.jpg)

|
|
|
|
|
|
|
|
|
|
|
Use of Allograft or Not for Narrow Ridge
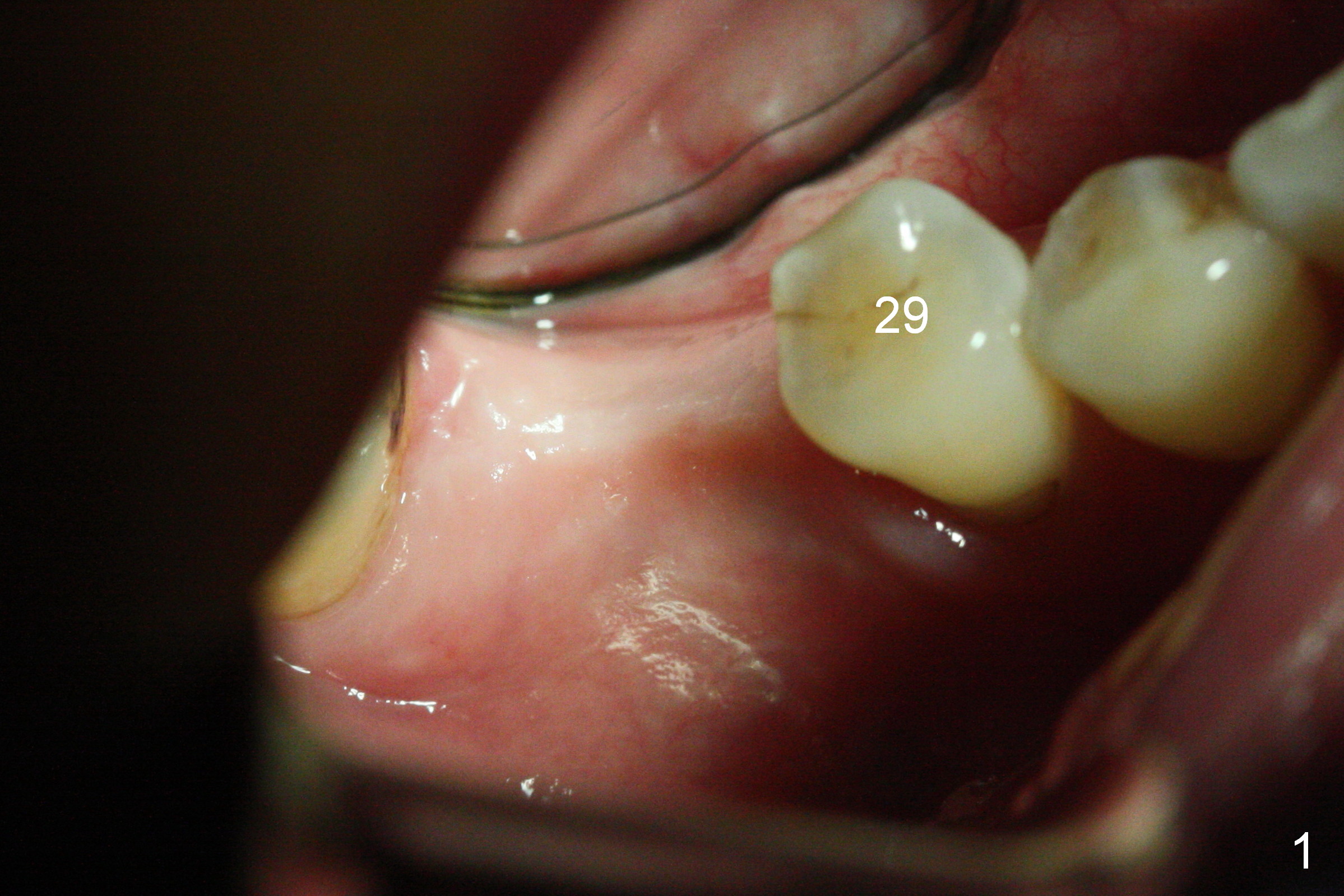
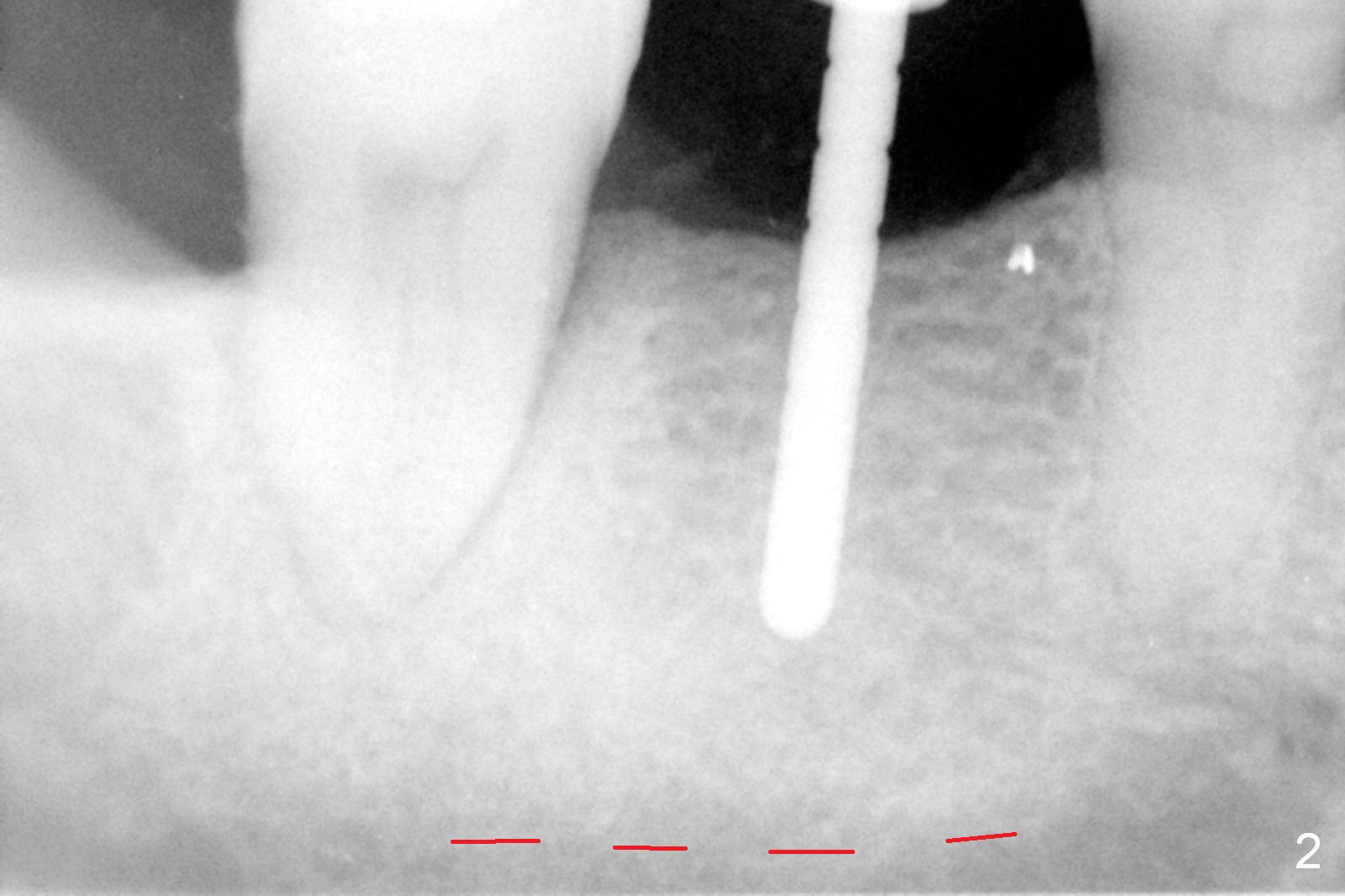
The ridge appears narrow buccolingually at the site of #30 of the dentophobic patient (Fig.1). The ridge does not look narrow after raising flaps. The initial osteotomy depth is 10 mm with ~4.75 mm clearance from the superior border of the Inferior Alveolar Canal (Fig.2 red dashed line). The depth is increased to 11.5 mm until a drill with diameter of 3.7 mm and 12 mm with 3.2 mm. The insertion torque of a 4.5x11.5 mm implant is ~ 55 Ncm (Fig.3). There is minimal implant exposure buccally and lingually, which is covered first with harvested autogenous bone, following placement of 6.5x4(2) mm abutment. The graft is washed out by the copious saliva, which is due to lack of pain control while suture is being placed. Later allograft is applied.
