Immediate Provisional Closes
Molar Socket
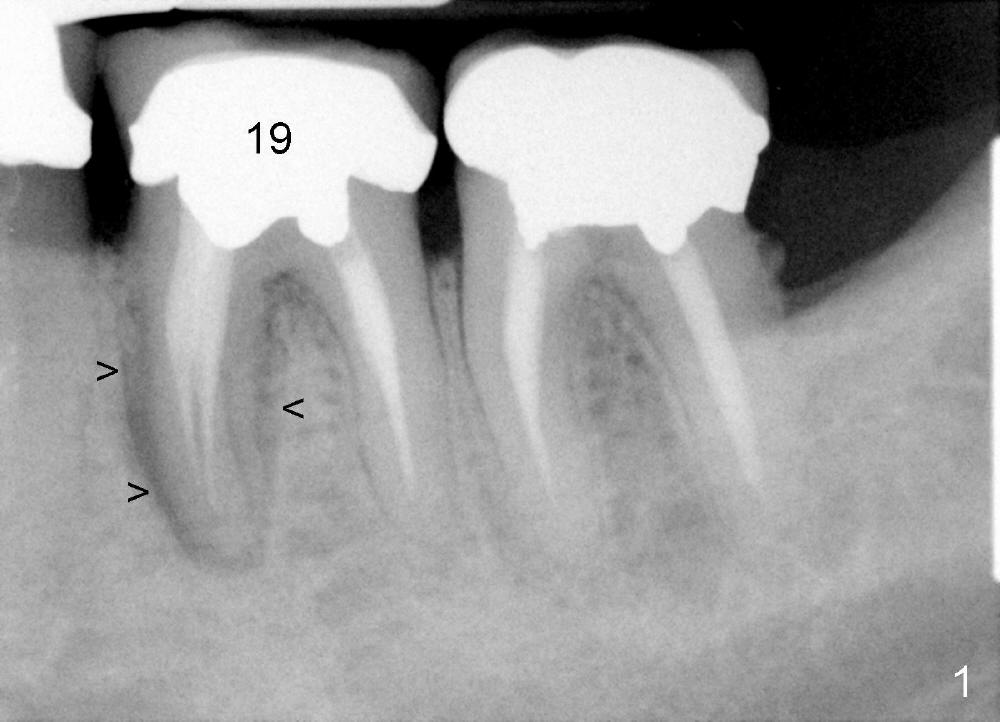
The tooth #19 is symptomatic. The diagnosis is consistent with fracture
of the mesial root (Fig.12): large radiolucency (Fig.1 >) and a mesiolingual fistula
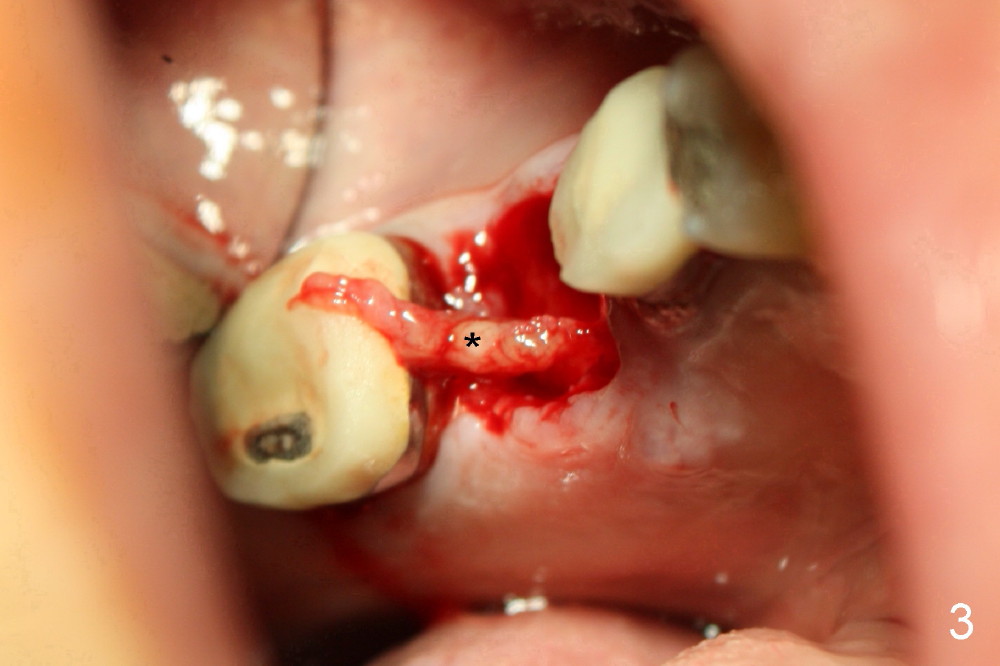
