
,%20Vanilla.jpg)


|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
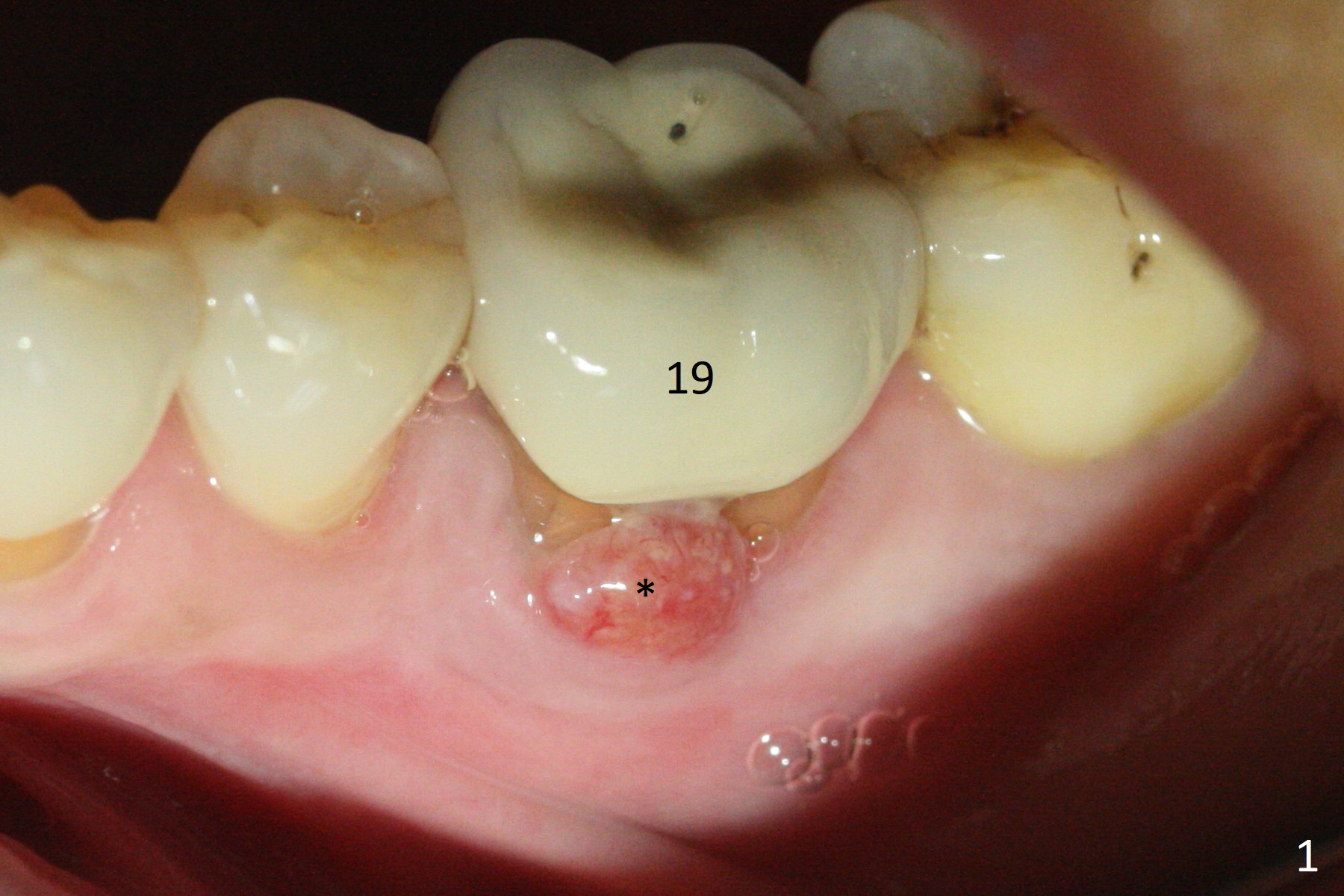
Bone Shorter than Expected
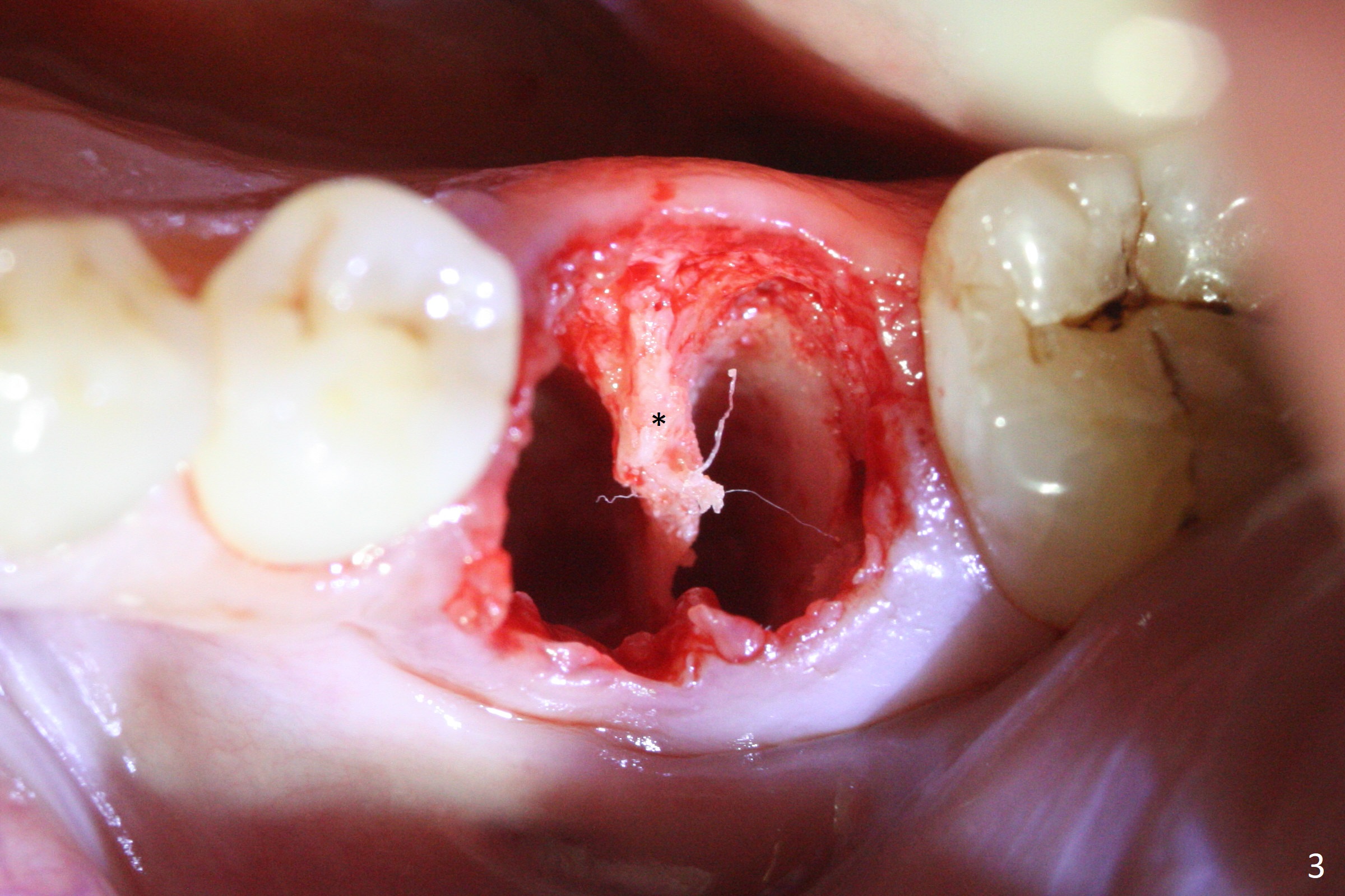
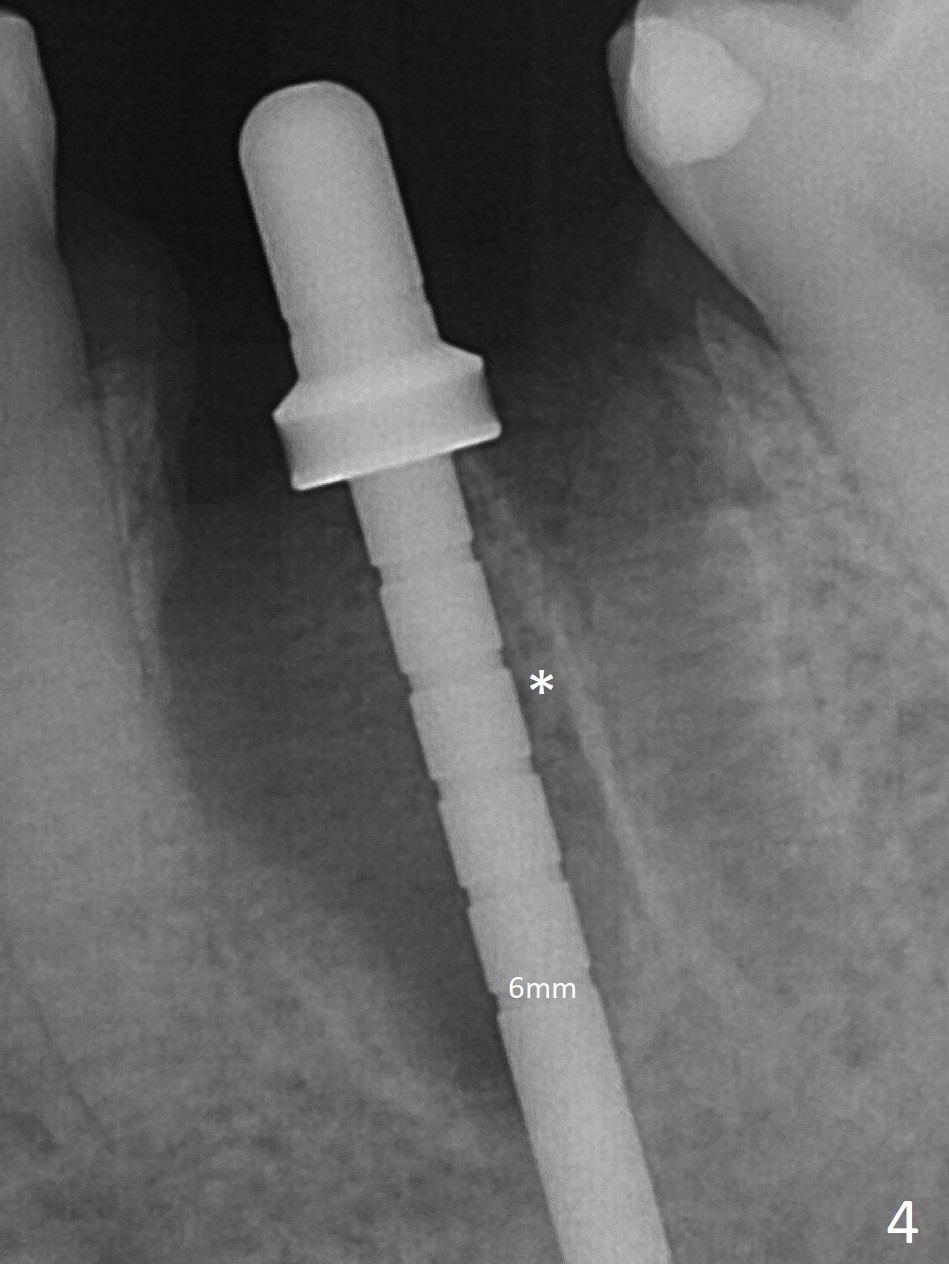
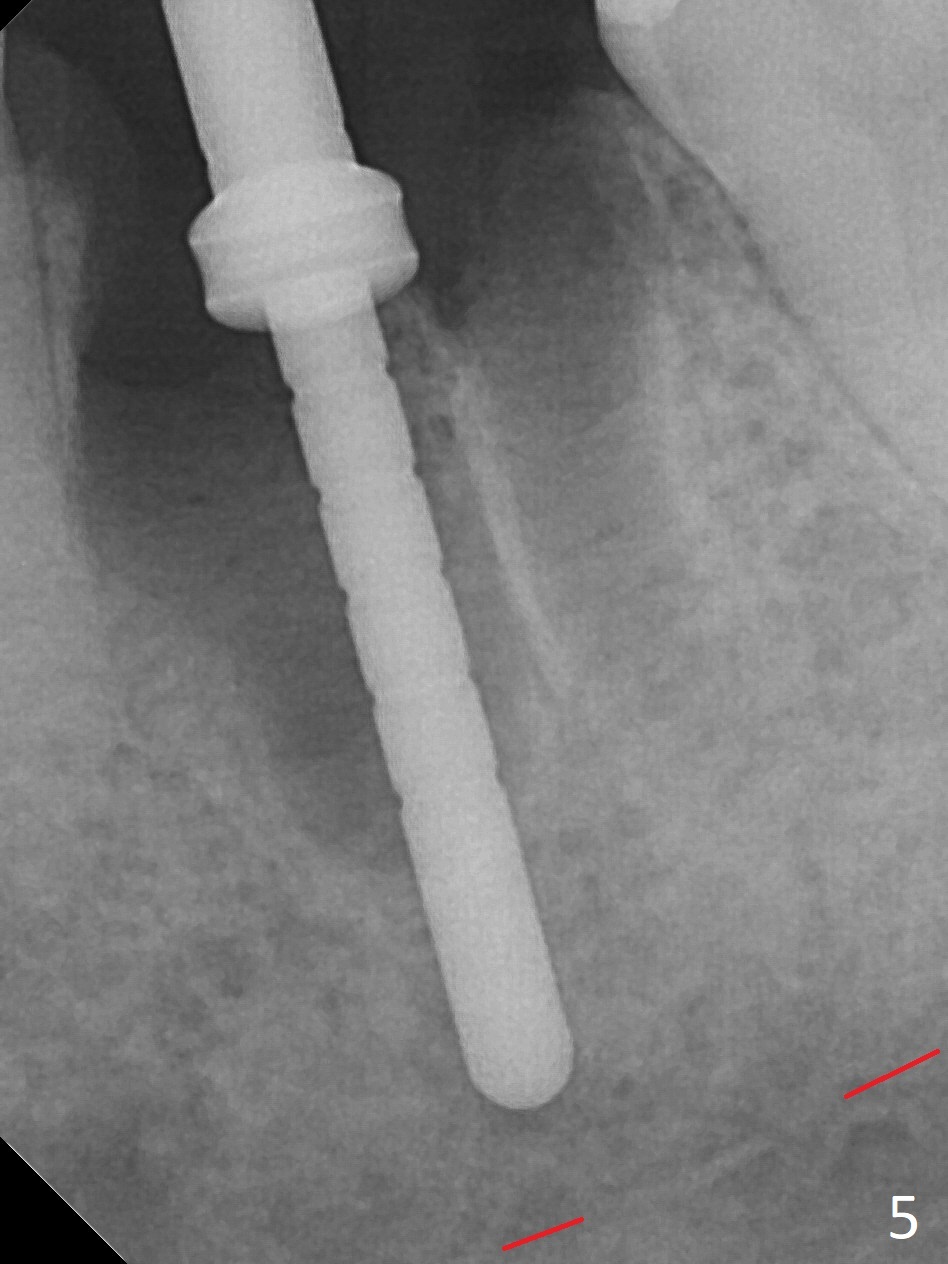
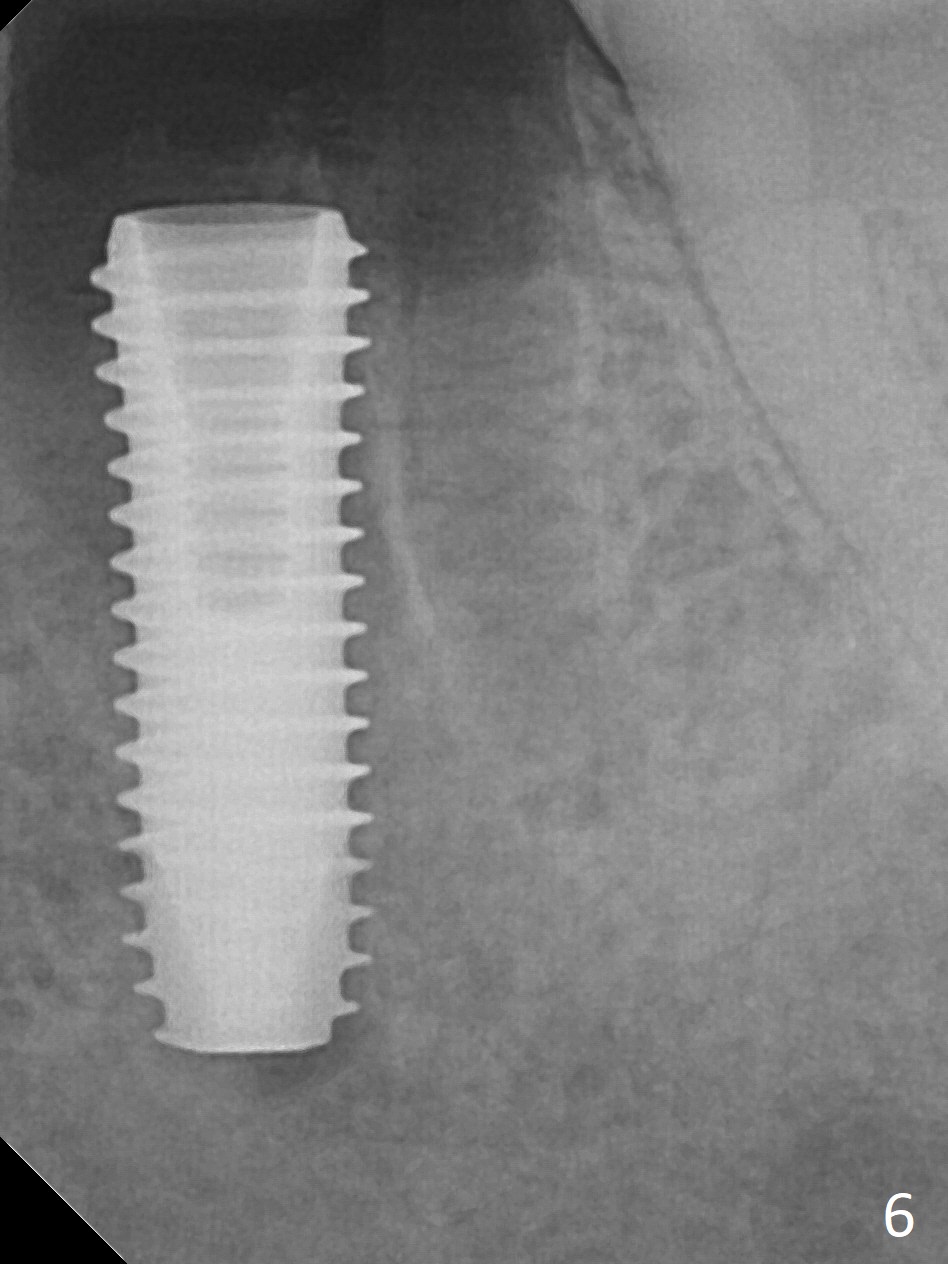
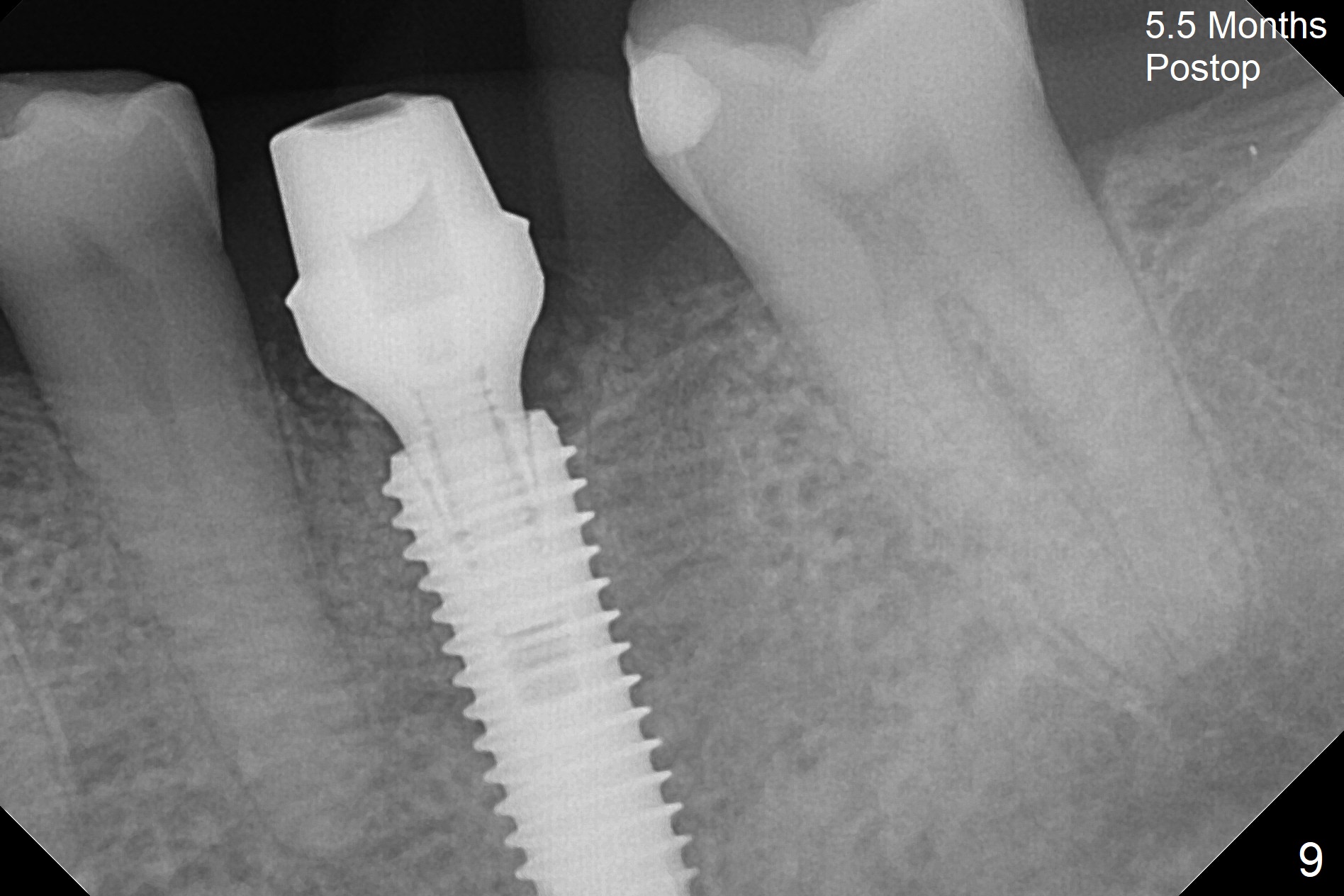
