






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Closure of Molar Socket Following Immediate Implant: Suturing
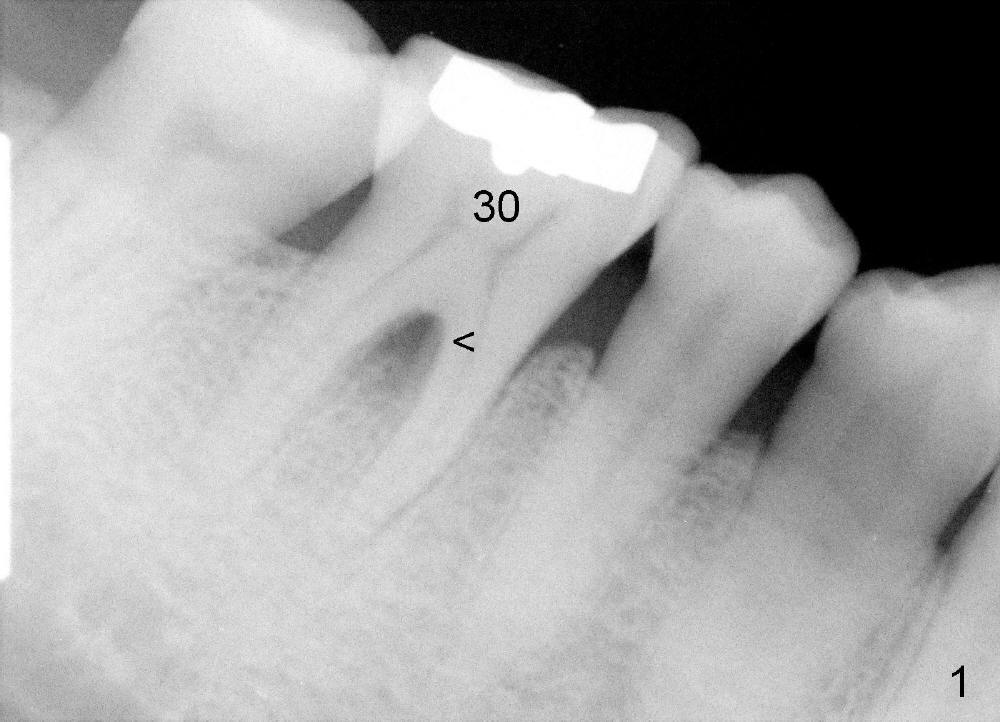
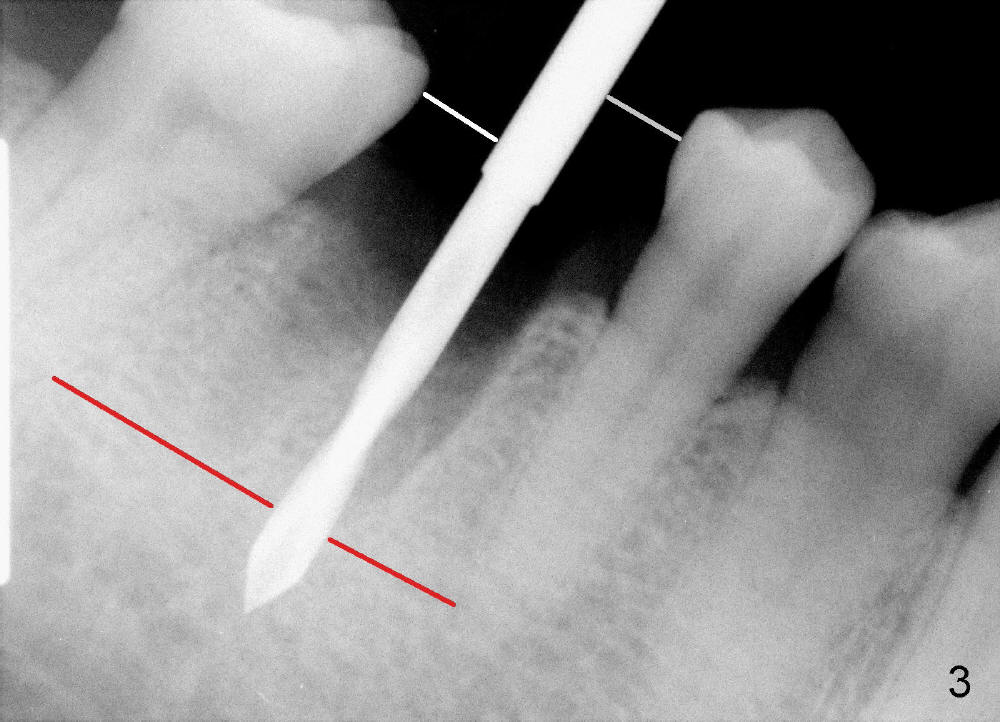
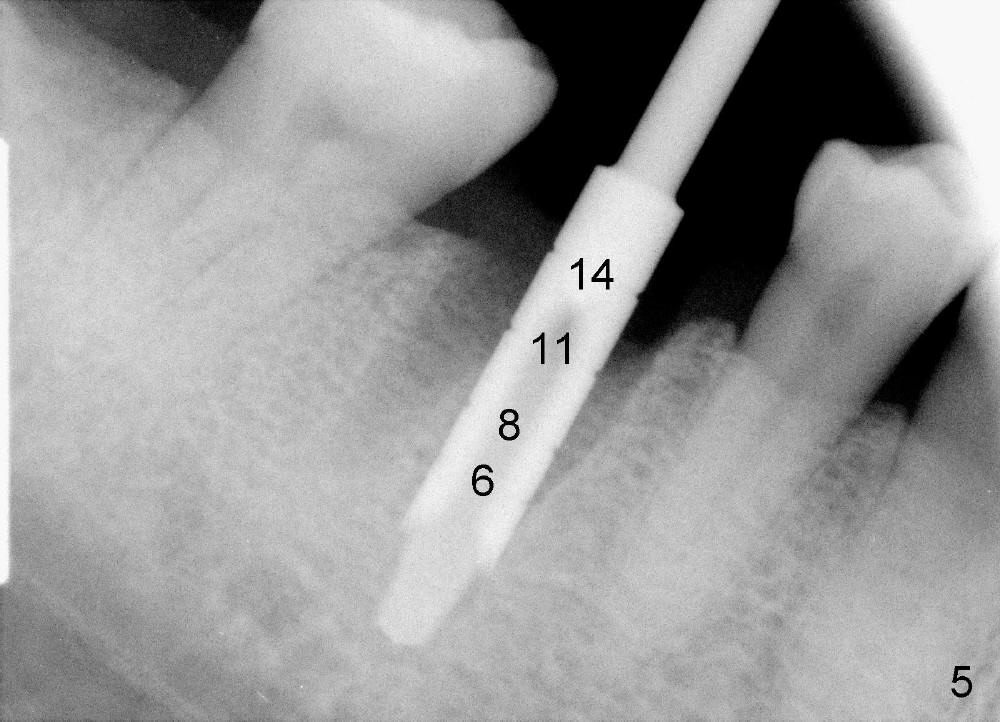
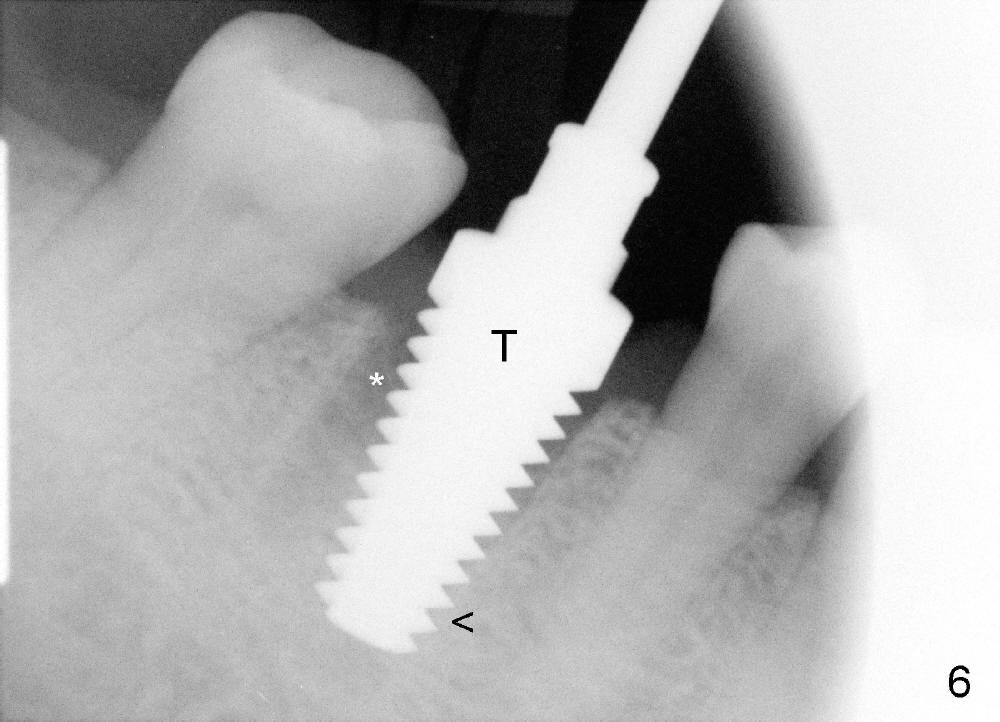
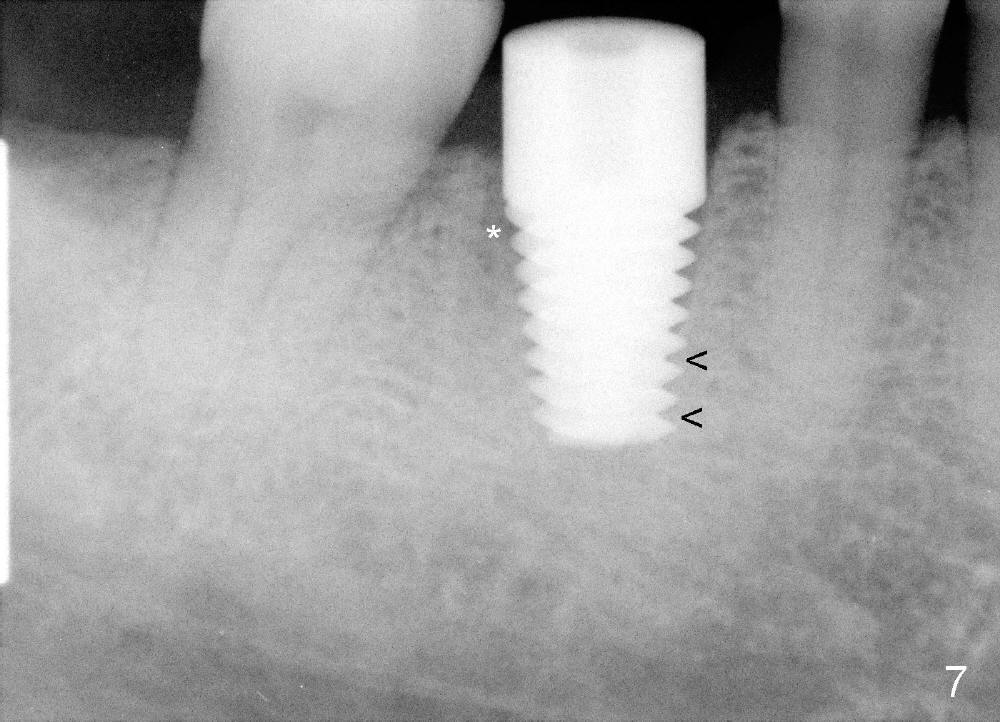
A 47-year-old man has had perio infection in the lower right 1st molar twice (Fig.1,2). Buccal and lingual furca pockets are ~ 9 mm. Following extraction and sectioning the septum, the osteotomy is initiated with a 2 mm pilot drill (Fig.3). Although the drill deviates into the mesial socket, the coronal end is controlled more or less in the middle of the edentulous area (compare white and red lines). Ideally the axis of the osteotomy (Fig.4 red line) should be parallel to that of the 2nd molar and perpendicular to the curve of Spree. The coronal end of the 3.5 mm reamer (Fig.5) and of the 7x17 mm tap (Fig.6 T) remains in the center of the edentulous space. The apical threads of the tap are engaged into the bone for stability (Fig.6 <). When 7x17 mm implant is placed with > 60 Ncm, the mesial socket is obliterated while the density of the distal one increases because of autogenous bone grafting (Fig.7*).