(Fig.2 (lingual view) *). There is granulation tissue attached to the mesiolingual aspect
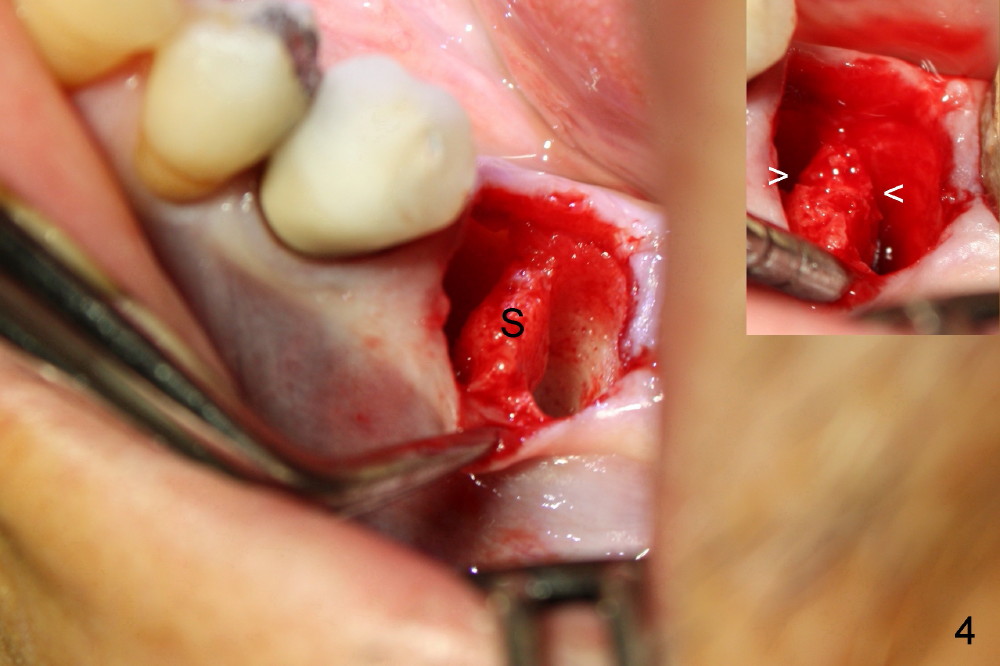
of the socket (Fig.3 (lingual view) *). After thorough debridement of the socket, the
septum (Fig.4 (buccal view) S) is sectioned by thin
osteotomes as indicated by arrowheads in Fig.4 insert.
