,%205x14.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Implants in Narrow Crest
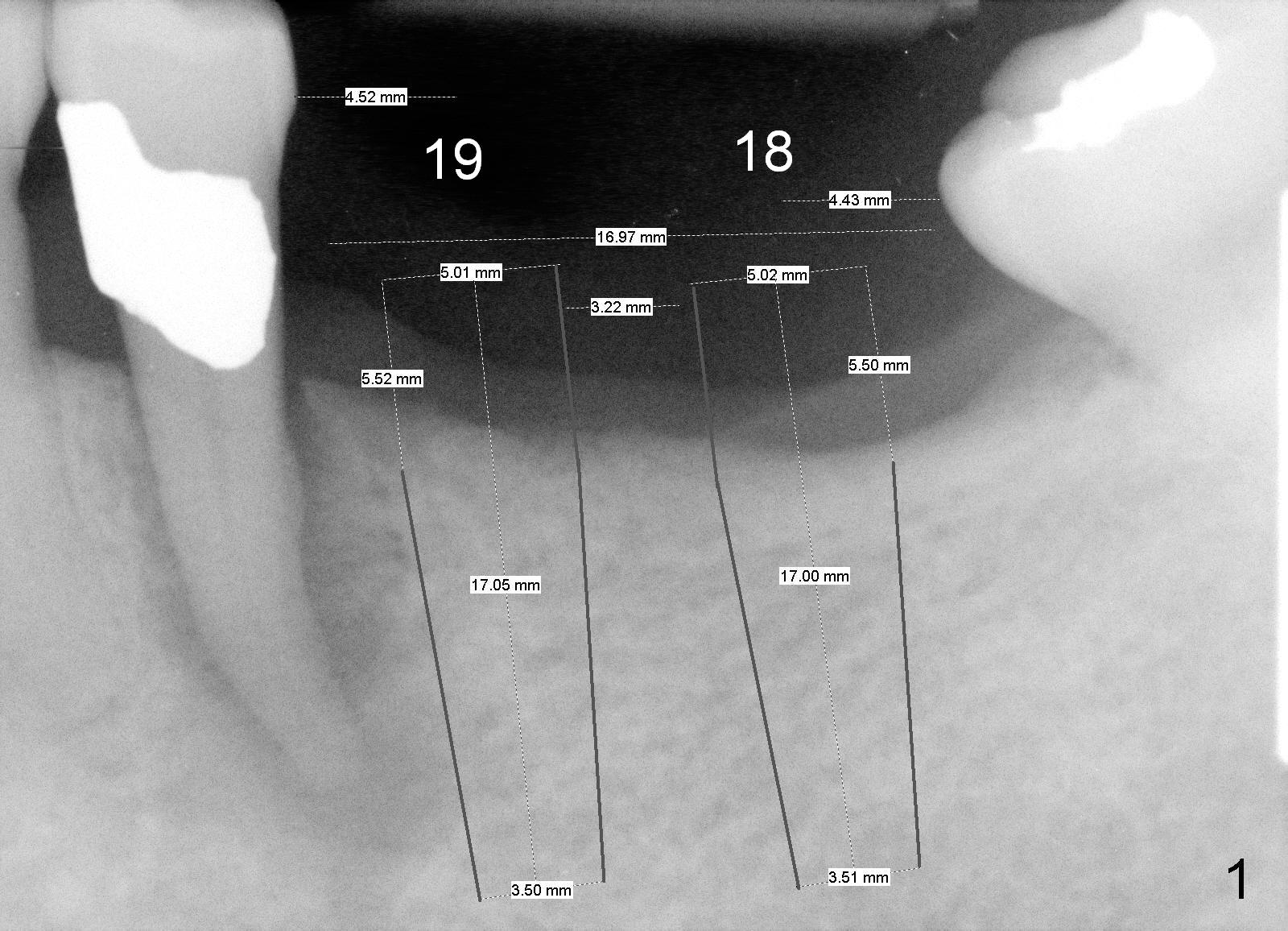
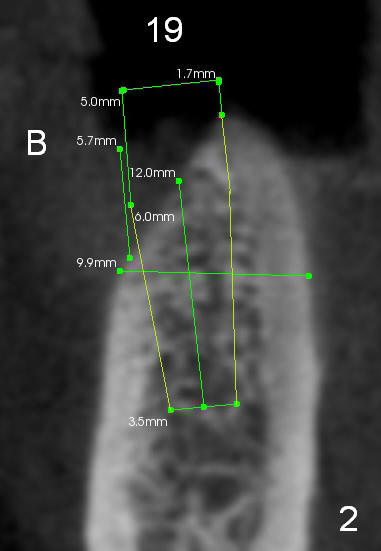
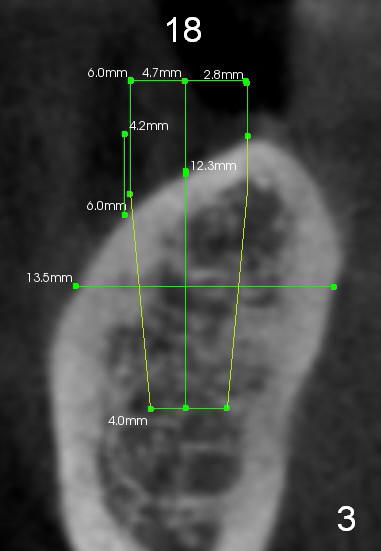
A 57-year-old lady needs implant placement at the sites of #18 and 19 (Fig.1). It appears that 5x17 mm implants are feasible, but CT coronal sections show that there will be substantial buccal implant exposure (Fig.2,3). Ideally smaller implants should be placed as lingual as possible.
