
|
|
|
|
|
|
|
|
|
|
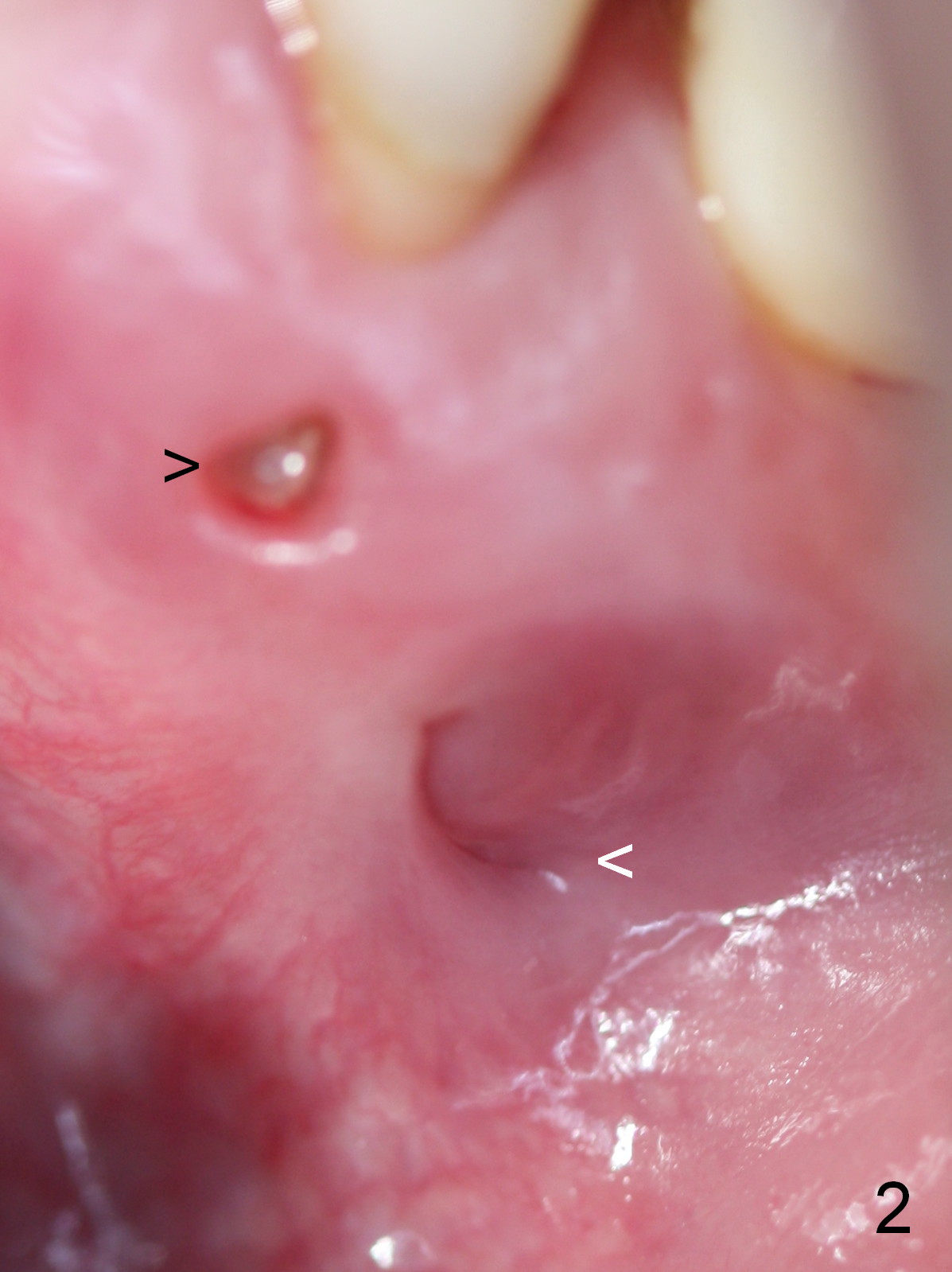
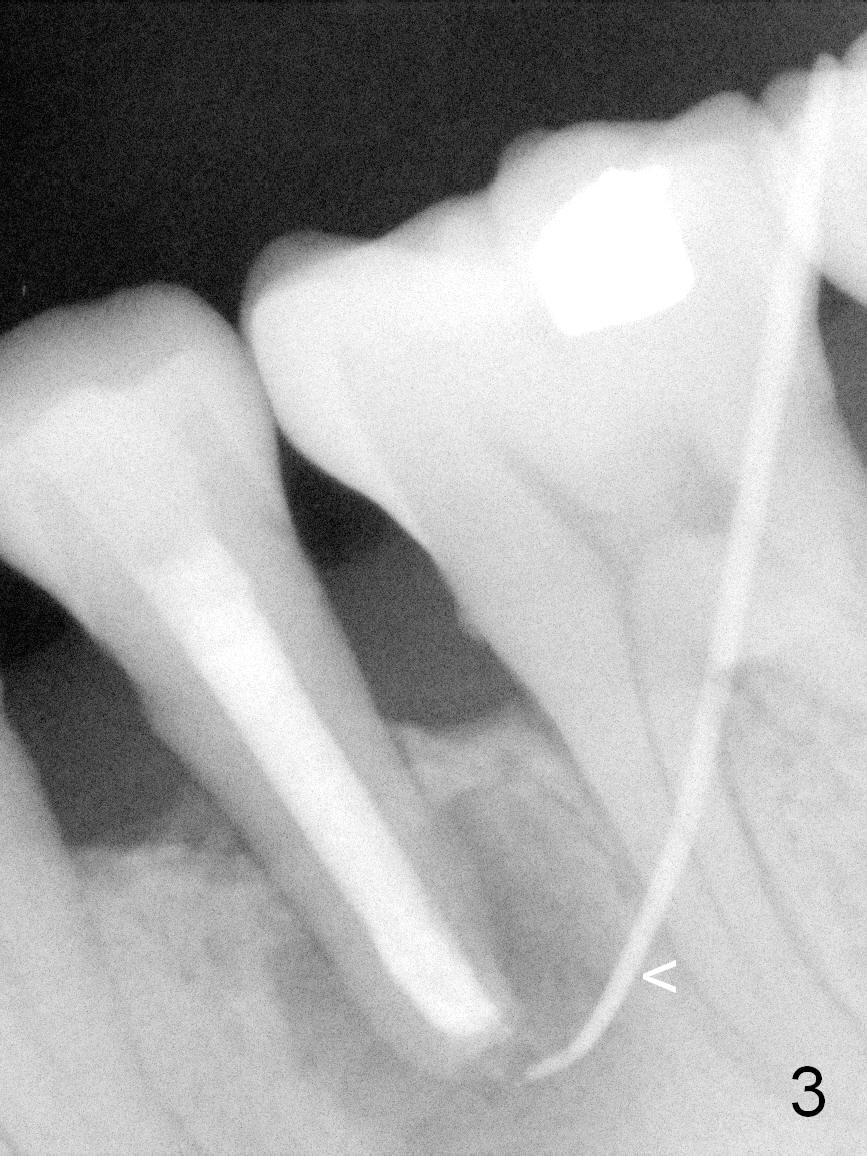
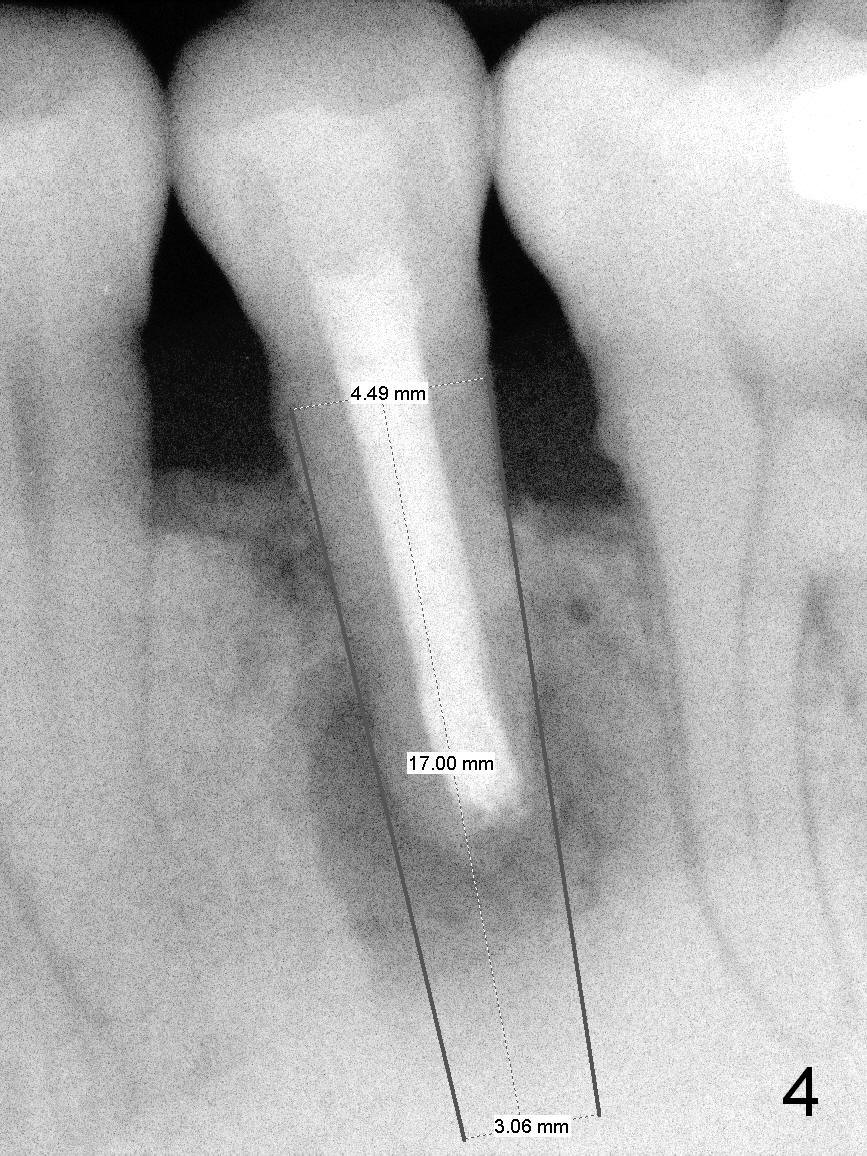
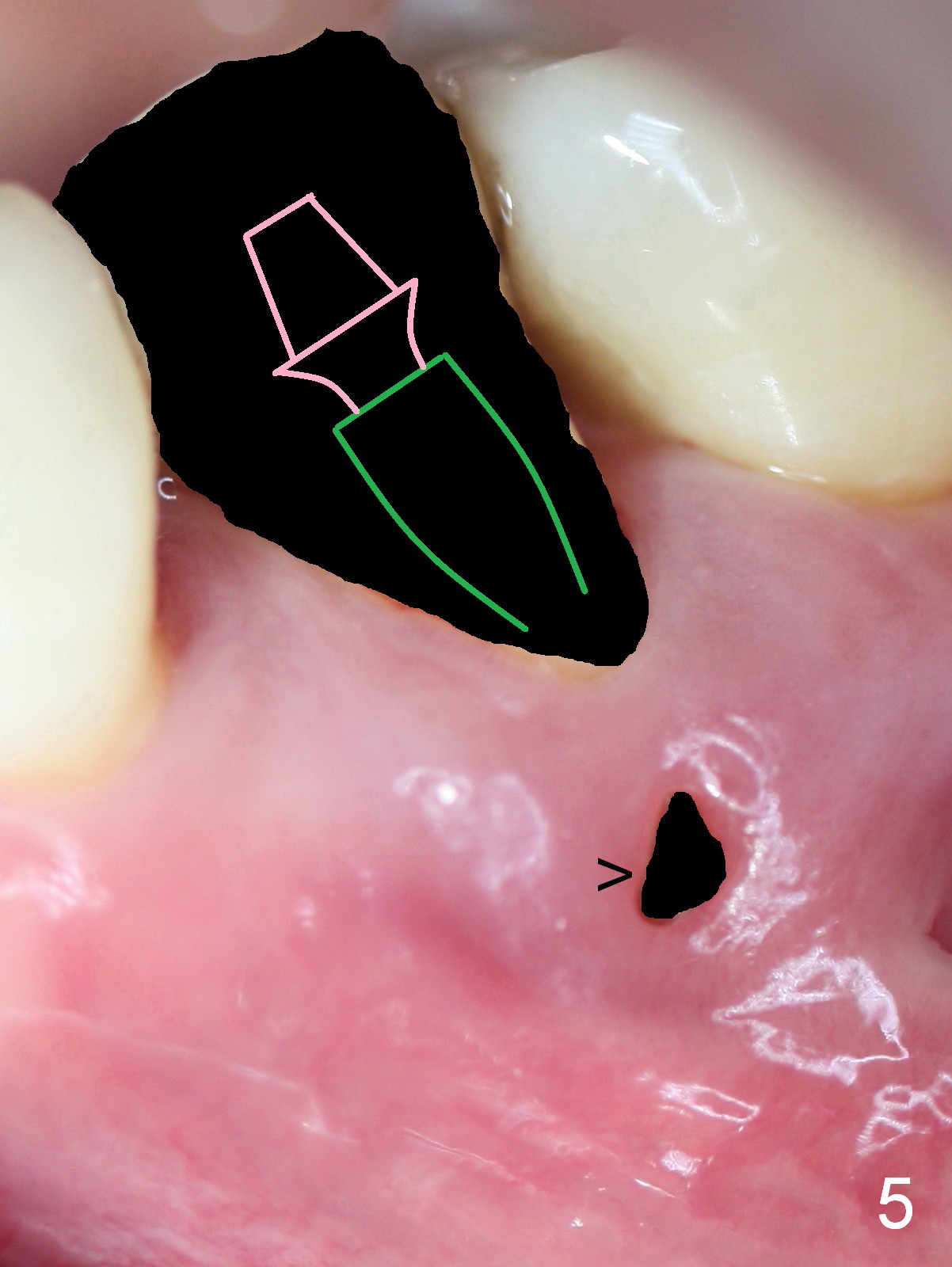
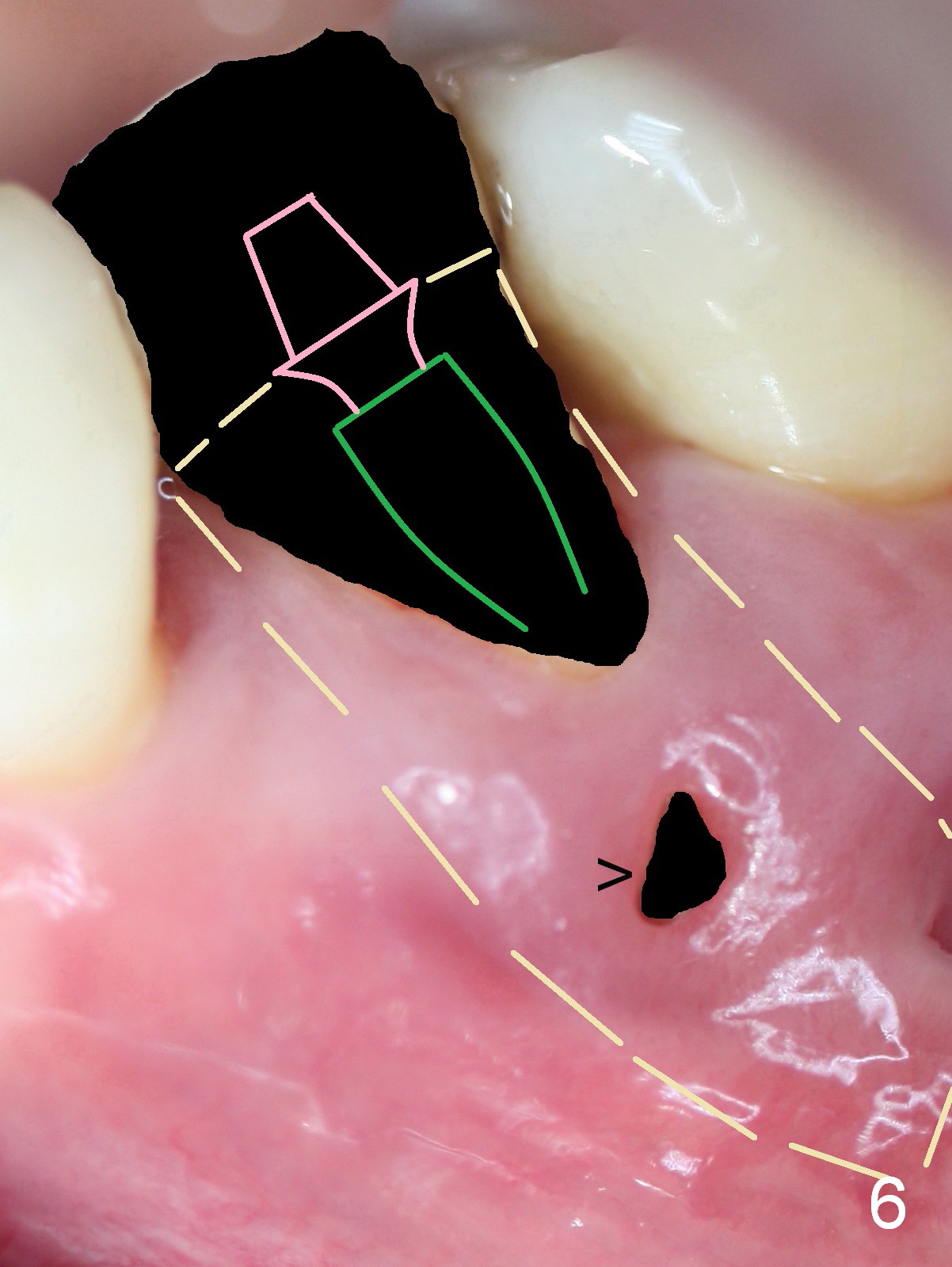
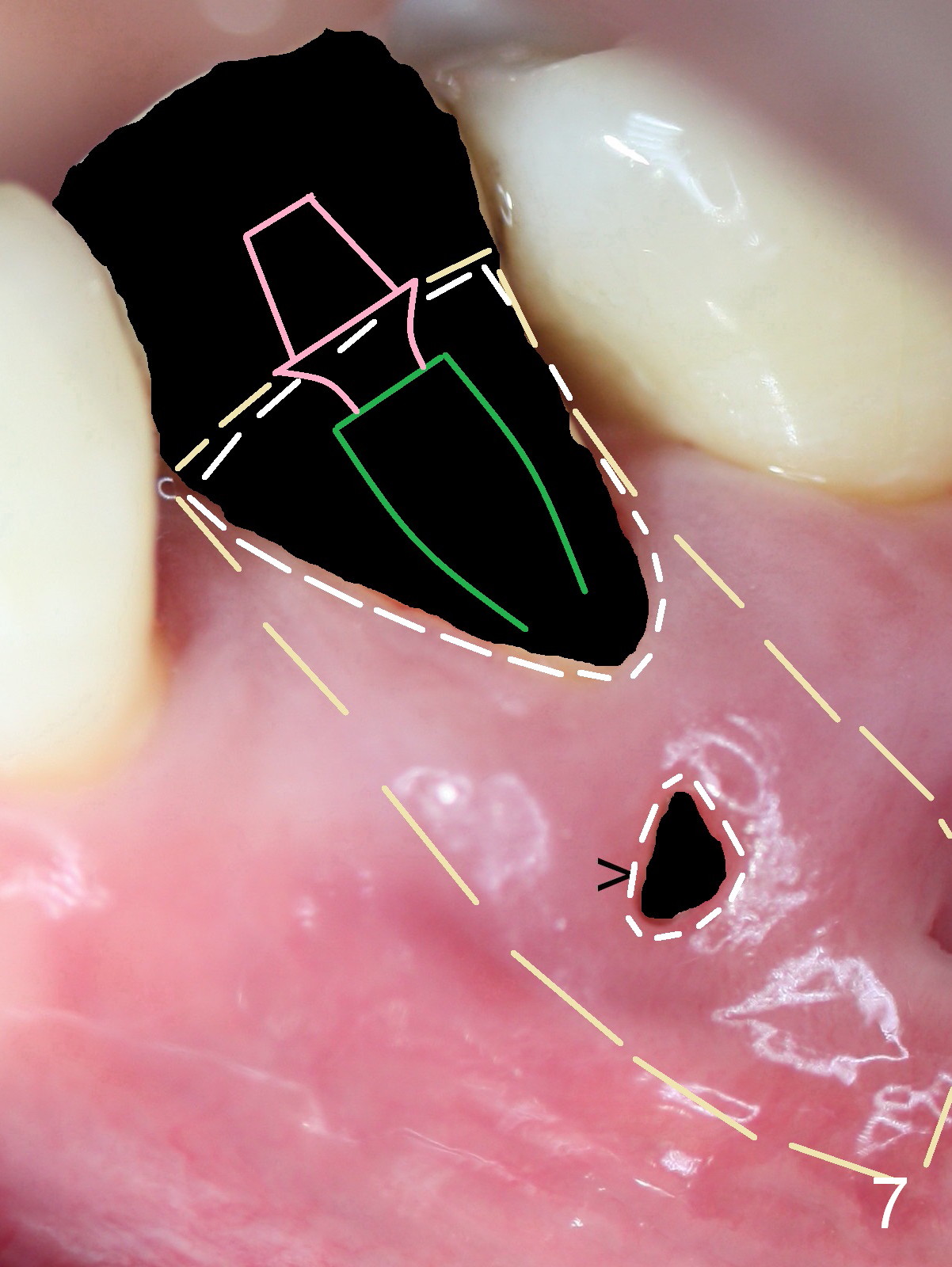
Fenestration Repair
