|
|
|
|
|
|
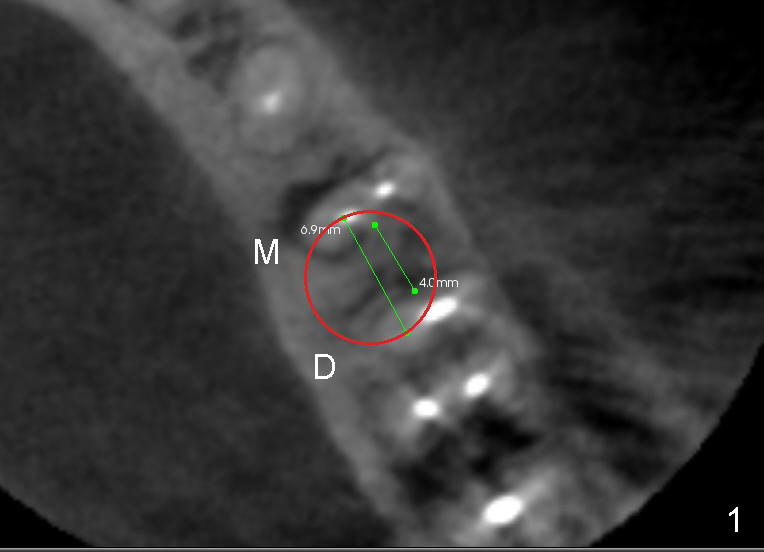
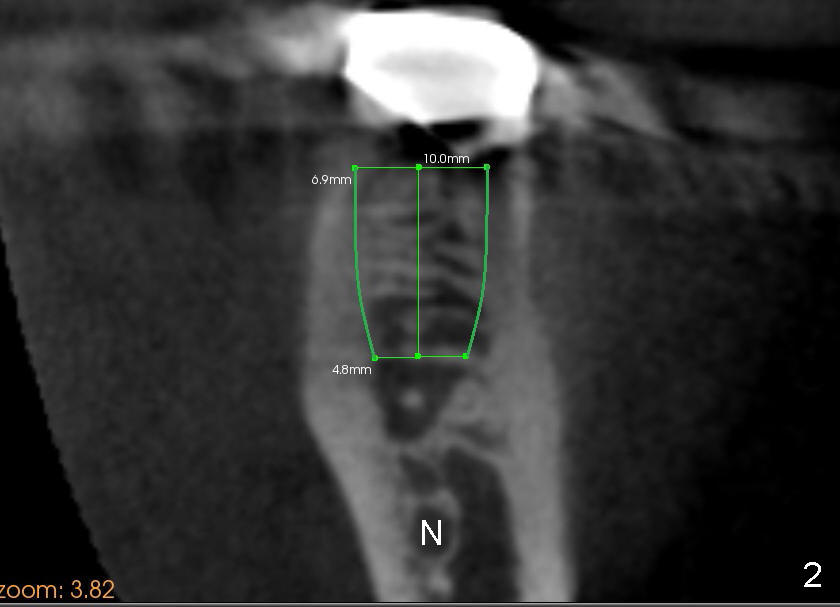
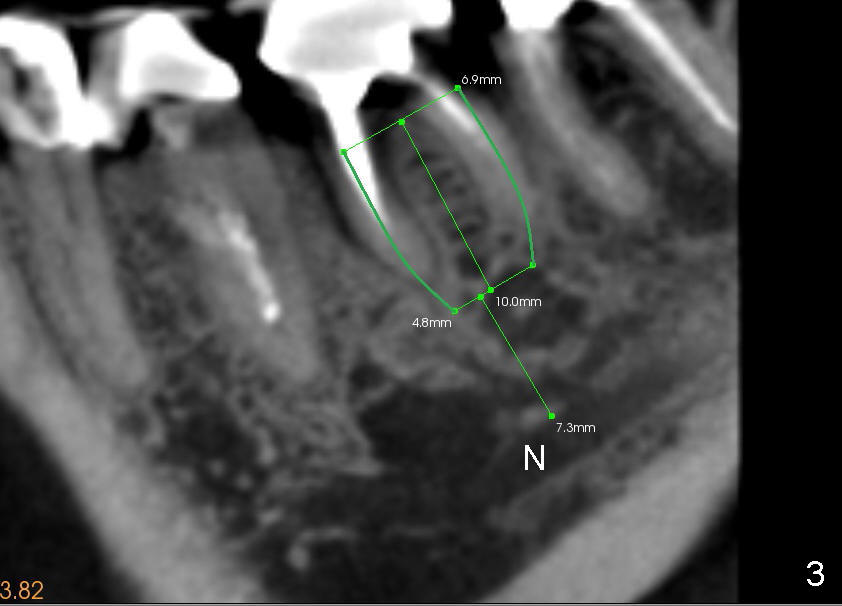
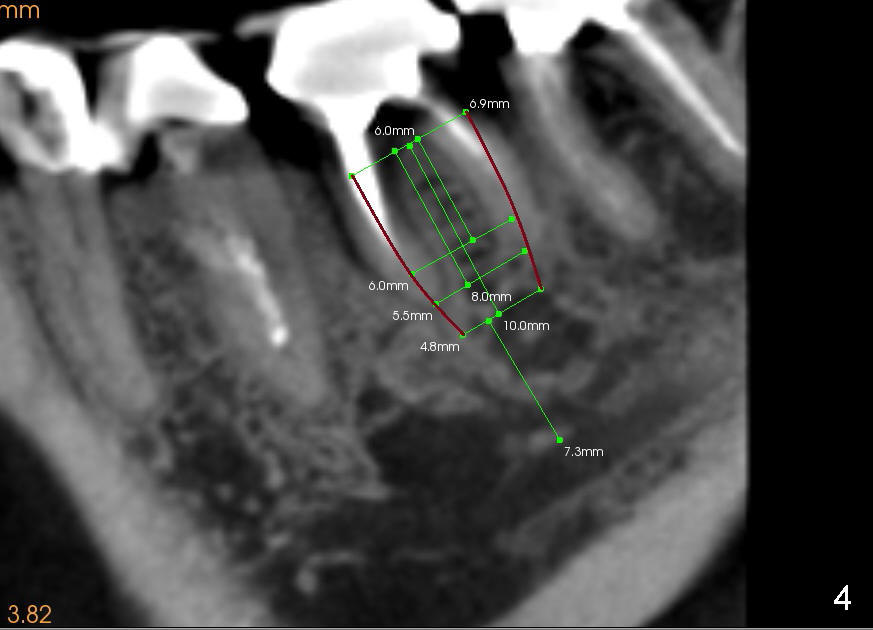
Harvest Bone and Healing Abutment
A 60-year-old man has difficulty chewing with the lower left 1st molar, which may have root fracture. CBCT is analyzed for implant placement in the septum. The latter is sectioned by thin blade osteotomes, as indicated by 6.9 mm green line in Fig.1 (axial section). The sectioning creates a slot and makes it easy to start osteotomy with a 2.0 mm pilot drill and a series of reamers in the middle of the septum (Fig.2 (coronal section), 3 (sagittal)). The mandibular bone has high density. It may be hard to finish osteotomy with osteotomes. Instead, reamers are used to form osteotomy and at the same time to harvest bone. The autogenous bone is then mixed calcium sulphate to be grafted in the remaining mesial (M) and distal (D) sockets before and after implantation. To form a tapered osteotomy (green outline in Fig.2,3) with relatively straight reamers, the latter should be used in a step back fashion. For example, the 2.5-4.5 mm reamers are to be used to create osteotomy at the depth of 11 mm, 5.0 at ~ 10 mm, 5.5 at 8 mm, and 6.0 at 6 mm (Fig.4). A 7x14 mm tap is used at the depth of 11 mm to create threads and test stability before placing 6.9x10 submerged tapered implant. A 8 or 9 mm healing abutment is used to cover the socket. There will be spaces mesially and distally, which are to be closed with sutures, supplemented by perio dressing.
The surgery turns out to be different from the design.
Xin Wei, DDS, PhD, MS 1st edition 03/06/2014, last revision 03/08/2014