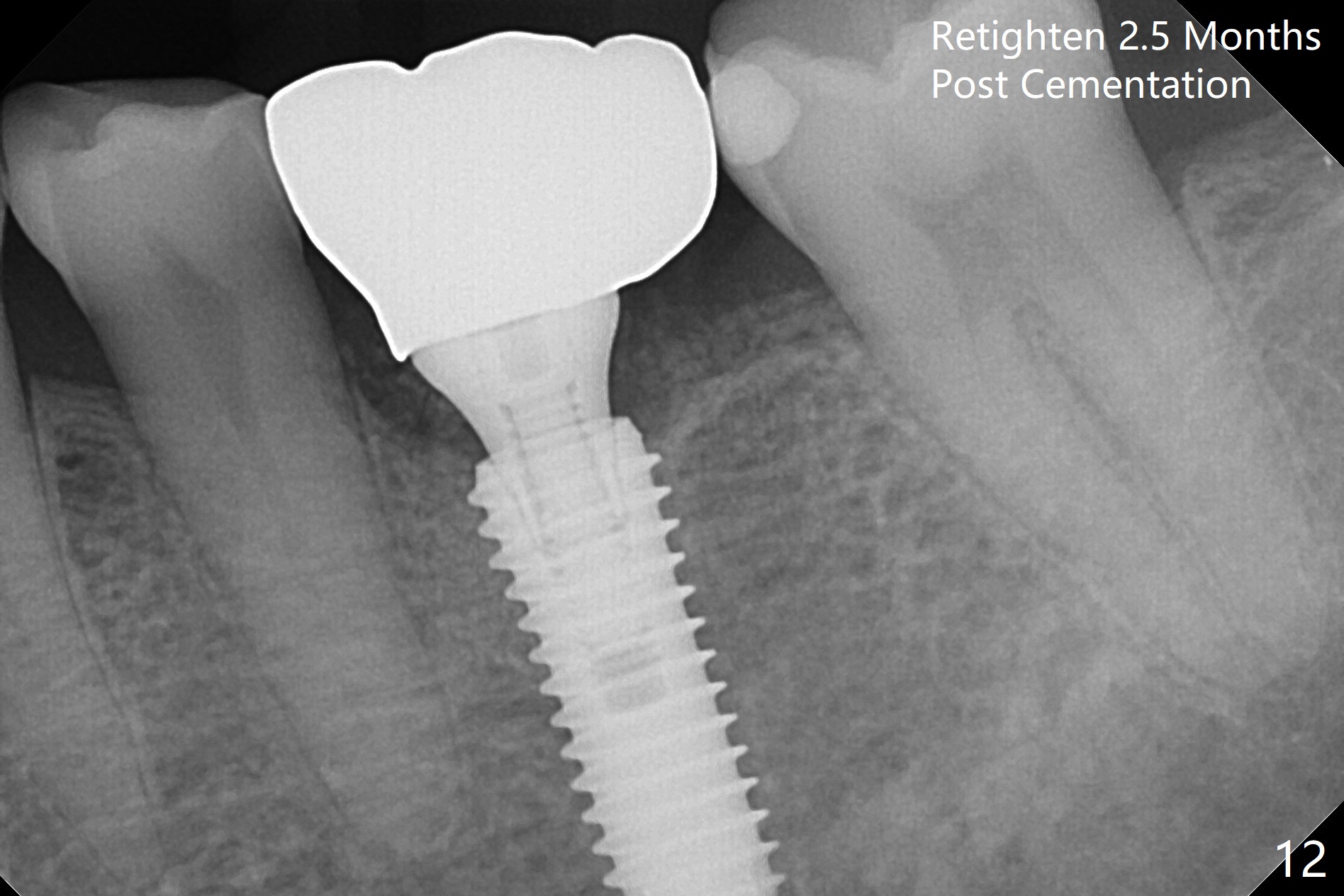
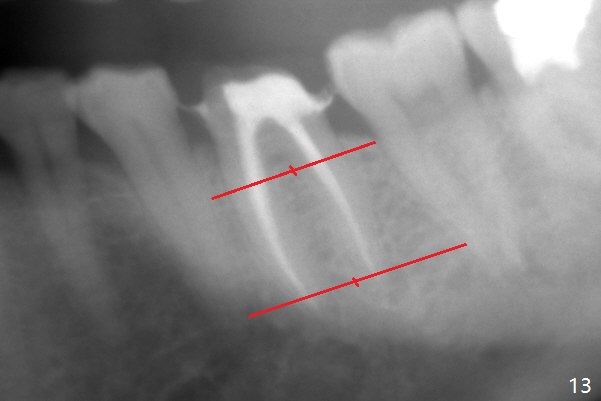
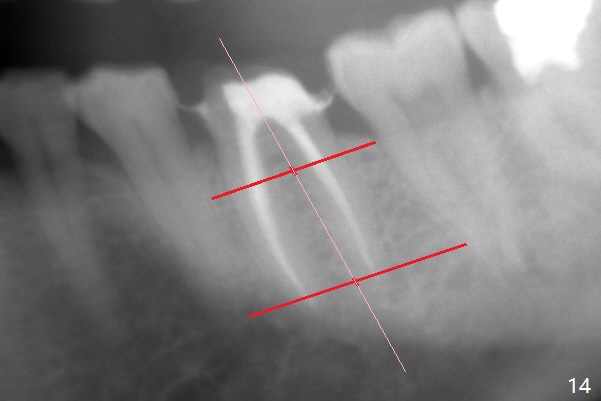
When the patient returns 9 months later, there is severe buccal gingival recession and abscess at #19 (Fig.1 *) with large mesial periradicular radiolucency (Fig.2 *). The septum is thin and the buccal crest is low