

.jpg)



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Small and Short Implant
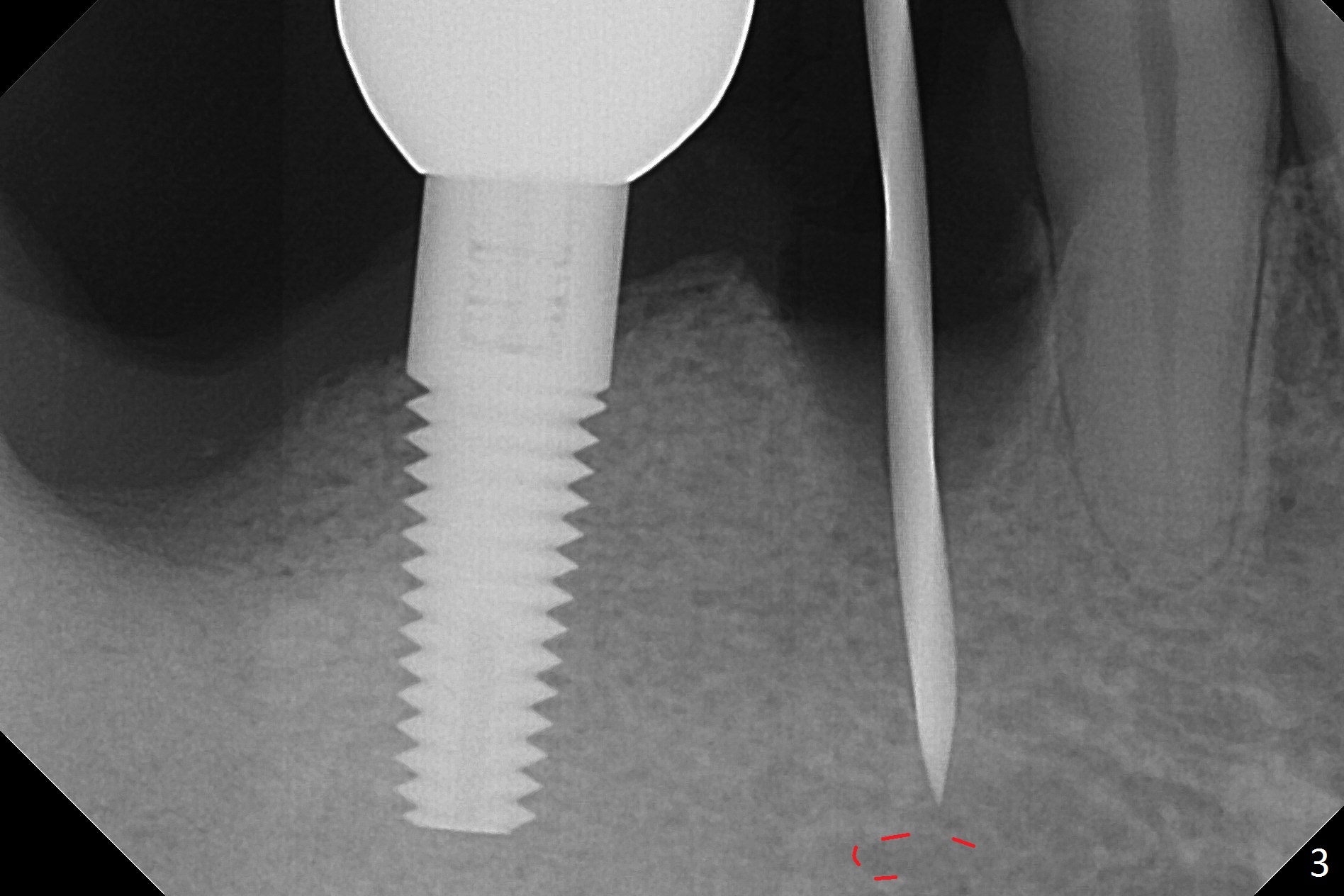
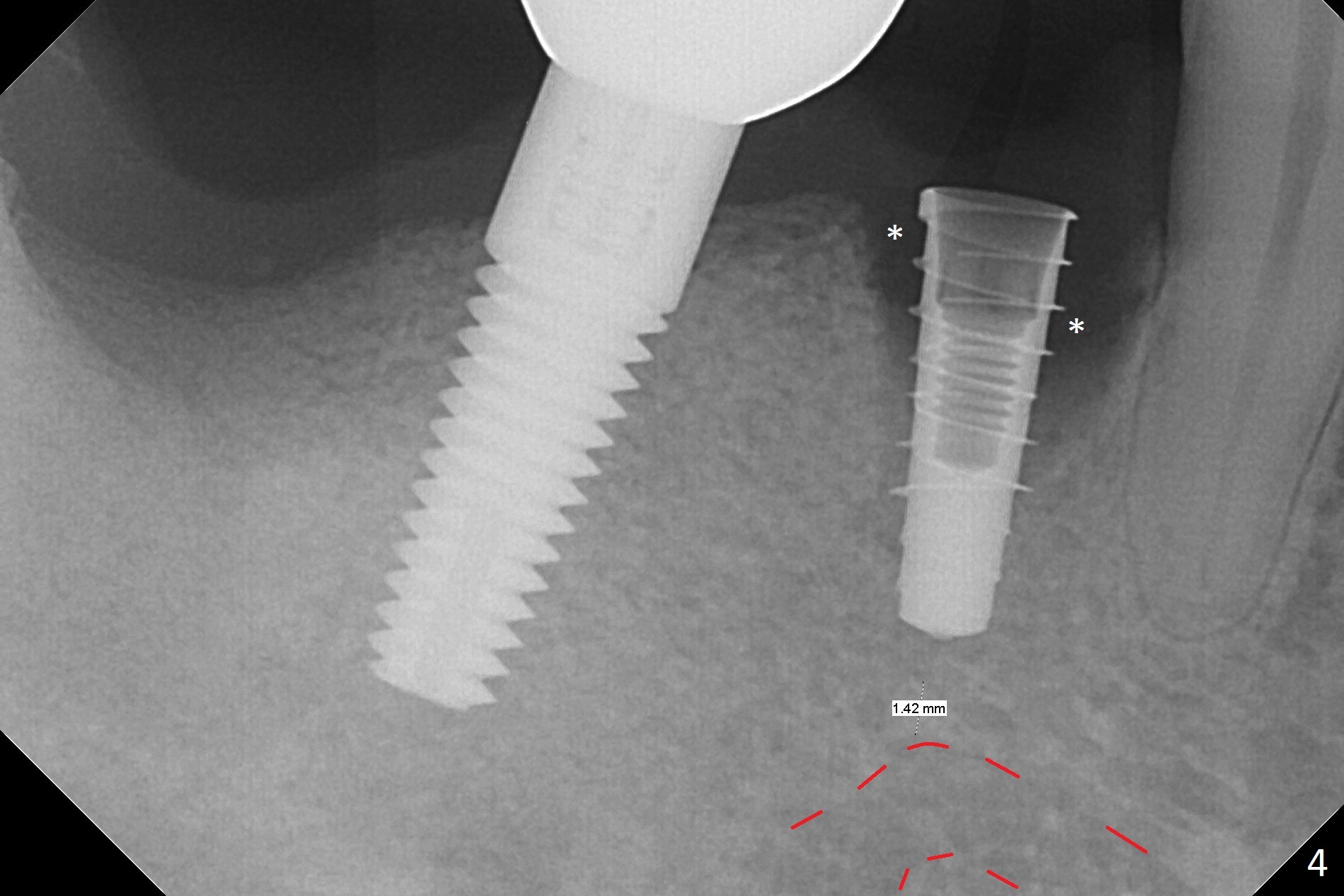
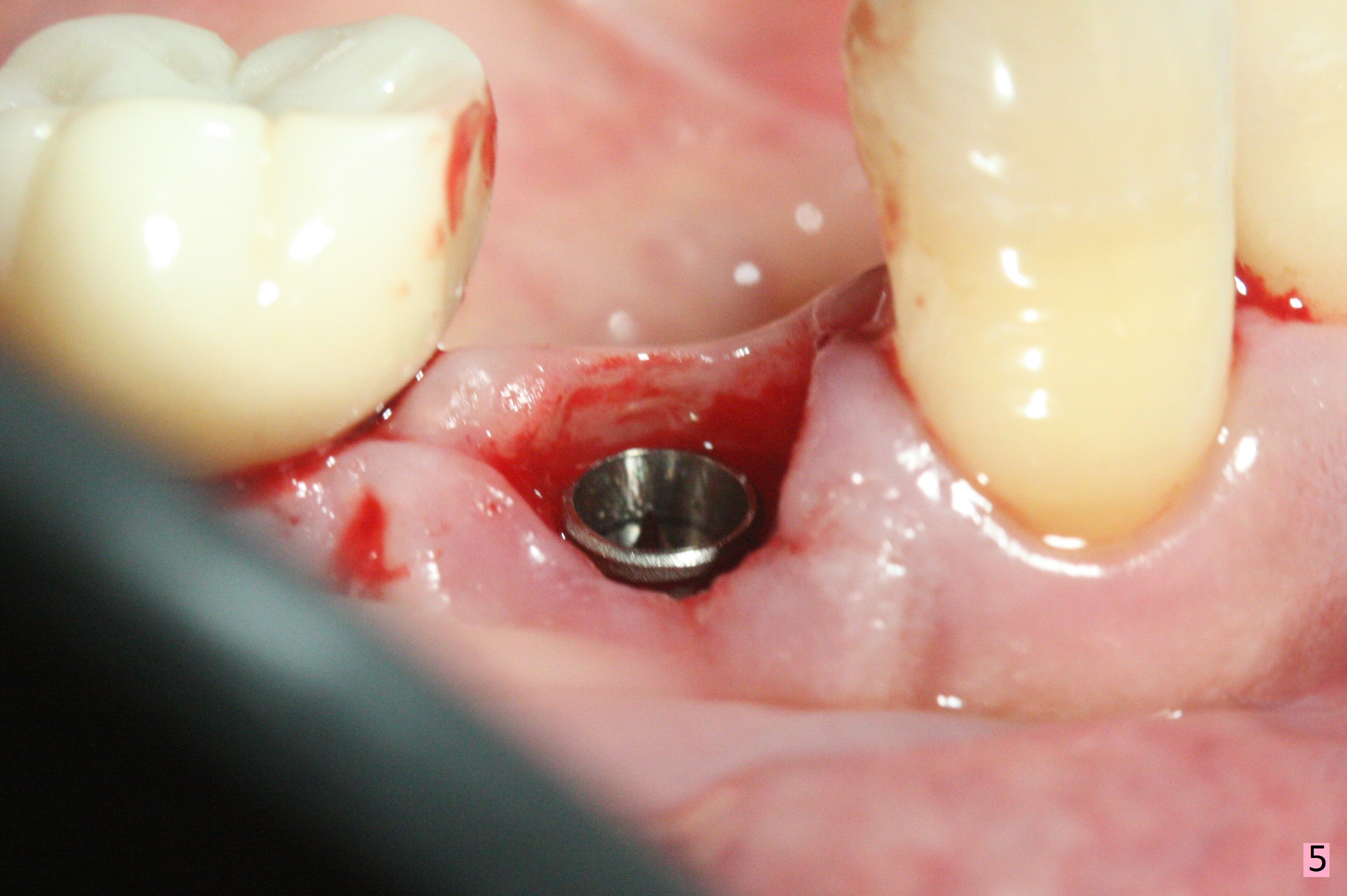
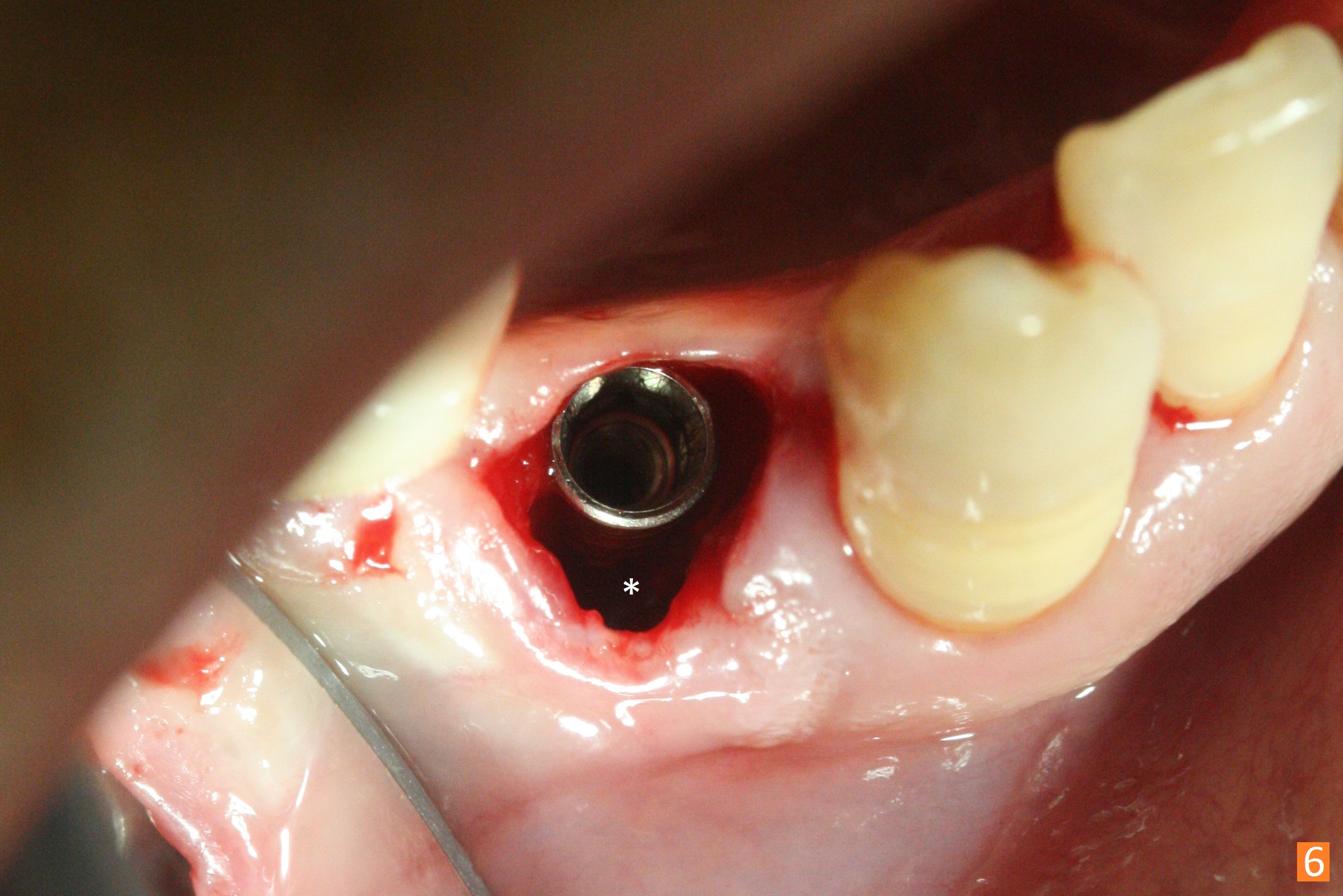
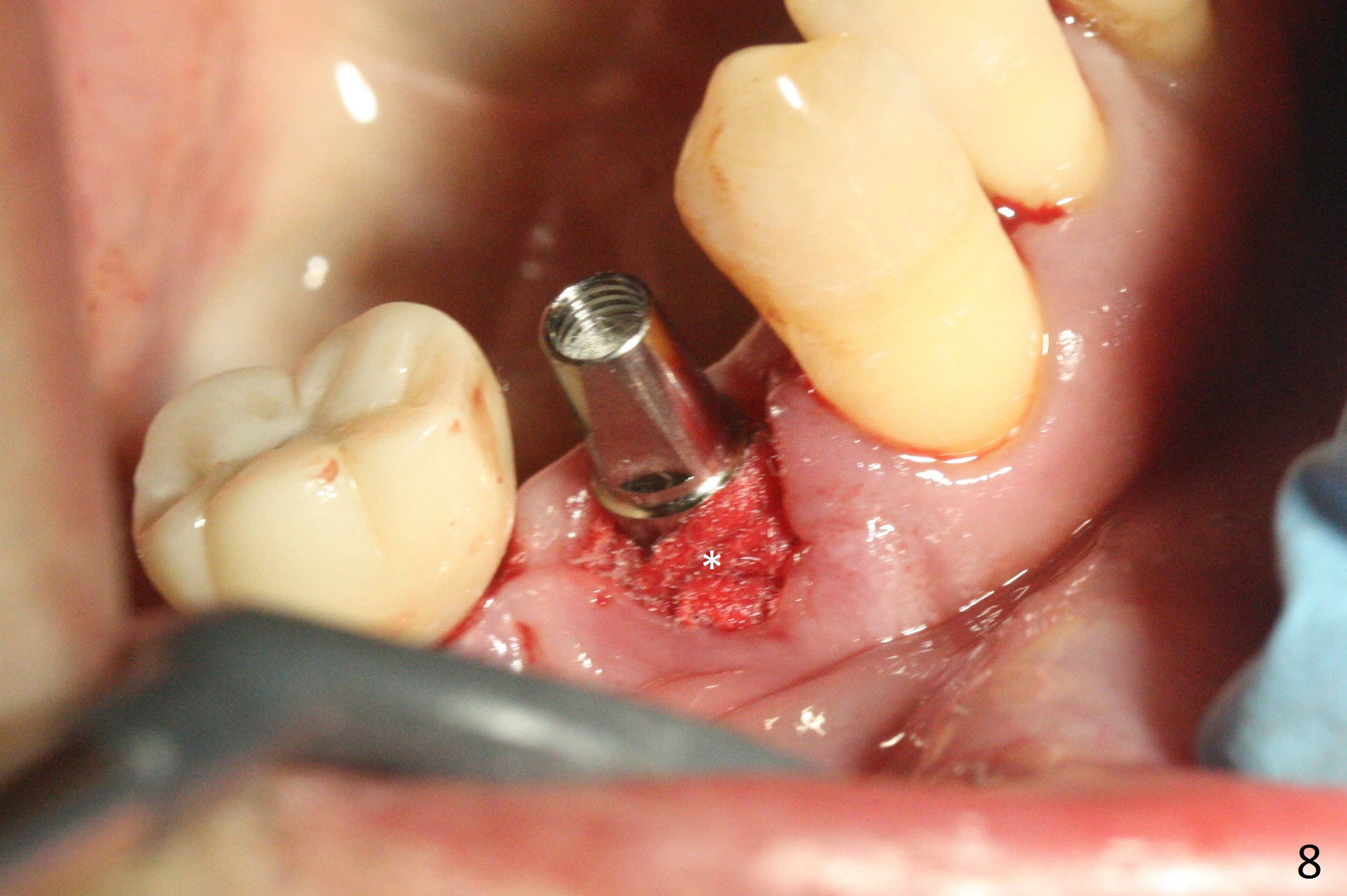
