|
|
|
|
|
|
|
|
|
|
|
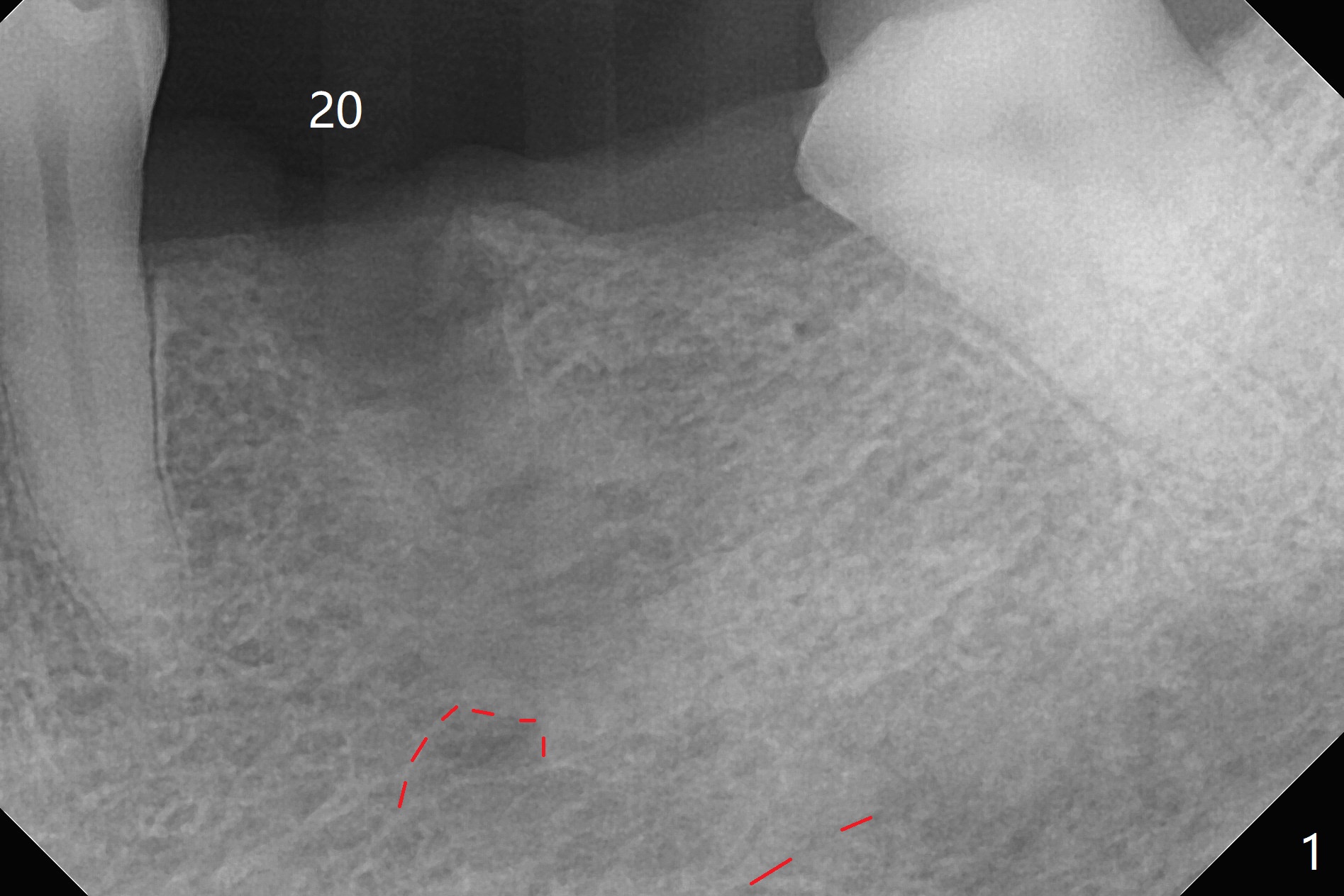
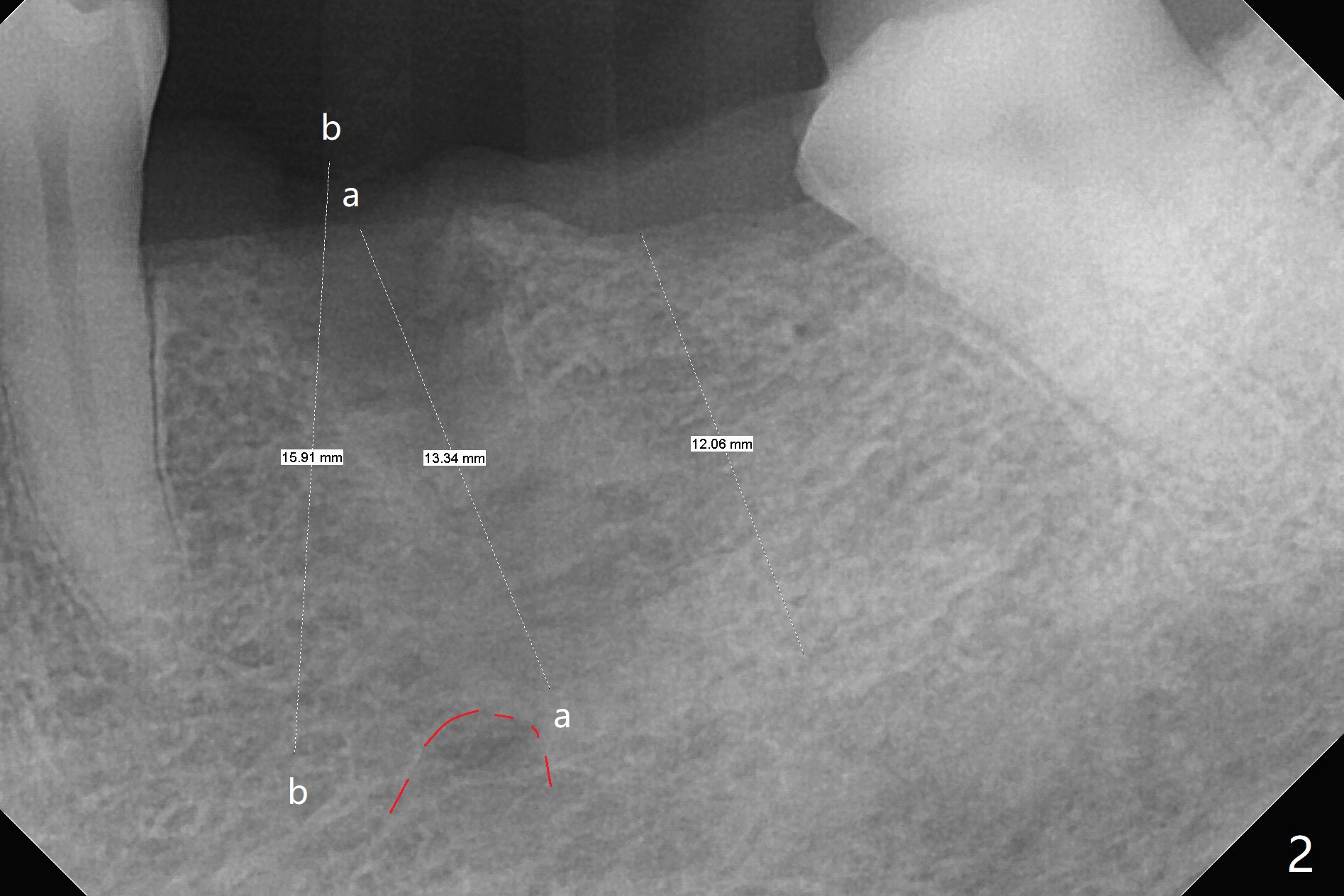
No Drill Osteotomy for Immediate Implant
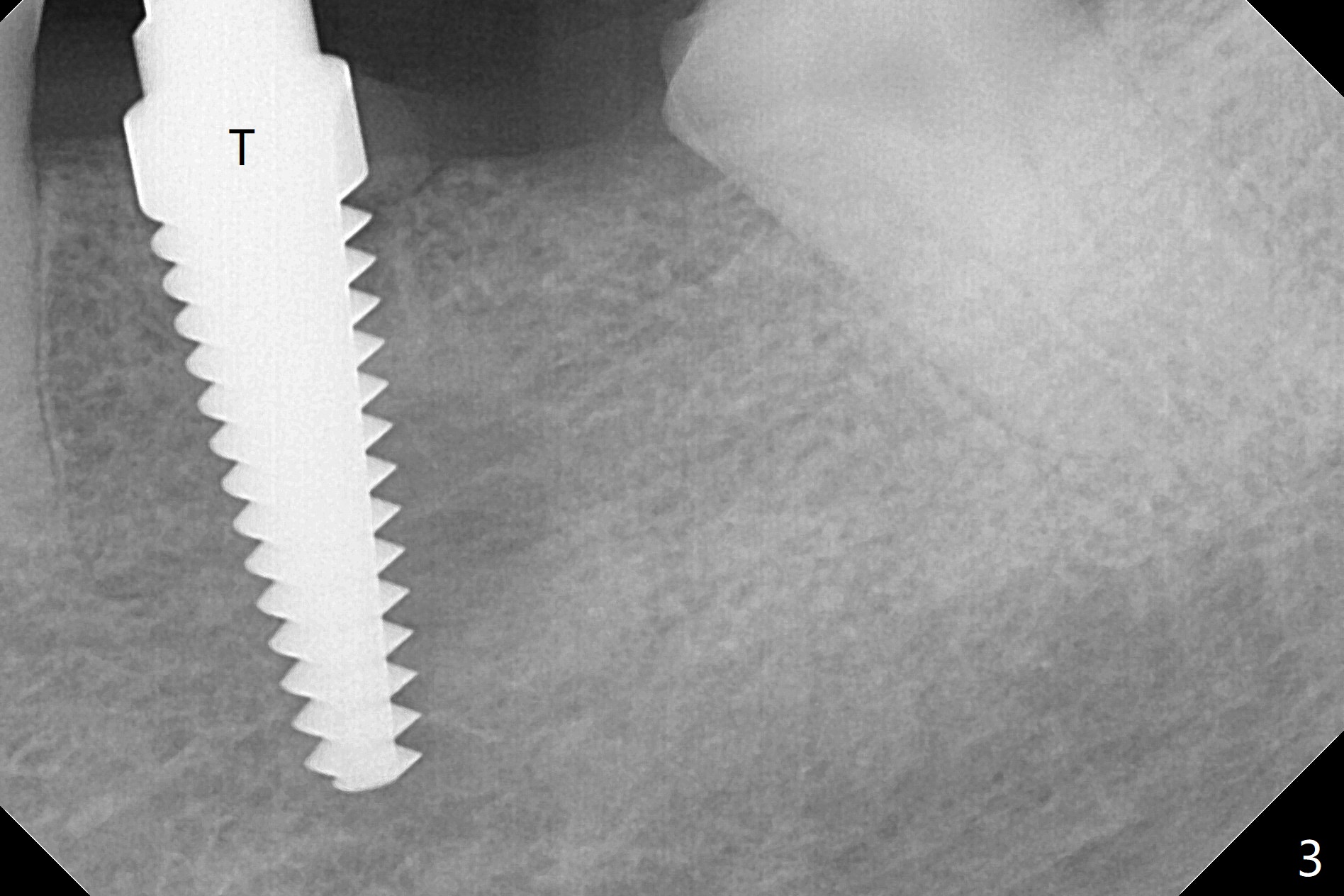
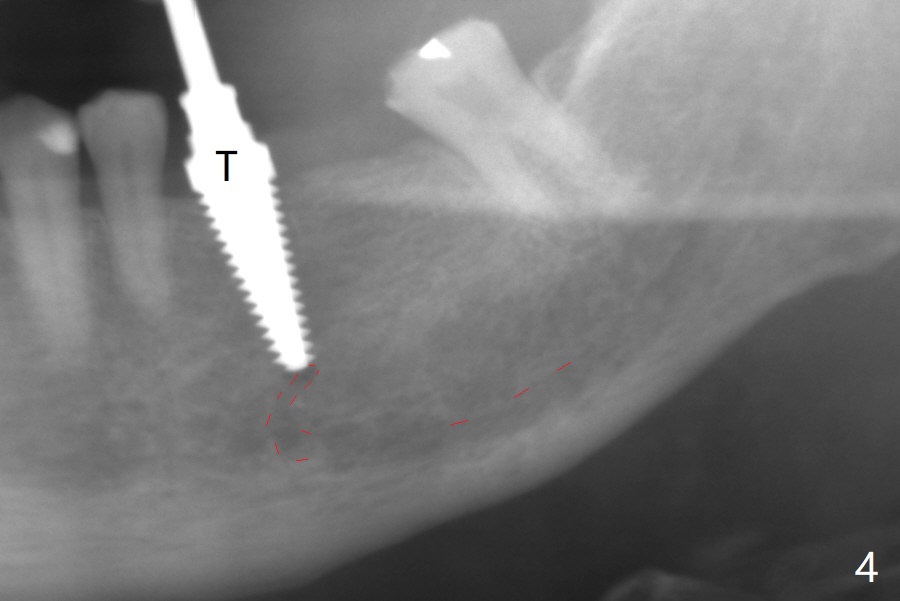