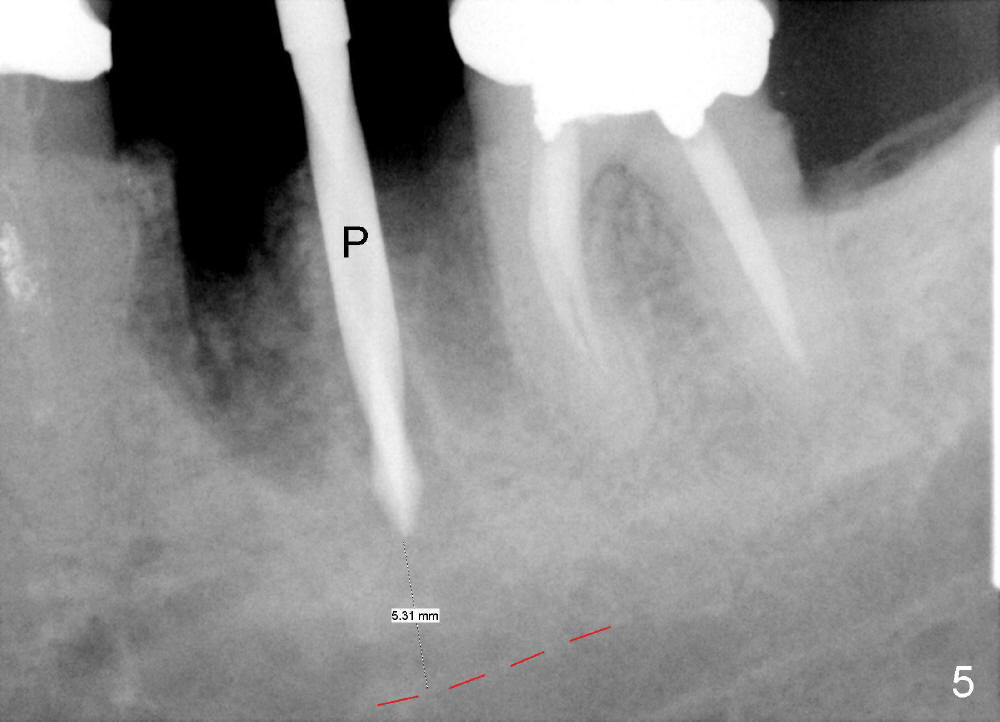
The sectioning makes it easy for a 2 mm pilot drill (Fig.5 P) to penetrate the
septum without sliding into either the mesial or distal socket. The osteotomy is enlarged by reamers from 2.5 to 4 mm at the depth
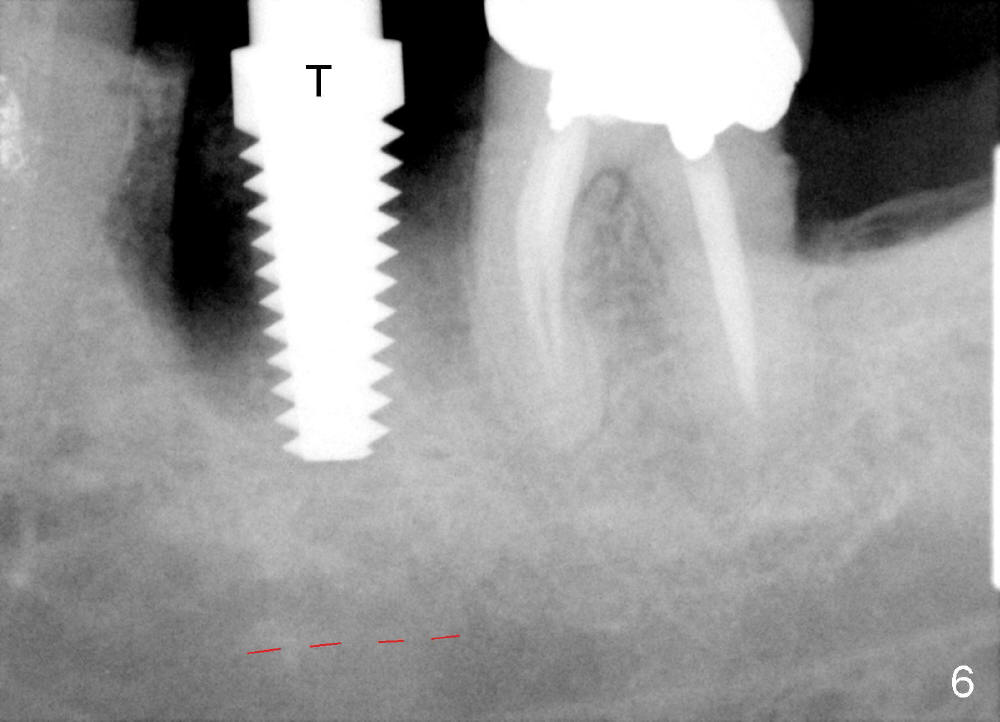
of 11 mm (from the crest of the septum). A 6x17 mm tap (Fig.6 T) lacks
stability at the depth of 14 mm from the gingival margin. Since there is