after extraction (Fig.3 * (mesial root vertical fracture)). Osteotomy is initiated in the mesial socket immediately against the septum (Fig.4.5) with ~ 5 mm in the native bone. Due to severe buccal plate resorption, a shorter implant is placed (Fig.6; 5x15 mm in stead of 18 mm). There is at least 2 mm gap buccally for Vanilla Graft, which is also placed next to the implant and the neighboring root (Fig.7 *). There is clearance from the Inferior Alveolar Canal (Fig.8 red dashed line). Both the mesial and distal sockets heal 5.5 months postop (Fig.9), although the apical portion of the distal socket was not filled with allograft (Fig.7). The implant was placed mesial. The straight abutment (6.5x4(4) mm) (Fig.10) is changed to an angled one (5.5 x15 degrees 3 mm cuff (Fig.11)) before impression. The implant is also placed buccally. Therefore the implant position is far more important than its length. The abutment is retightened 2.5 months post cementation, which is related to mesiobuccal placement of the implant (Fig.12). An ideal trajectory is determined by drawing 2 horizontal lines (at crestal and apical levels: red lines in Fig.13), finding a central point of each line (vertical short line) and joining these 2 central points (Fig.14 pink line). In fact the ideal osteotomy should have been established distal to the septum in this case. Guided surgery may alleviate the issue. The crown is not loose, but the patient feels that the implant tooth cannot sustain mastication. In fact the screw is removed with hand driver (not wrench). The abutment hex is rounded and worn. A new 5.5x4(4) mm abutment is placed (without knowledge of previous use of an angled abutment) with mesial reduction to reduce undercut and buccodistal margin lowered to reduce gingival embrasure. It is that the straight abutment could decrease the chance of screw loosening. Otherwise the implant has to be removed for better trajectory.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments
Xin Wei, DDS, PhD, MS 1st edition 12/07/2017, last revision 05/05/2019