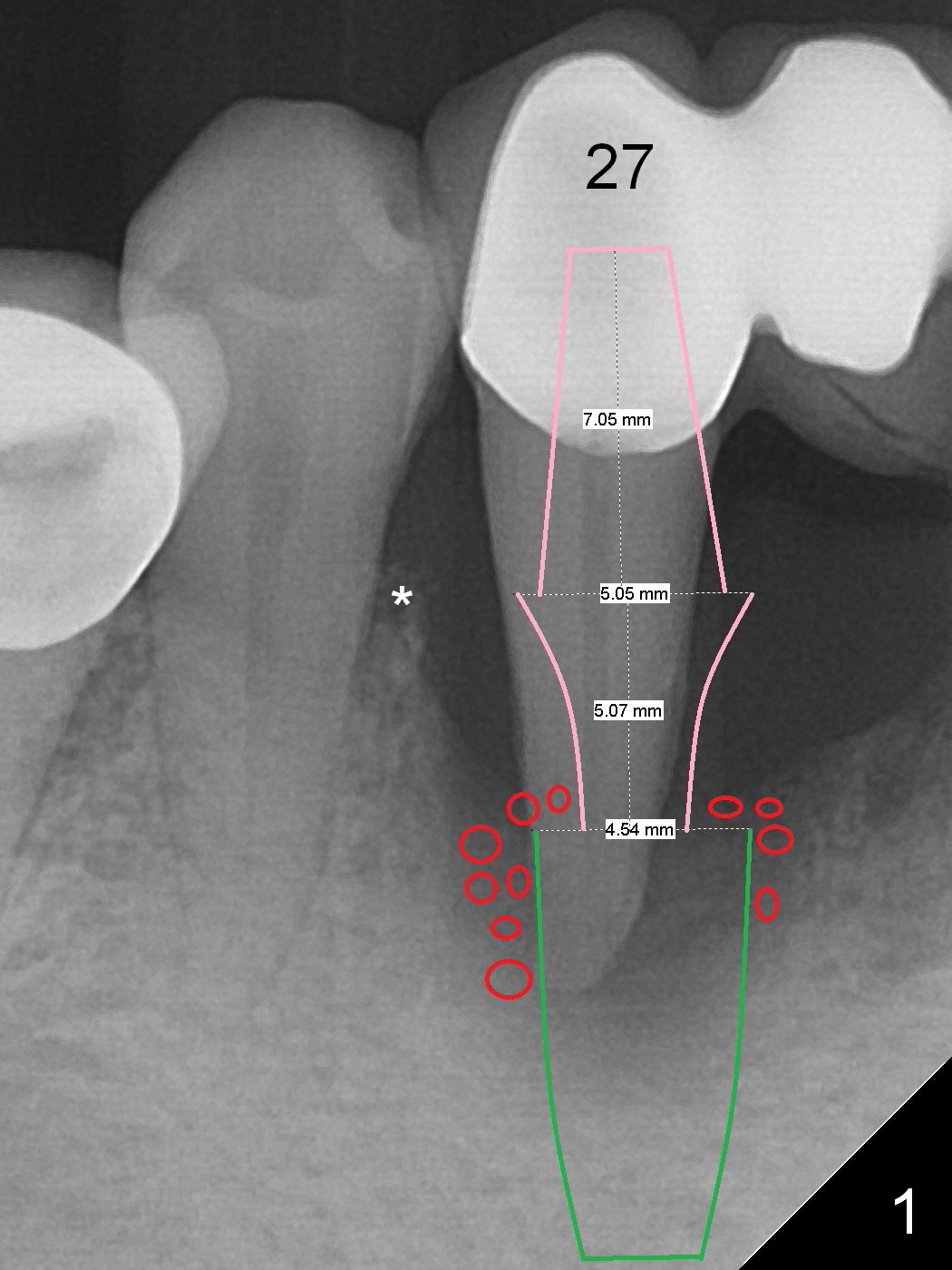
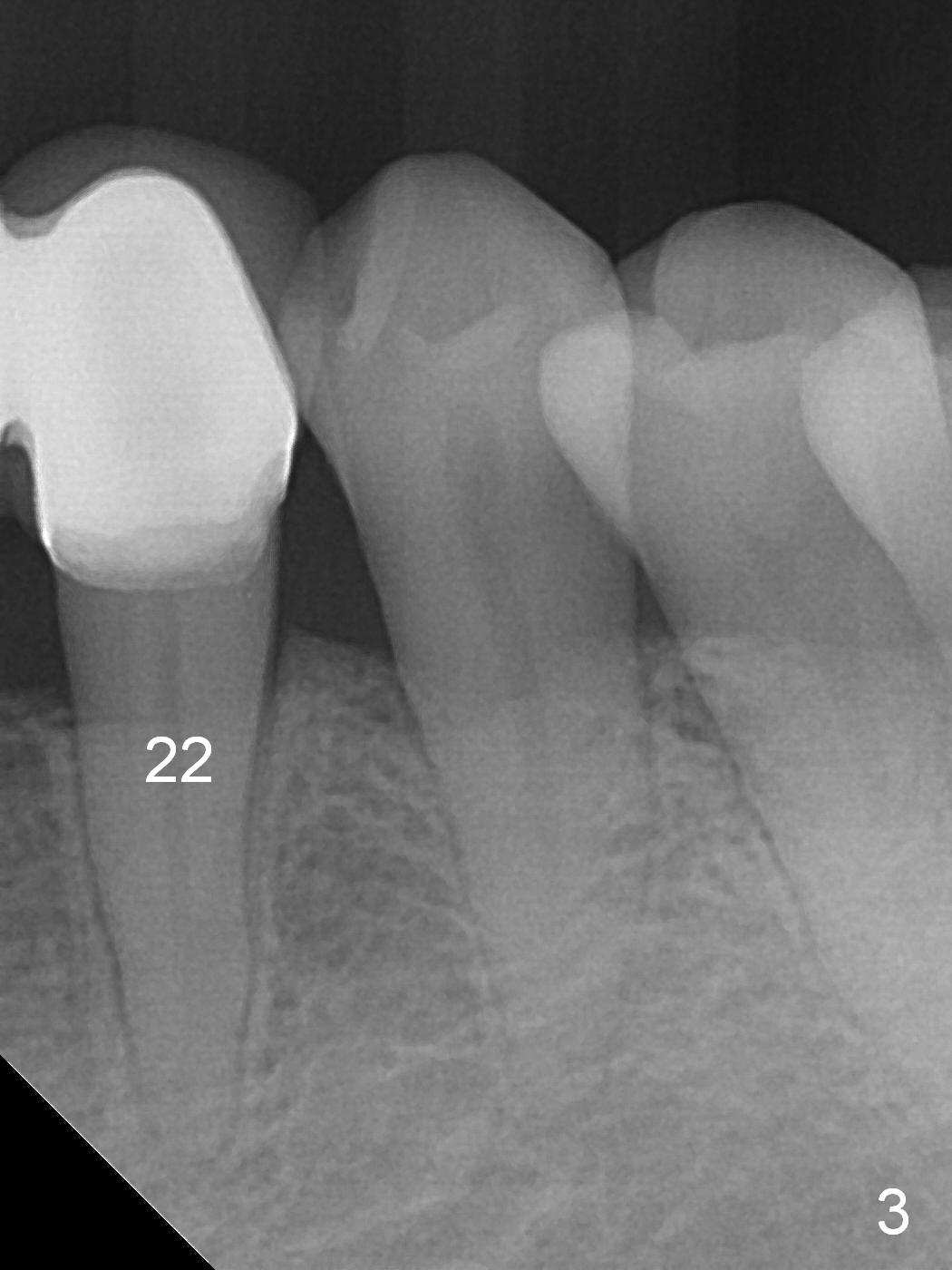
A 57-year-old woman has a 20-year-old loose FPD (fixed partial denture, Fig.1-3). Upon Alginate impression for stent, the 6-unit FPD was dislodged with the exfoliated abutment at #27. After removal of calculus from the root of #27, the FPD was placed in situ and temporarily cemented to #22 abutment. When the patient returns, remove the FPD, treat the socket of #27 with Clindamycin, place implants at #23, 25 and 27 and fabricate a 6-unit provisional FPD. At definitive stage of restoration, fabricate a 4-unit FPD at #24-26 and a single unit at #27. Since bone loss is more severe mesiobuccally at #27 (Fig.1), place an implant as lingual as possible, but slightly more mesially. If the defect is so severe that the implant (green) has to be placed deep, the abutment margin with the longest cuff (5 mm, pink) is less likely to contact the distal crest (*). Crown margin (i.e., abutment margin of an implant) should be 2 mm more coronal to the crest normally. The condition that does not meet the requirement is called violation of biologic width, associated with periodontitis or periimplantitis.