distance from the upper border of the inferior alveolar nerve canal (Fig.6 red
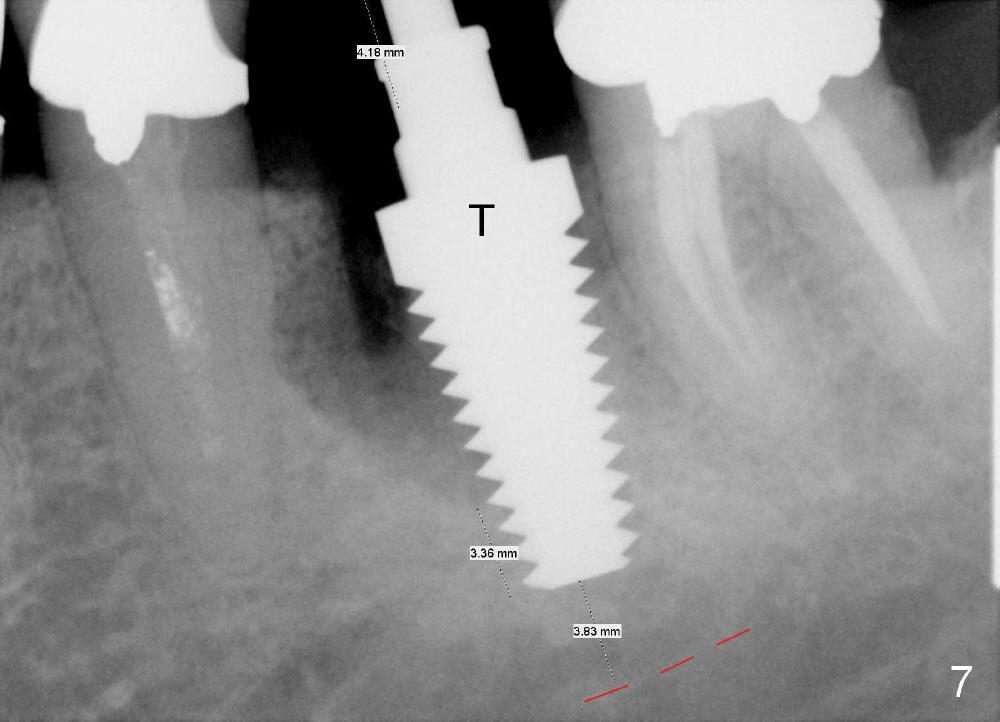
dashed line), the length of the osteotomy can increase by 3 mm. By the time a
7x17 tap (Fig.7 T) is inserted at the gingival level, it has sufficient
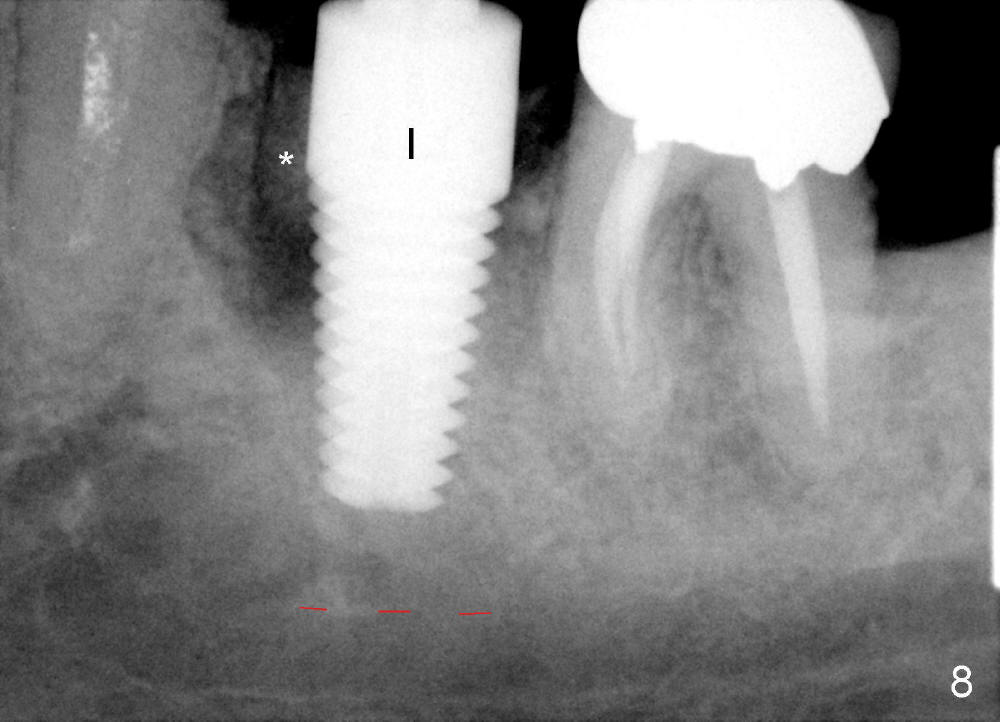
stability. The corresponding implant has insertion torque >60 Ncm (Fig.8).