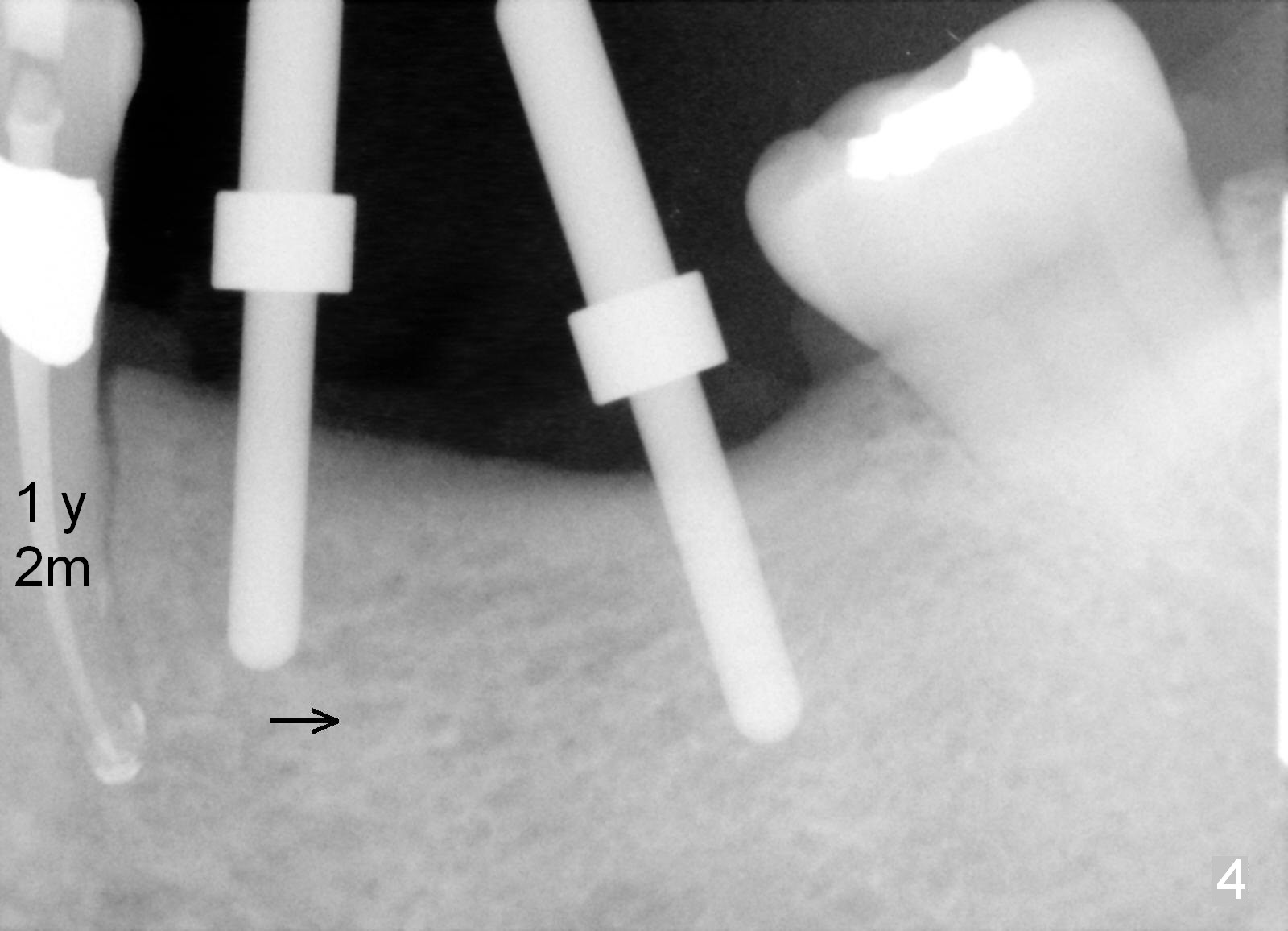
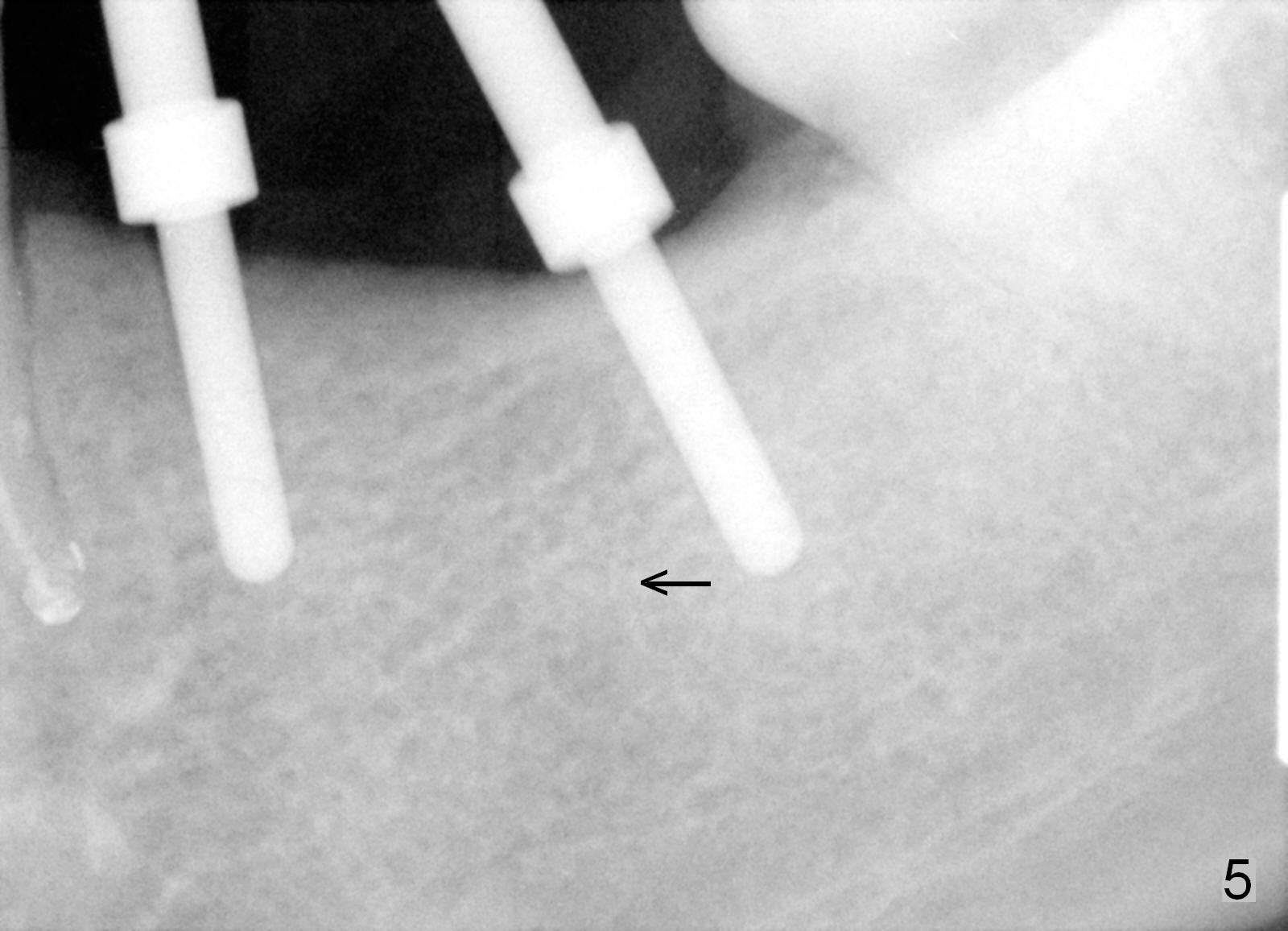
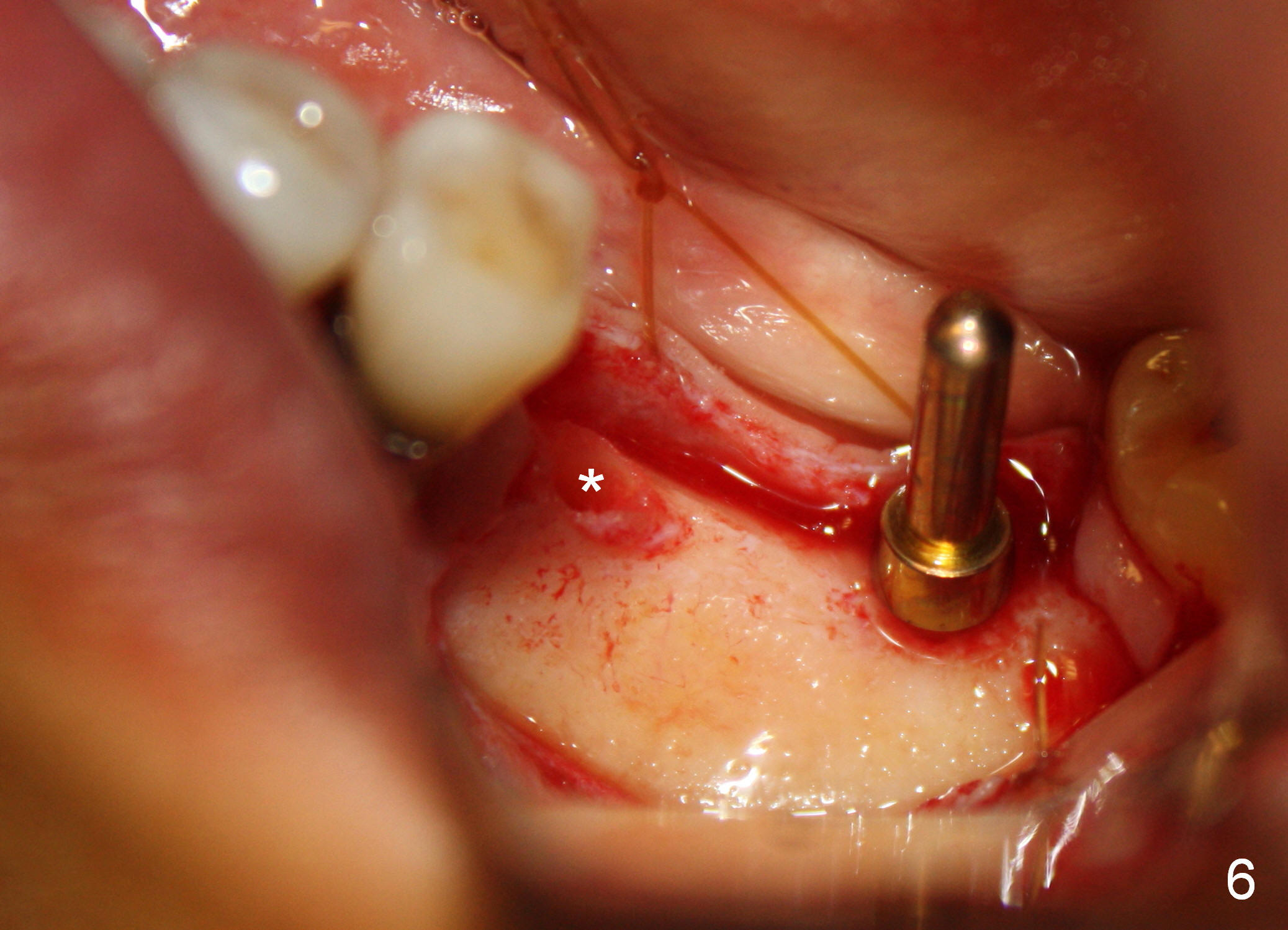
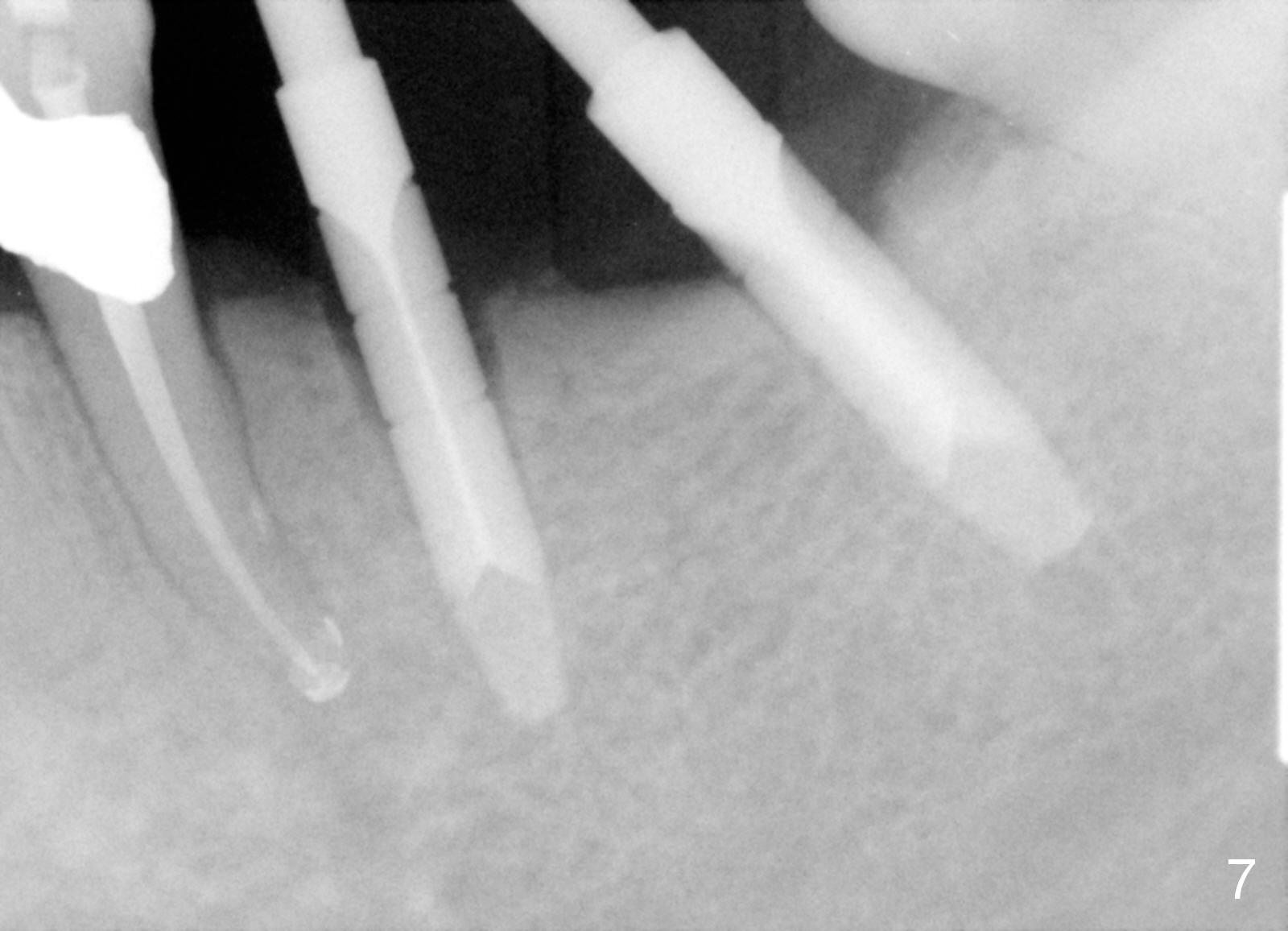
One year 2 months post root canal therapy at #20 (Fig.4), osteotomies are initiated at #18 and 19. The trajectory at #19 is subsequently corrected (Fig.5); that of #18 should be also corrected (arrow). The fact of the narrow ridge (Fig.6) is also ignored intraop. Without further adjustment, the osteotomies are enlarged (Fig.7) and the implants are placed (Fig.8: 4.5x14, 5x14 mm). As expected, the buccal coronal implant surface is exposed. The buccal plate is decorticated with placement of autogenous bone graft. Periodontal dressing is applied. Postop, the wound is infected with wound gapping. With irrigation, the wound finally heals.