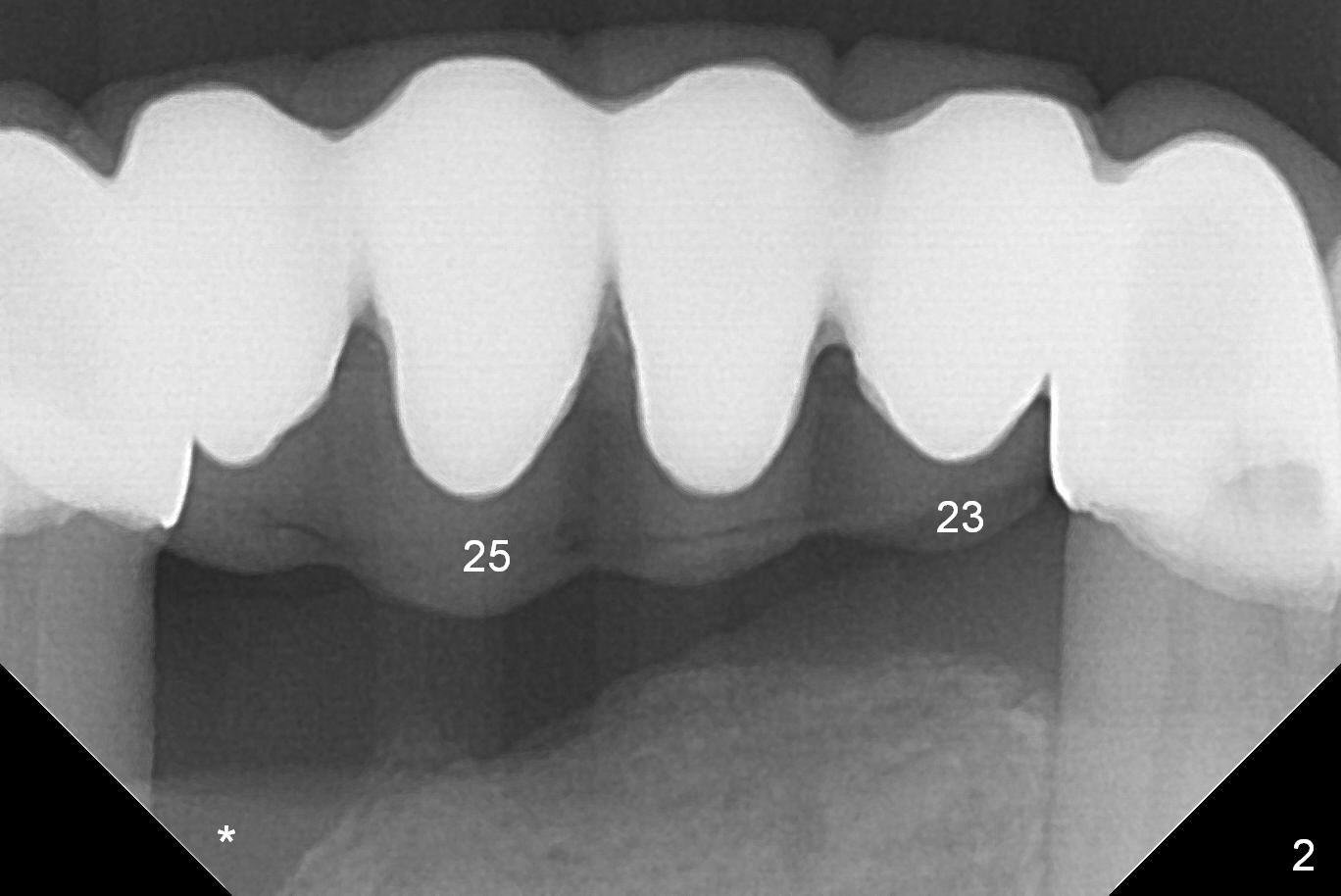
For the same token (severe bone loss at the mesial aspect of the site of #27), the site of #26 is not a good candidate one for implantation (Fig.2 *). The site of #25 is most likely a better one. The site of #23 should be the most favorite one among #23-26, since the edentulous site next to the dentate one is less likely resorbed after extracted. For a FPD, abutments should be far away from each other. No matter what, prepare 1-piece implants (as small as 2.5 and 2.0 mm ones) and surgical handpiece (why?). Take preop photos to show recessive gingiva at #27.
Return to
Lower
Incisor,
Canine Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 01/29/2017, last revision 05/12/2020