Mixture of autogenous bone (harvested from reamers) and Osteogen (Implandent) is
placed in the periphery of the socket prior to and after implant placement
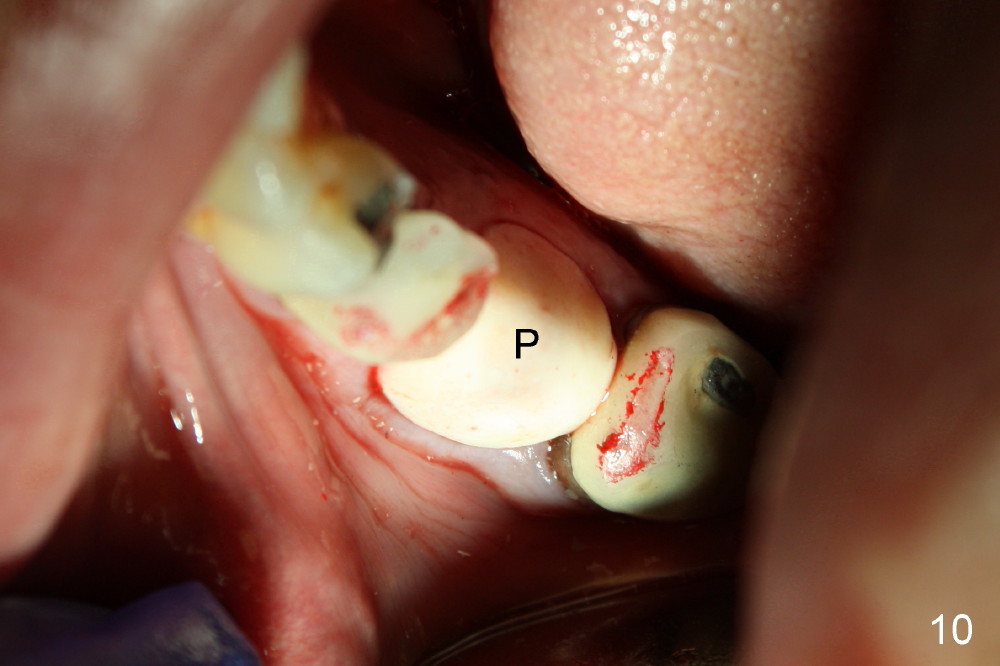
(Fig.8,9 *). To contain the graft in place, a 4x3 mm abutment is placed
(Fig.9 A) and an immediate provisional is fabricated (Fig.10, 11 P). There is no
need to raise flaps or use sutures to close the socket. To avoid micromovement
of the implant, the occlusal
surface of the provisional is reduced so that there is no occlusal contact in
any excursion (Fig.11). As the wound heals, the tissue surface of the
provisional may be adjusted to have normal gingival contour.