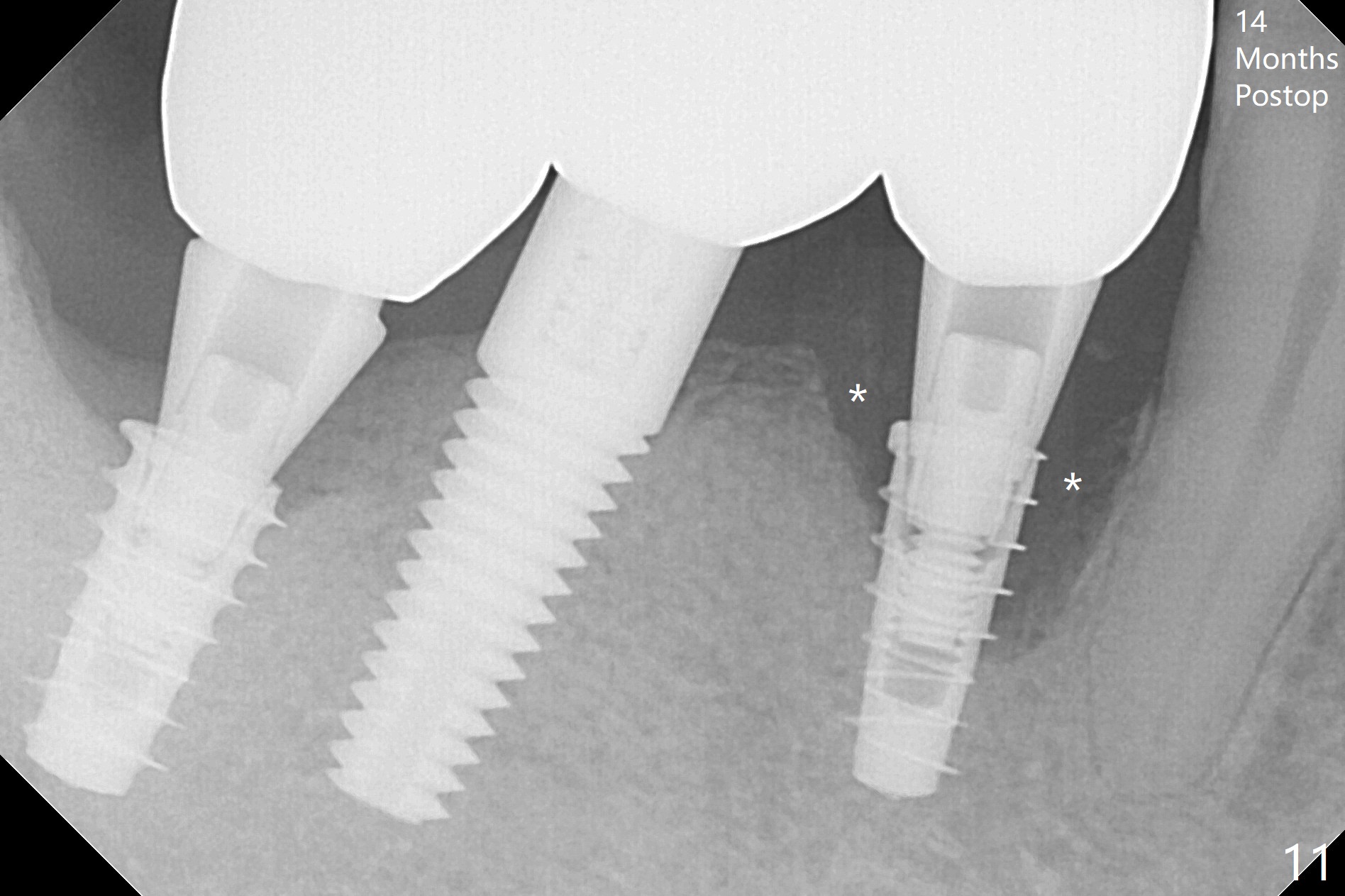
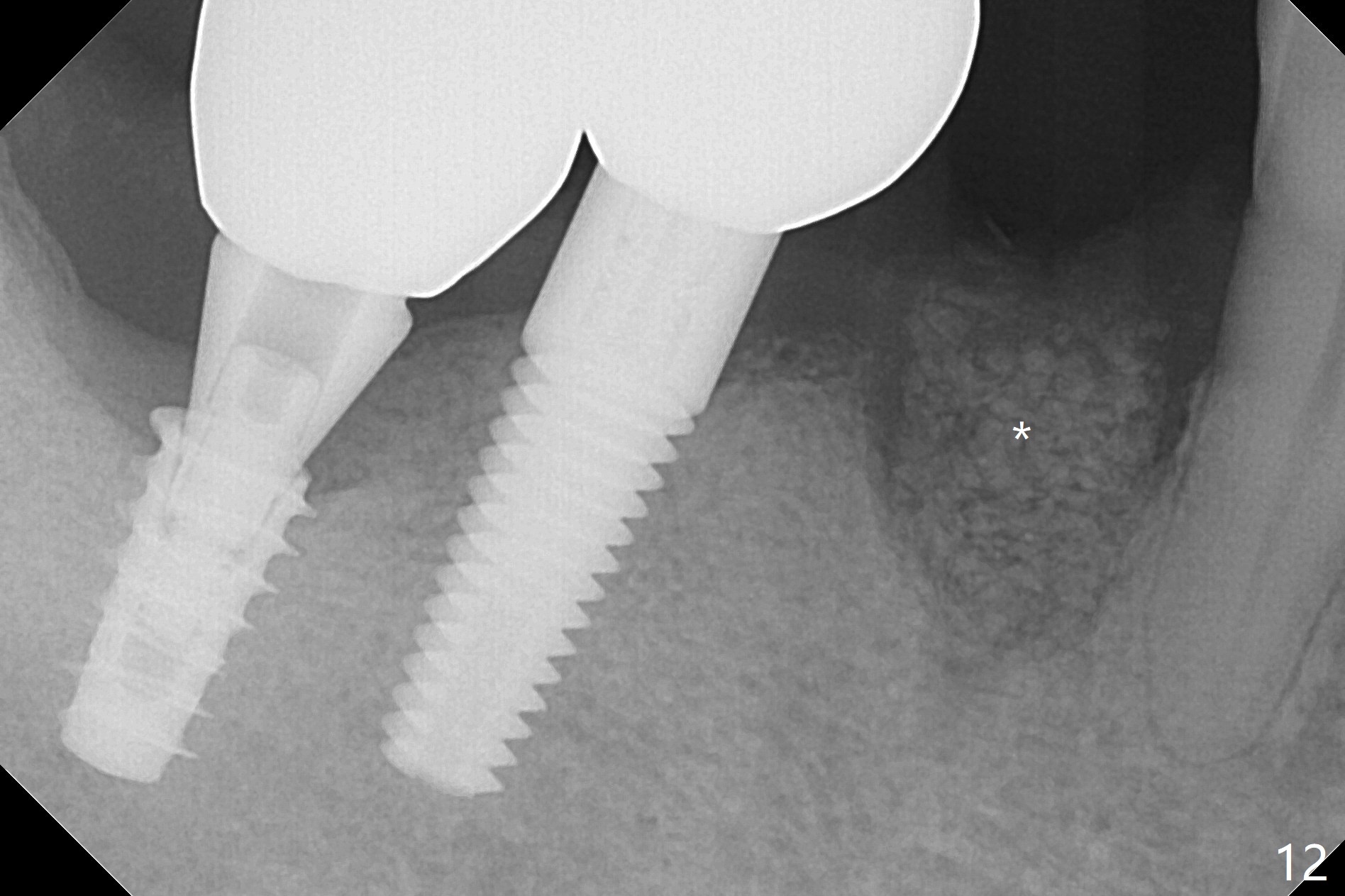
The affected tooth (#28) has buccal gingival recession (Fig.1). As expected, the buccal plate is found low after extraction. Osteotomy is established in the lingual slope of the