A new method is proposed for secure placement of bone graft. After implant placement is confirmed, block anesthesia is administered for pain control. Mix autogenous bone (fine in size, wet with blood) with a small amount of allograft (coarse in size, dry). Insert a piece of folded dry 2x2 gauze in the lingual vestibule in the same way using cotton roll for a mandibular implant case if block anesthesia is not given.
If bone loss turns out to be severe later, it is due to the shallow placement of the implant.
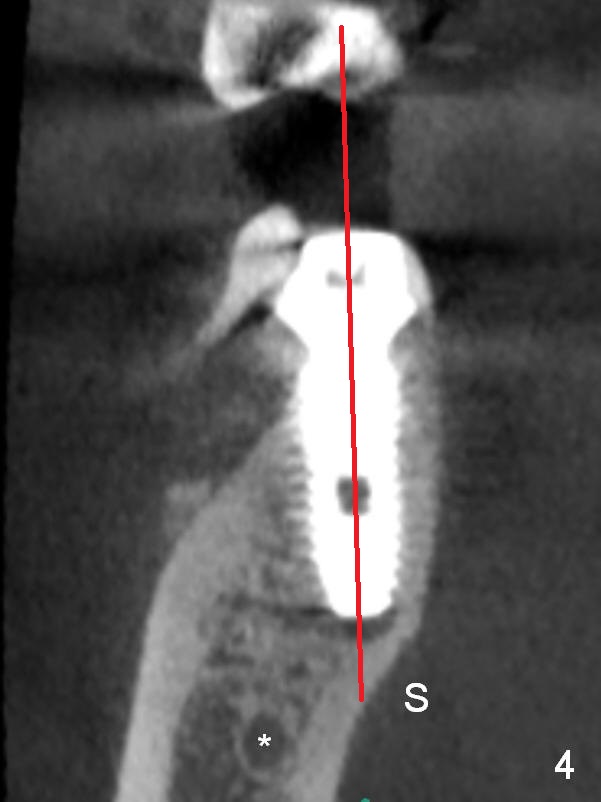
The nervous patient seems to have longer period of time of postop pain, although there is no paresthesia. To rule out any complication, CBCT is taken 4 days postop. The latter demonstrates a good trajectory (Fig.4 red line), but the lingual plate nearly perforates at the Submandibular Fossa (S, (*: Inferior Alveolar Canal)). The latter has rich blood supply and loose tissue with difficulty in hemostasis. Therefore the implant should be short when the ridge is narrow to avoid inadvertent perforation into the Submandibular Fossa.
A provisional is fabricated after abutment reprep 1 month postop.