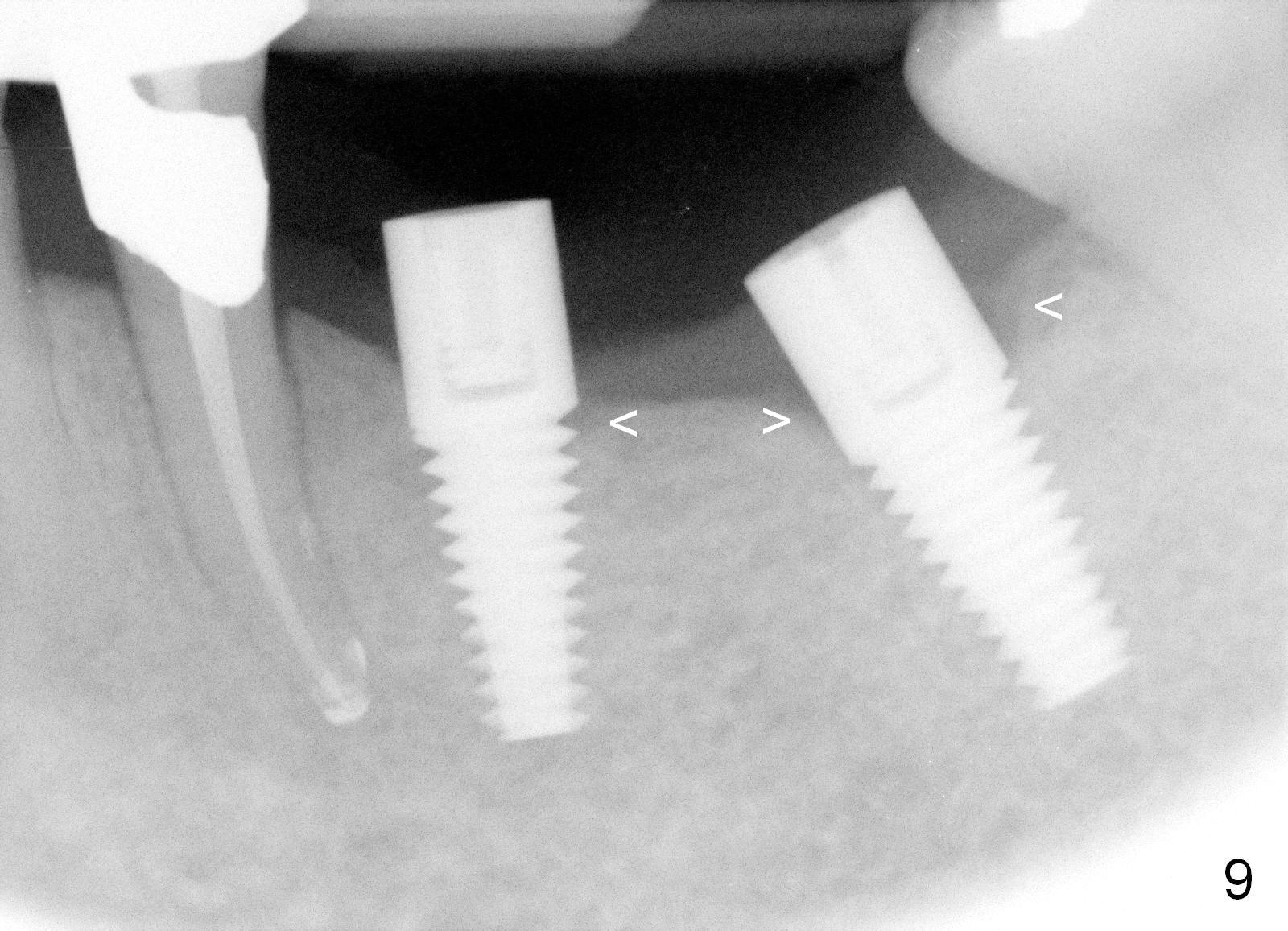
Three months postop, crestal bone has started to resorb (Fig.9 arrowheads). Resorption gets worse over time (Fig.10: 4 months post cementation, 11 months postop) (Fig.11: 1 year 2 month post cementation). On the other side (#30), postop bone resorption is not so severe. The patient's main concern is that she does not have normal taste ever since she got the implants.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/24/2015, last revision 01/19/2018