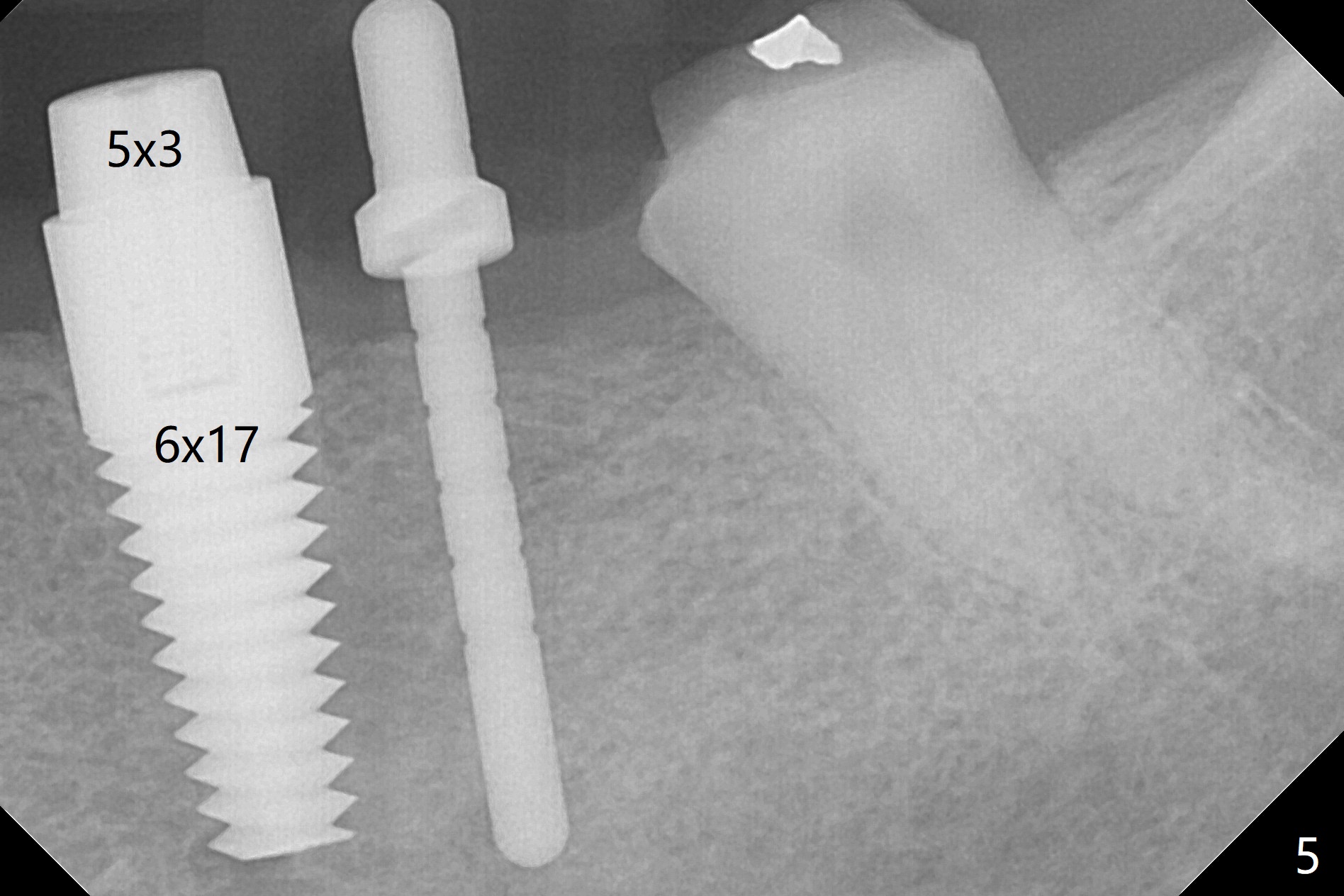
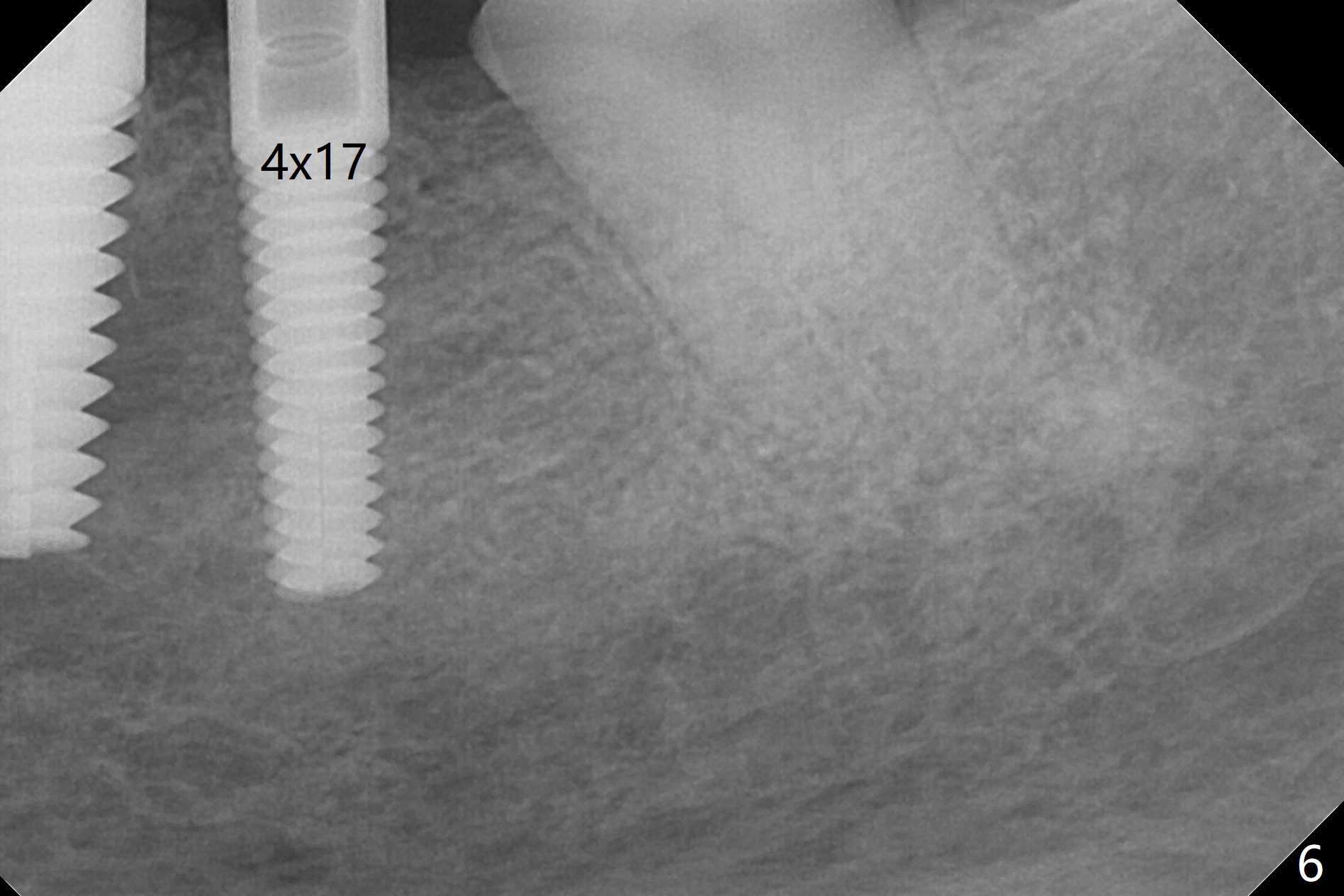
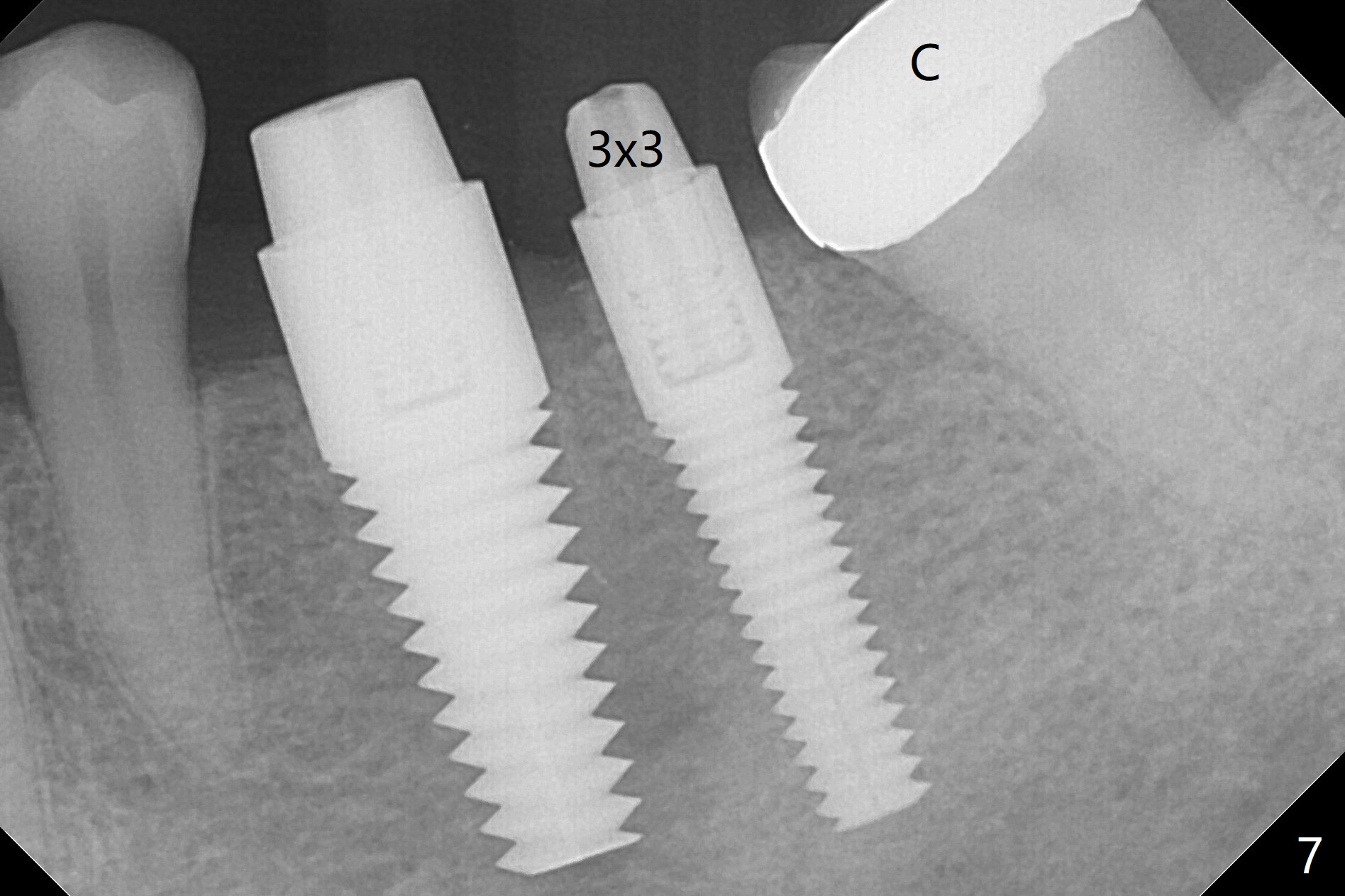
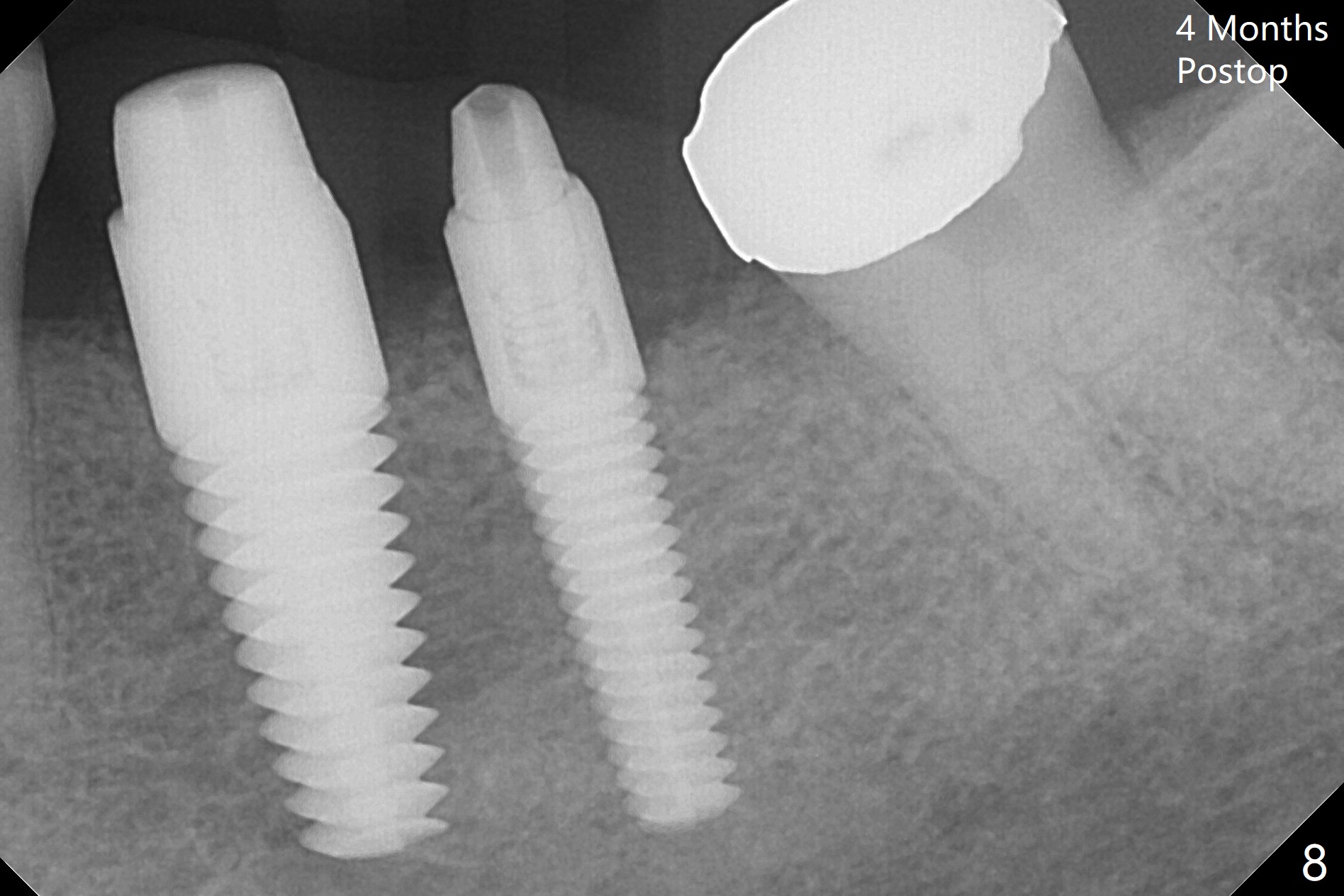
When the tooth #20 is extracted, the buccal and lingual plates are intact, but the apical lesion is deep. A PA is taken (Fig.1). Osteotomy will be established either along the long axis of the original socket (Fig.2 a line) or in the mesial slope (b line). Either osteotomy may damage the Mental Loop (red dashed line). To reduce the complication, osteotomy is being made by inserting 3.8 to 6 mm taps. In fact the 6 mm tap achieves stability (Fig.3,4), but it invades the buccal gap. When the tap is removed, the bottom of the socket is sensitive to probing with oozing from the socket. To reduce further compromise of the buccal space, Lindamann bur is used to remove the bone from the lingual and mesial plate, followed by placing a 6x17 mm implant with >50 Ncm (Fig.5). In fact the implant is placed shallower than the tap. When a 4x17 mm implant is placed at #19, there seems to be clearance from the Inferior Alveolar Canal (Fig.6). Postop there is no paresthesia. The buccal gap is <1 mm, which is filled with Vanilla Graft. After recementing the retainer (crown, C in Fig.7) at #18, periodontal dressing is applied to the sites of #19 and 20. Impression is taken 4 months postop with that of #15.
Return to
Lower Bicuspid
Molar Immediate Implant,
IBS
Xin Wei, DDS, PhD, MS 1st edition 10/24/2017, last revision 02/23/2018