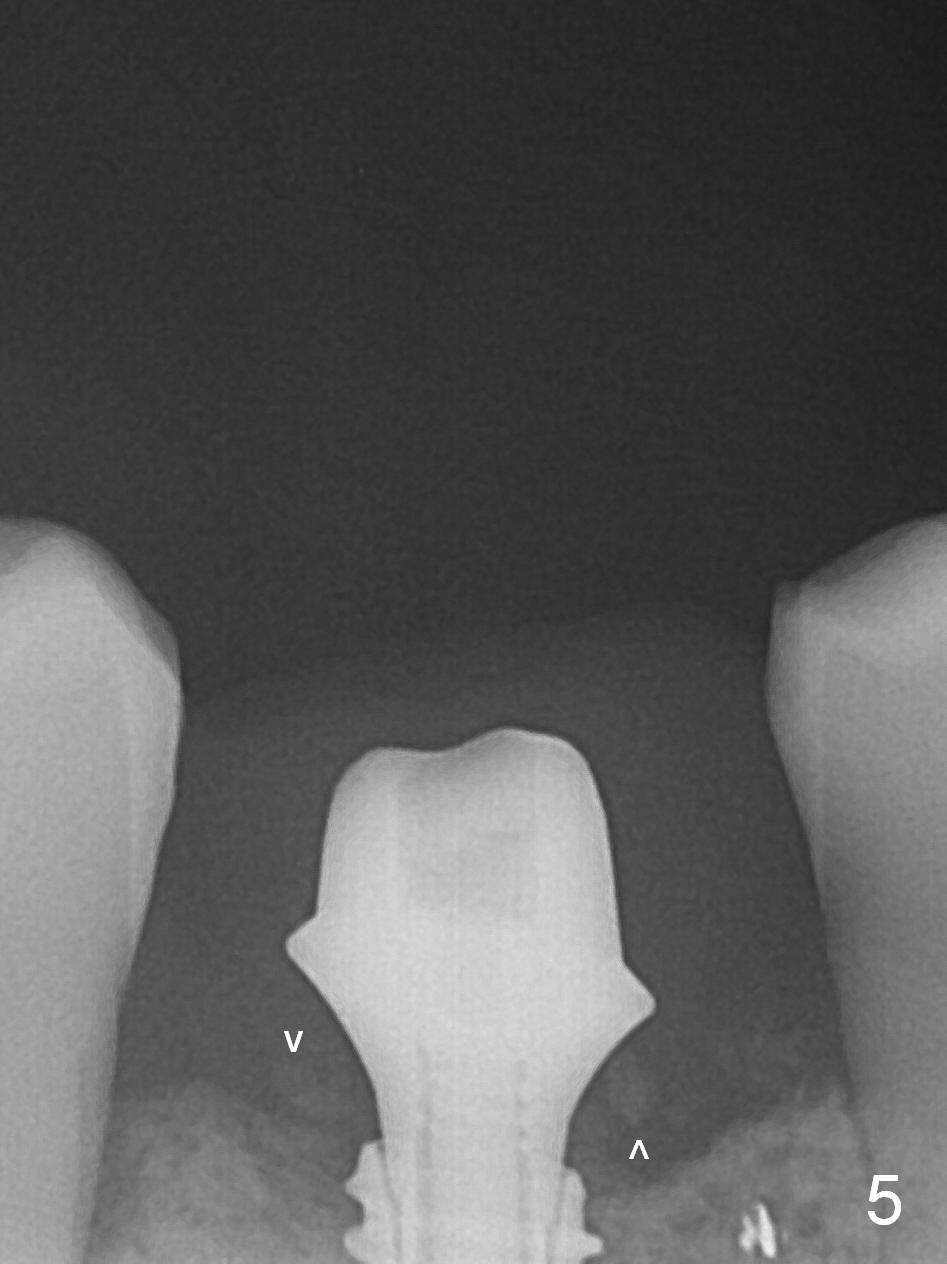
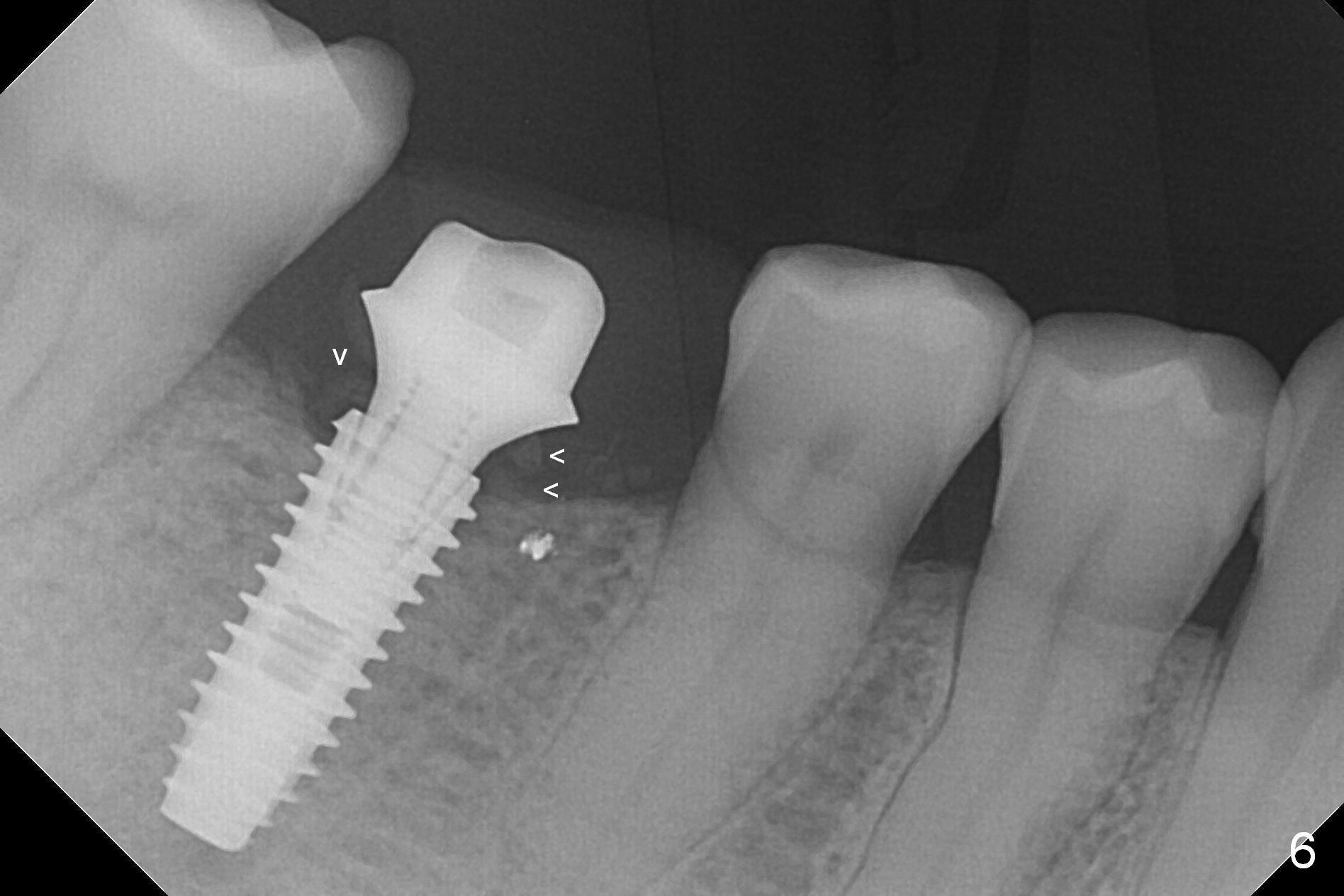
The patient returns for impression for final restoration 3 months 10 days postop. PA shows mild crestal bone resorption with retention of the bone graft (Fig.5,6 arrowheads). The ridge looks wider with implant and abutment in place (Fig.7) than before (Fig.1).
Return to Lower Molar Immediate Implant, IBS
Xin Wei, DDS, PhD, MS 1st edition 10/21/2016, last revision 01/31/2017