


|
|
|
|
|
|
|
|
|
|
18 mm Bone-level Implant
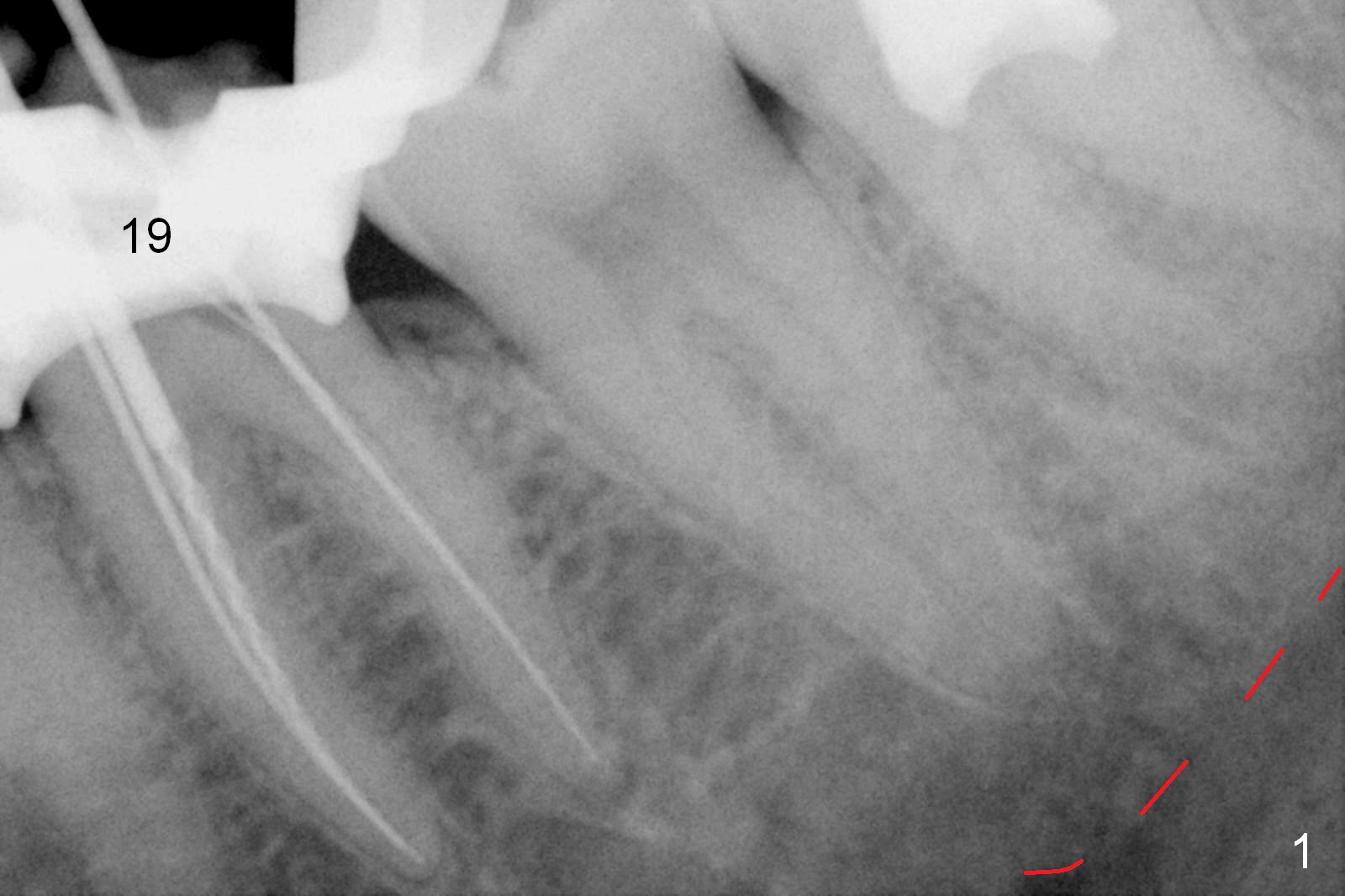
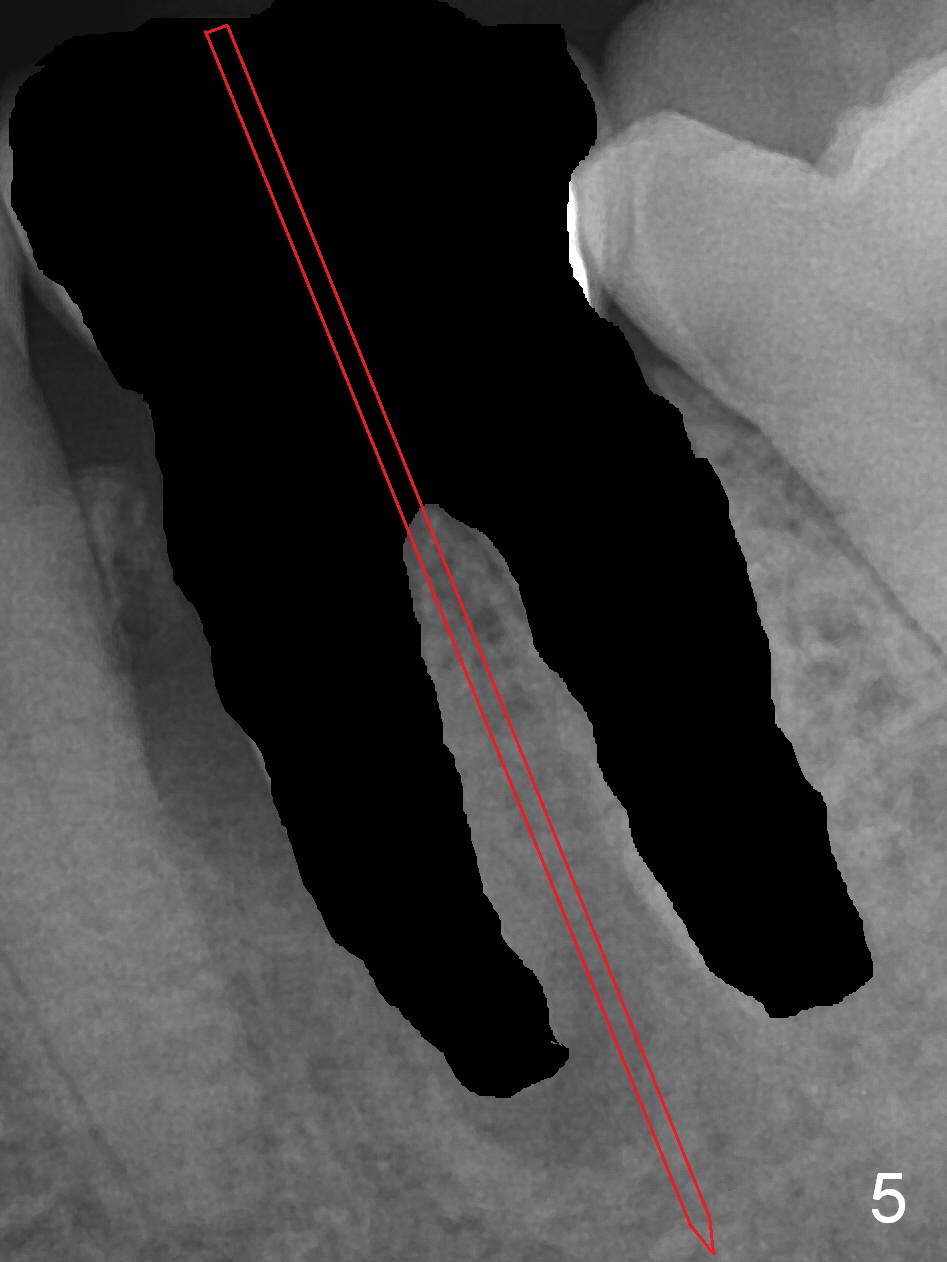
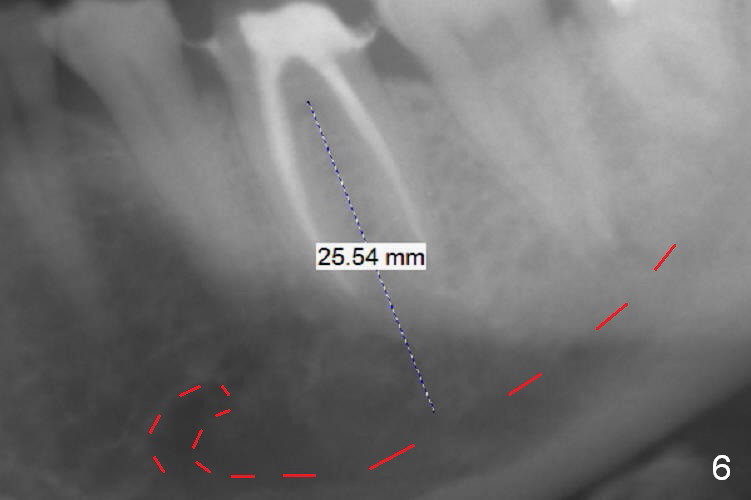
A 59-year-old woman had root canal therapy for the tooth #19 10.5 years ago (Fig.1 (red dashed line: the superior border of the Inferior Alveolar Canal). Two years later there was apparent periapical radiolucency with the distal root (Fig.2 *). The tooth remains asymptomatic until the last six months. There are 2 fistulae associated with the tooth: mesiolingual and buccal furca. Radiogra-phically, there are 2 radiolucent lesions: mesial and apical to the mesial root (Fig.3 *). If a 16 mm implant is placed, there will be approximately 5 mm apical bone (Fig.4); 7 mm for a 18 mm implant. The bone height is 25 mm (Fig.6). Therefore, once initial osteotomy is established with a 13 mm long drill with PA confirmation, the osteotomy is extended to its depth with 1.5x21 mm drill (Fig.5). After socket treatment with Metronidazole gauze with Epinephrine (1: 50,0000), take PVS impression of the socket to catch the large mesial defect. A fair amount of allograft and Osteogen is expected. It has been 9 months since last visit. Retake PA before surgery. If the mesial defect enlarges, start osteotomy in the distal slope of the septum.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), Armaments
Xin Wei, DDS, PhD, MS 1st edition 03/05/2017, last revision 03/04/2018