A 45-year-old man (JT) has endo failure at #20 with fenestration (Fig.1,2 black >) and fistula (white <). Insertion of a Gutta Percha at the fistula (Fig. 3 <; PA taken 2 years ago) indicates that the infection is dervied from the apex of the tooth #20. The socket will be soaked with 2% Xylo, 1:50,000 Epinephrine gauze. A 4.5x17 mm tissue-level (Fig.4) or 14 mm bone-level implant is placed as lingual as possible (Fig.5 green). If primary stability is achieved, an abutment is placed (pink). A large piece of resorbable membrane is used to cover the buccal defect (including buccal recession, fenestration and fistula (Fig.6 yellow dashed line). Two small pieces of non-resorbable membrane are placed to cover the gingival recession and the fenestration (Fig.7 white dashed line, buried underneath the edge of the gigniva). Then place bone graft buccally. Place a small piece of gauze (one layer) or plastic (from Tatum implant bag) over the 2nd membrane over the gingival recession and fabricate an immediate provisional. When the acrylic is partially set, remove the gauze or plastic from the provisional. After trimming and polishing, the provisional is cemented to securely keep the 2nd membrane in place. When the wound is healing and the 2nd membrane is stable, trim the buccal extension of the provisional. It is expected that the buccal hard and soft tissue will regenerate over the implant.
Return to Lower Premolar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 08/28/2015, last revision 01/26/2019