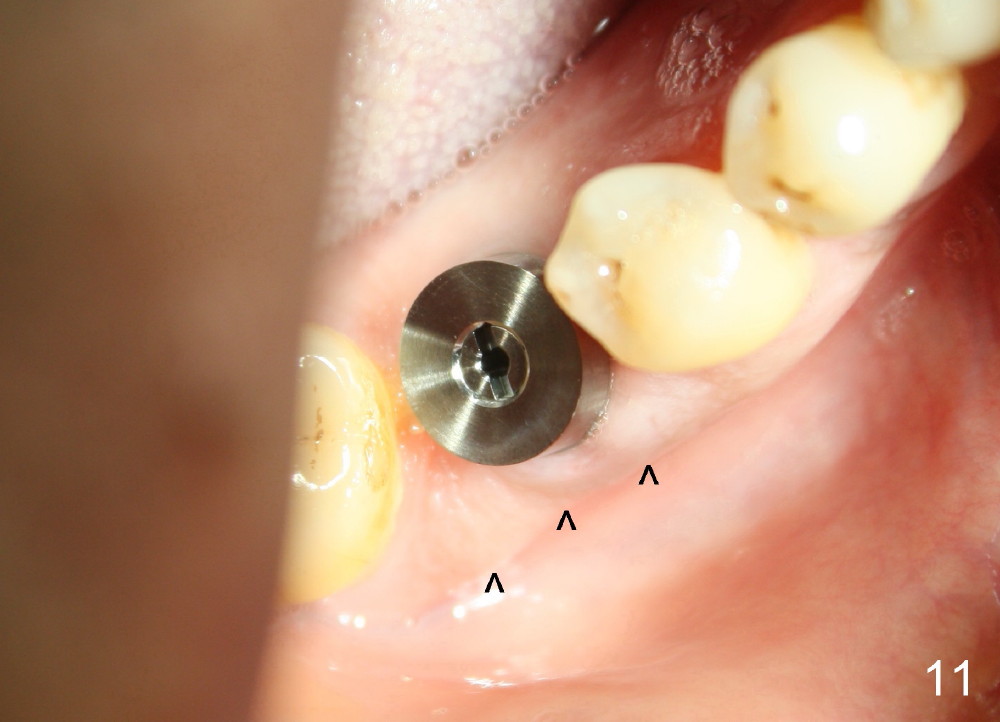
The distal socket is closed completely with suture, whereas the mesiobuccal space is partially closed with collagen gauze and suture (Fig.8 *). The wound is then covered by perio dressing. The gingiva heals around the implant 18 days postop (Fig.9). Three months postop, the implant is stable. The mesial upper portion of the threads appears to have better contact with the bone (Fig.10 <, as compared