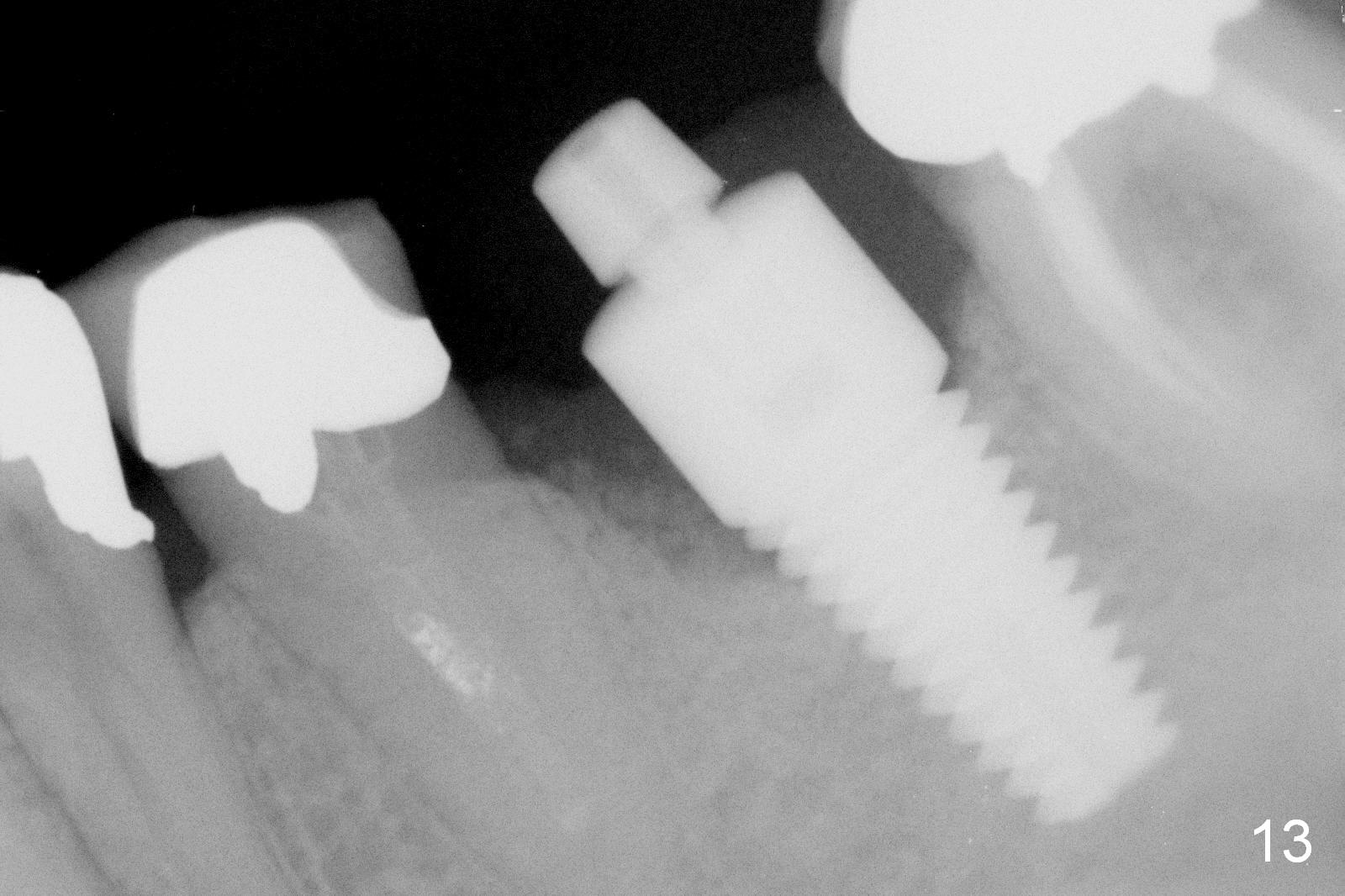
When the patient returns 18 months postop, the mesial portion of the
provisional is lost with loosening abutment with bone fill in the mesial socket
(Fig.13). The distal socket density increases.