socket with 1.5 mm drill for 13 mm (Fig.2,3). Following use of Magic Drill 3.3 mm for 13 mm, a 4x11 mm dummy implant is incompletely seated (Fig.4); it is also close to the Mental Loop (Fig.4 red line). After use of Final Drill, a 4x9 mm IBS implant is placed 4 mm and 2 mm subgingival buccal and lingual, respectively (Fig.5) with a large buccal gap (Fig.6 (40 Ncm)). After placement of allograft in the peri-implant space (Fig.7 *), a 4.5x5.7(4) mm abutment is placed (A). A piece of gauze is placed in the remaining buccal space prior to provisional fabrication (Fig.8 *). The space occupied by the gauze is later filled with collagen plug before provisional seating. The gingiva is healthy around the provisional 12 days postop (Fig.9). To reduce buccal gingival recession, the buccal margin of the provisional is shortened 4.5 months postop (Fig.10 arrow). PA taken 5.5 months postop is shown with the implant at 31. The lingual gingiva is erythematous, edematous, and recessive with +BOP and deep pockets 14 months postop (Fig.11). It appears that the small and short implant is not favorable for healing. The infected implant is removed with the missing buccal plate; bone graft is placed 15 months postop (7 months post cementation, Fig.12,13).
Return to
Lower Premolar Immediate
Implant
, #3,14,15,
31, Course 1,2
Xin Wei, DDS, PhD, MS 1st edition 06/12/2017, last revision 08/20/2018