to Fig.7); the density of the distal socket seems to increase (*). There is no buccal plate atrophy (Fig.11 ^). Supragingival margin is designed for the crown to prevent periimplantitis (Fig.12)
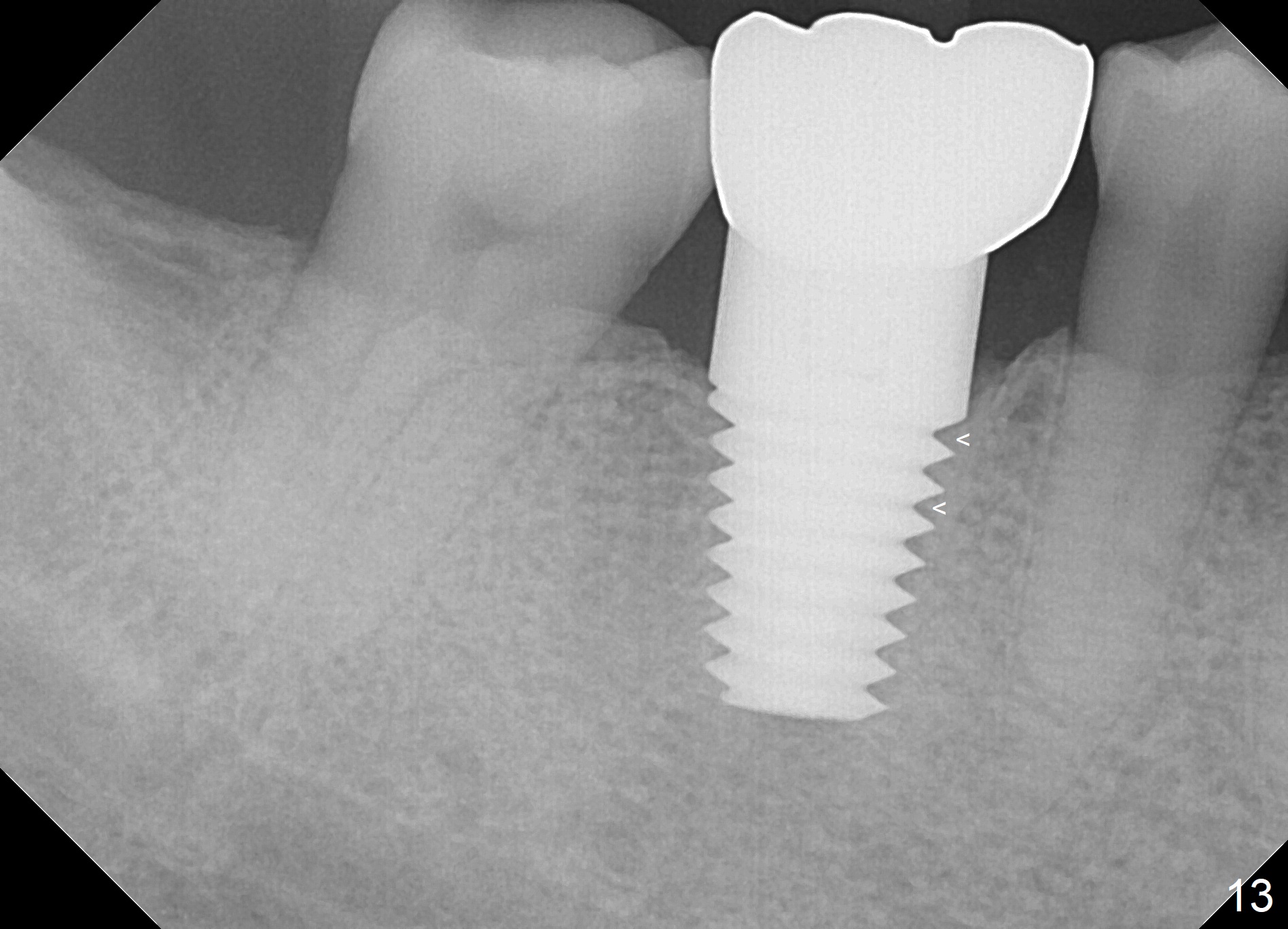
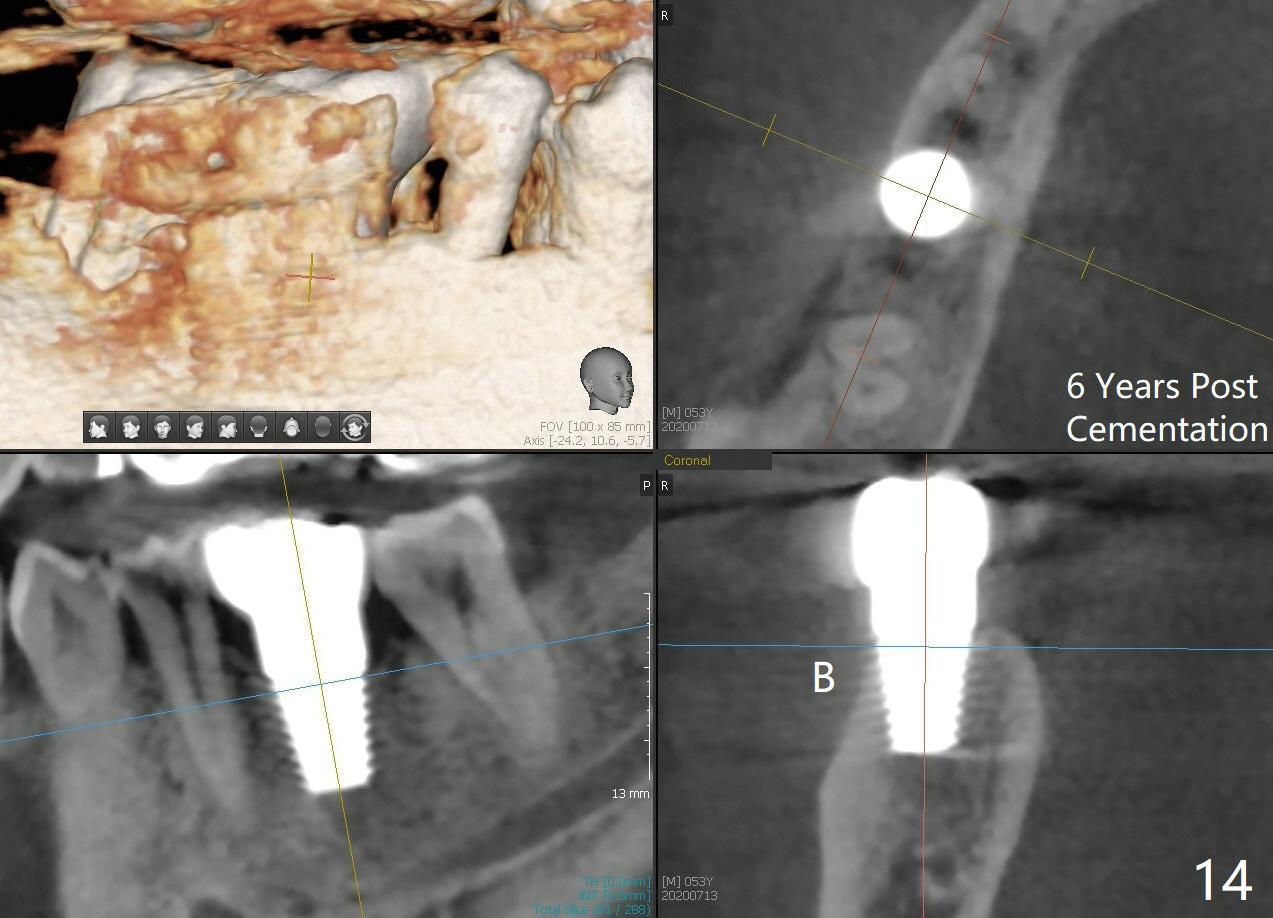
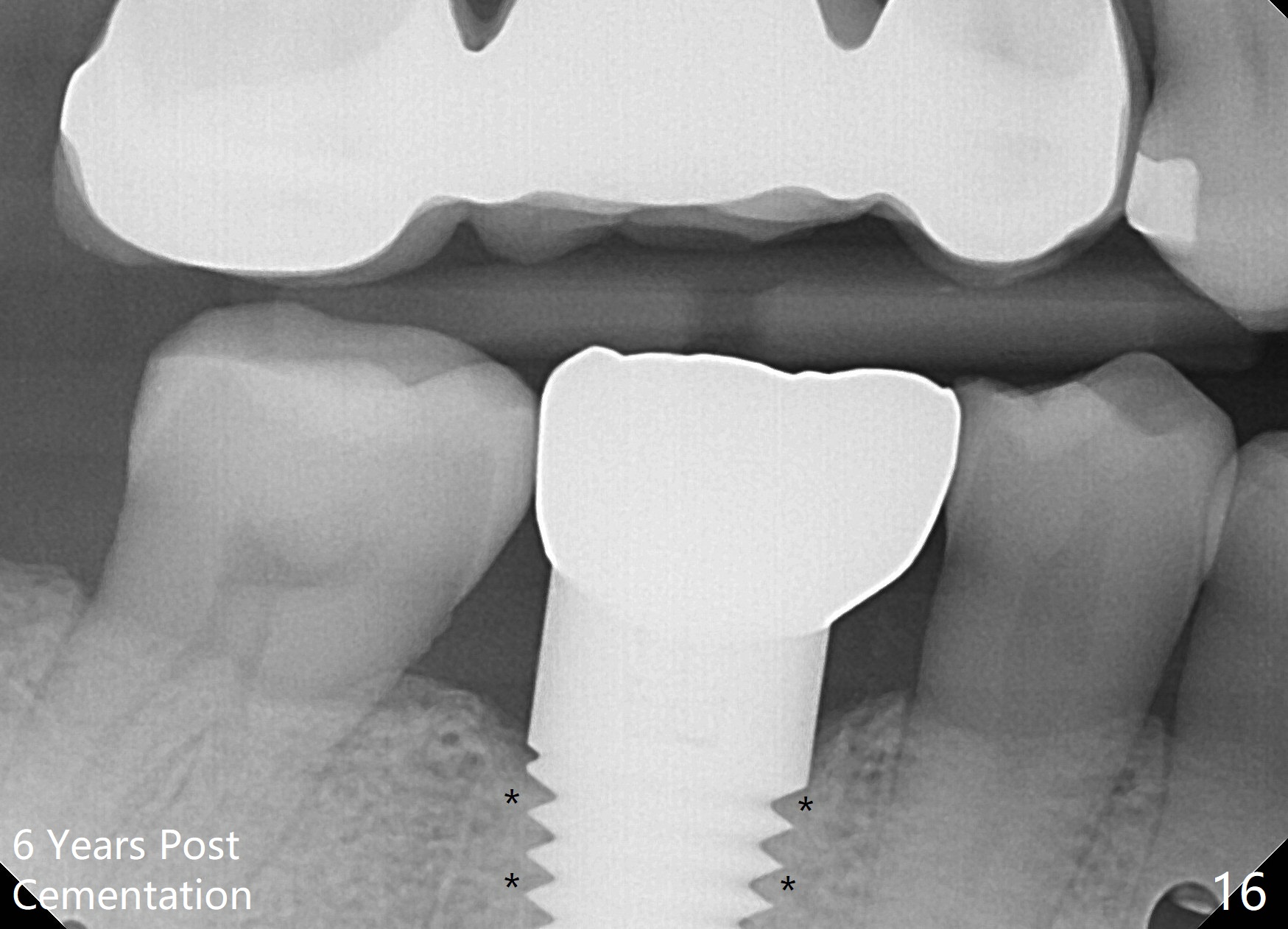
When a large implant is placed in a molar socket, one dimension of the remaining socket is small (buccolingual for lower, mesiodistal for upper). It is apparent that the mandibular buccal and lingual gingiva is relatively loose for the most time, the mesial and distal socket could be closed by suturing and perio dressing. The maxillary palatal gingiva is particularly thick and tough to be approximated. It appears necessary to develop a technique using an immediate provisional to close the socket or place an abutment. Cortex-like bone seems to have grown into the mesial thread spaces 3 years post cementation (Fig.13 <). The 7x17 mm implant was placed buccal (Fig.14 B). The slowly resorbed buccal plate seems to darken the buccal gingiva (Fig.15 B). The bone next to the implant is dense 6 years post cementation (Fig.16 *). The implant at 19 should be smaller and placed lingual.
Return to Lower Molar Immediate Implant 13
Xin Wei, DDS, PhD, MS 1st edition 03/09/2014, last revision 11/25/2020