03/15/2014 J Shaped Radiolucency
冬生,Dr.魏,Dr. 田:
同学们:
你们好!近几年来,我积累了许多例有关“ J shaped radiolucency"。此题目很有临床意义与`价值。文献与最新版的 Pulp
pathways 都有提到它。最近两个月,我手头就有五例 “J 型阴影...”,结局都是拔牙,植骨与 implants. 尤其是本周就有两例。都由哈佛的
endodontist 处理,几周前刚做的 retreatment 或根切加retrofilling,
但最終病变对治疗都无有利反应,反而出现越来越大的脓肿。“J 型阴影" 就一定是 root fracture 吗??上述病人一个月前来我诊所, 要求
endo retreatment。 经 PAs 检查,很明显是 J 型阴影,我在会诊中告诉病人很有可能此两颗牙都是 root fracture, 于是
要求病人签字: 如在 retreatment 或 探查中发现有 root fracture 可能需拔牙,他不接受。于是我把他转诊到 哈佛的
endodontist, 我在转诊单上写明“ J shaped..."。专科医生接到 case 后, 连问都不问就做了起来,一例做根切加retrofilling,一例做顺向
retreatment, 结果两例都无有利反应,又转回来拔牙和 implants. 病人多花费 over $ 1000 还加上 insurance
benefit.,还遭受额外的痛苦。 病人很不高兴。上周那位哈佛的 specialist 打电话过来商量病例,我问她仔细读过我的转诊单吗?她說
"Yes. ". 当我提到我的具体的 documentation有关 “J shaped ..."时,
她真的丈二和尚摸不着头脑,一无所知。可惜她是个女的,又是老外,不适用吧?我深知我是 GP, 什么是我的份范与分寸,
但我更知道做人要自强不休与努力不息!无论如何最终我还是帮了她忙,我知道她心里想什么。
这是个很有意思的题目,可以让病人少吃苦头,如何掌握分寸?
据我所知,冬生早早熟知此 topic, 是否考虑在 Email
上讨论一下,大家讨 论出个有意义的规范。最近许多事搅和在一起,我实在太忙,我要等到六月中旬后,才有时间写我的体会, 经验与有关的处理途径。
如果有人觉得打扰你了, 敬请删除,并接受我的诚恳的致歉。
敬颂
方炳忠
Dear Dr. Fang:
It is an excellent topic.
Would you give us a list of this type of defect in X-ray? It is difficult
to make diagnosis, even when the tooth is extracted? The crack is shown
only after the tooth has been bleached for a while. I have published a case
similar to yours.
http://www.xinweidds.com/. Professionals, Immediate Implant (in the
first line), under Case Table: lower Molar, under Case Table again: 1st
molar, Root Fracture, Provisional. Thanks.
2014_03_16
03/18/2014
海雄兄:
你好!谢谢你的复件。
这个问题有两个层面:第一个是 clinical judgement; 第二是
怎么处理,即:途径,策略,方法和临床实践。作为一个专科医生并不应该什么病例 到手就做的。对于 J- shaped
radiolucency,我转诊的医生都是我们南加州 top level 的, 至少有三个。但他们中竟没有一个对此经过认真考虑而对病人作较为认真的
consultation,而是病例一
到手就做。这几个病人结果没一个不后悔的,当初没有听从我的advice。如果行医是单纯的商业行为,那是医学的悲哀。而且我觉得医术与职业操守是紧密相联的。对于J-
shaped radiolucency, 什么时候什么情况下可以试做或探查是需要有比较良好的临床判断能力的。如果明确是 vertical
fracture 是没有任何转诊价值的。正如我的前几天报导的,我转诊的唯一理由:病人不愿接受可能拔牙的事实。而不是讓specialist
去做一件不可能实现的事。无论是顺向或逆向的 retreatment 我本人都非常胜任而且confident,绝不是技术上原因而转诊
。我的本意是让specialist和我一起,让病人接受一个可能拔牙的事实而不是“ 让他们病例一 到手就做”。 在转诊单上,我明确地写上:“
consultation and tx if needed".
但很不幸,他们中竟没有一个有过任何的顾虑与犹豫对于损害的转归。
海雄兄,你提到的病变与我讲的,可能不是一回事。root fracture 与vertical
fracture, 有时不是同一的。这涉及很多。请参阅最新版的Pulp Pathways 与有关的文献。.
我很遗憾与感慨的是,在我和他们的对话中,竟没有一个对此病变认真考虑过,而是一无所知, 一问三不知,无言以对而告终。
昨天很匆忙,打错很多字,所以重新改写。六月之前,不会再有时间wechat 了。用午餐时间写了几行。再见。
谢谢!
方炳忠
Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 03/07/2014, last revision
01/19/2018