

|
|
|
|
|
|
|
|
|
|
Immediate Implant Threads Should be Contacted by Bone, Native or Grafted
Common denominators of peri-implantitis associated with immediate placement are no or not enough bone graft and lack of infection control (patients do not take antibiotic and lack oral hygiene, as instructed).
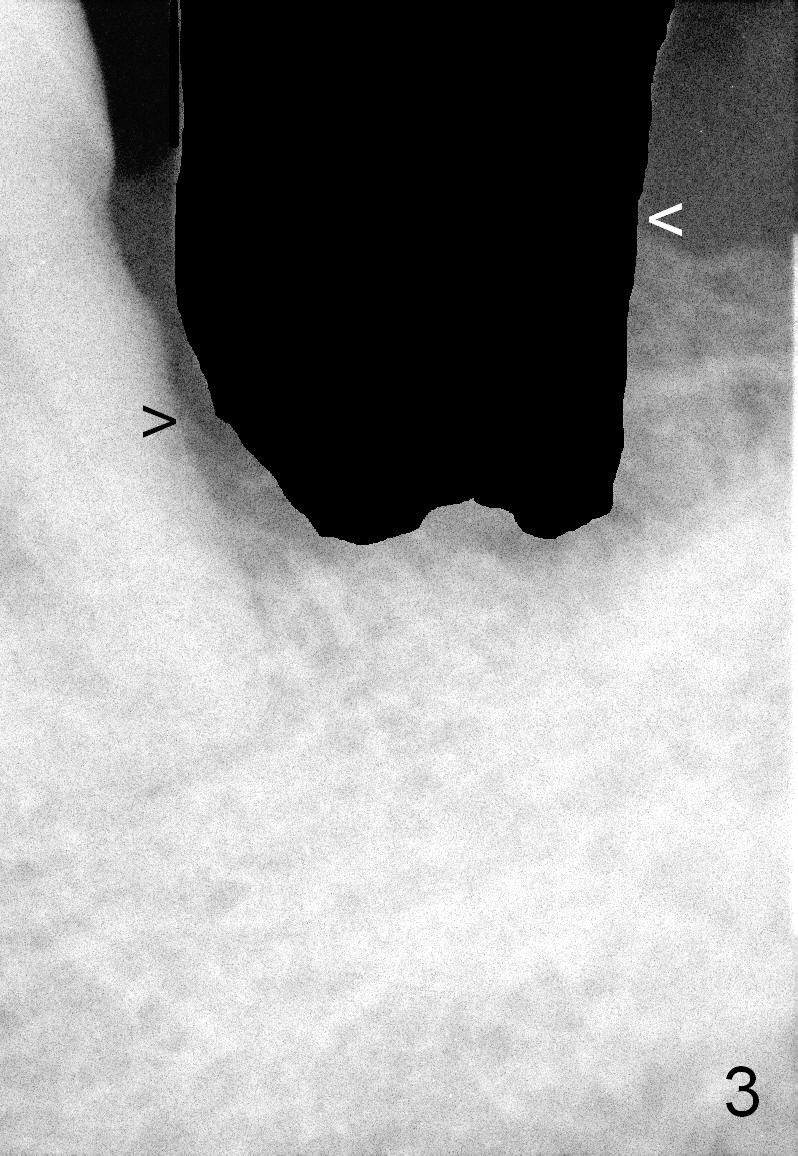
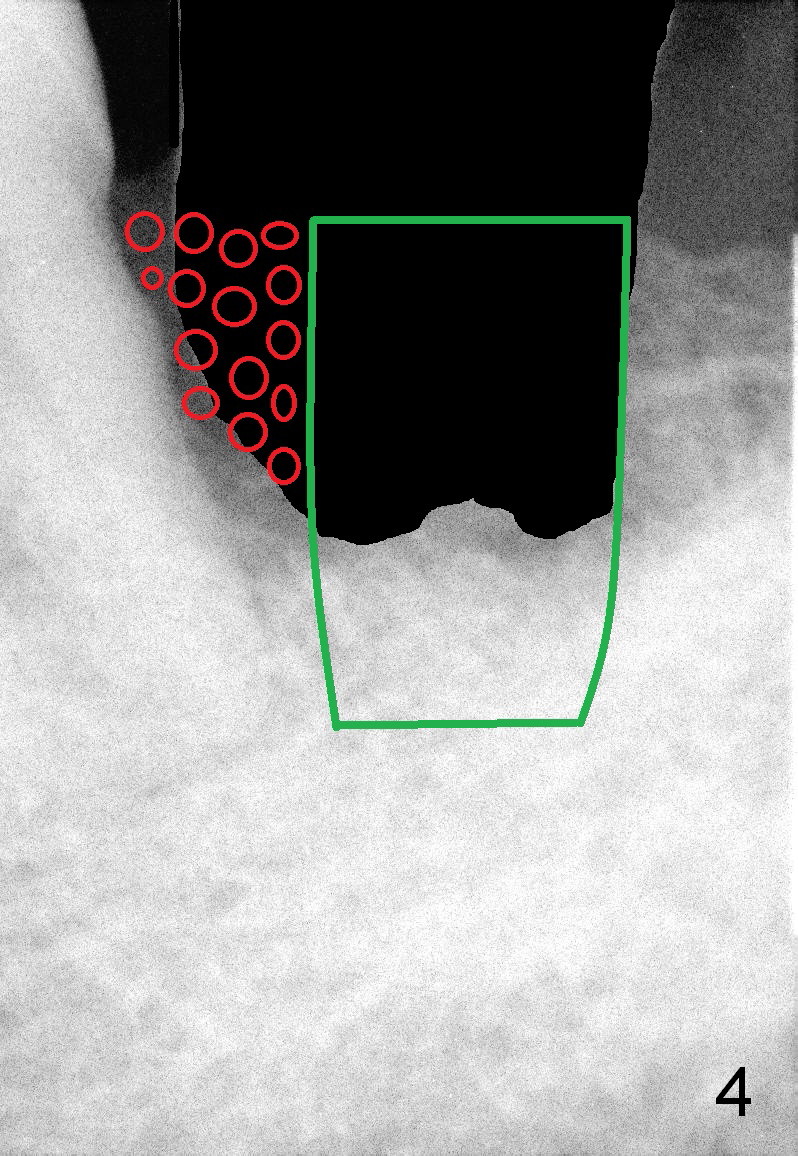
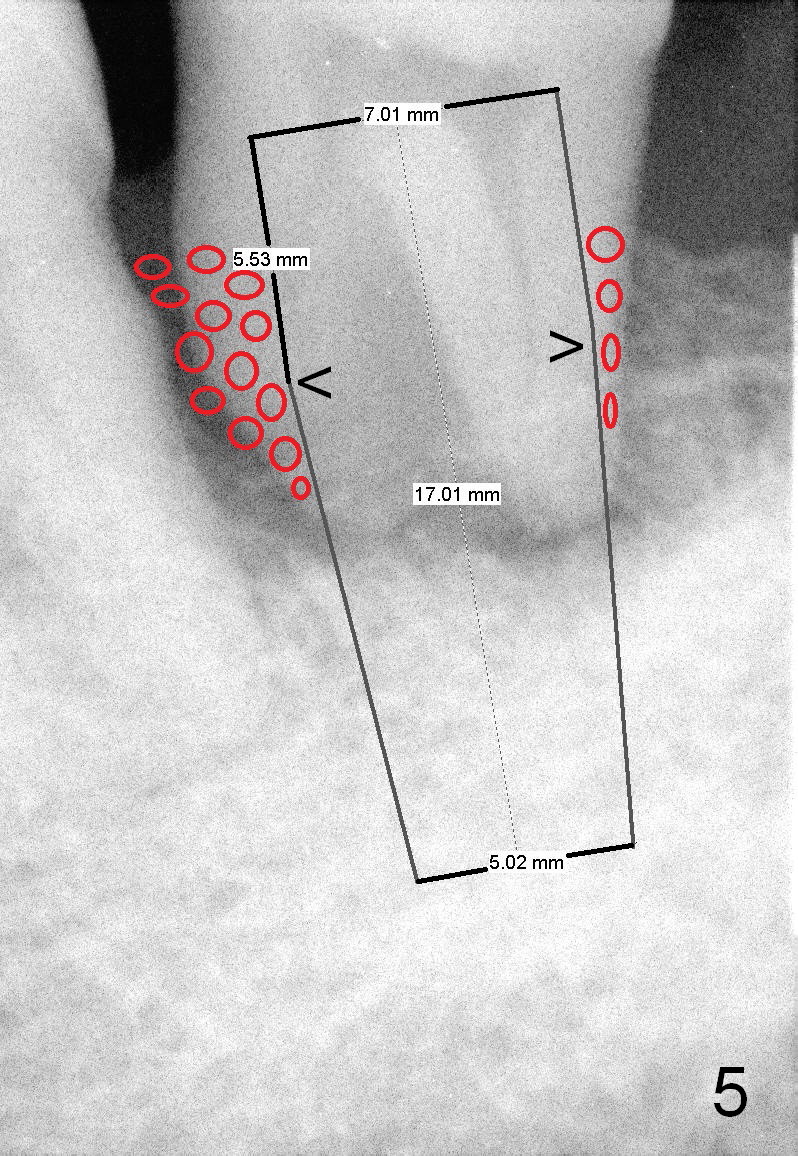
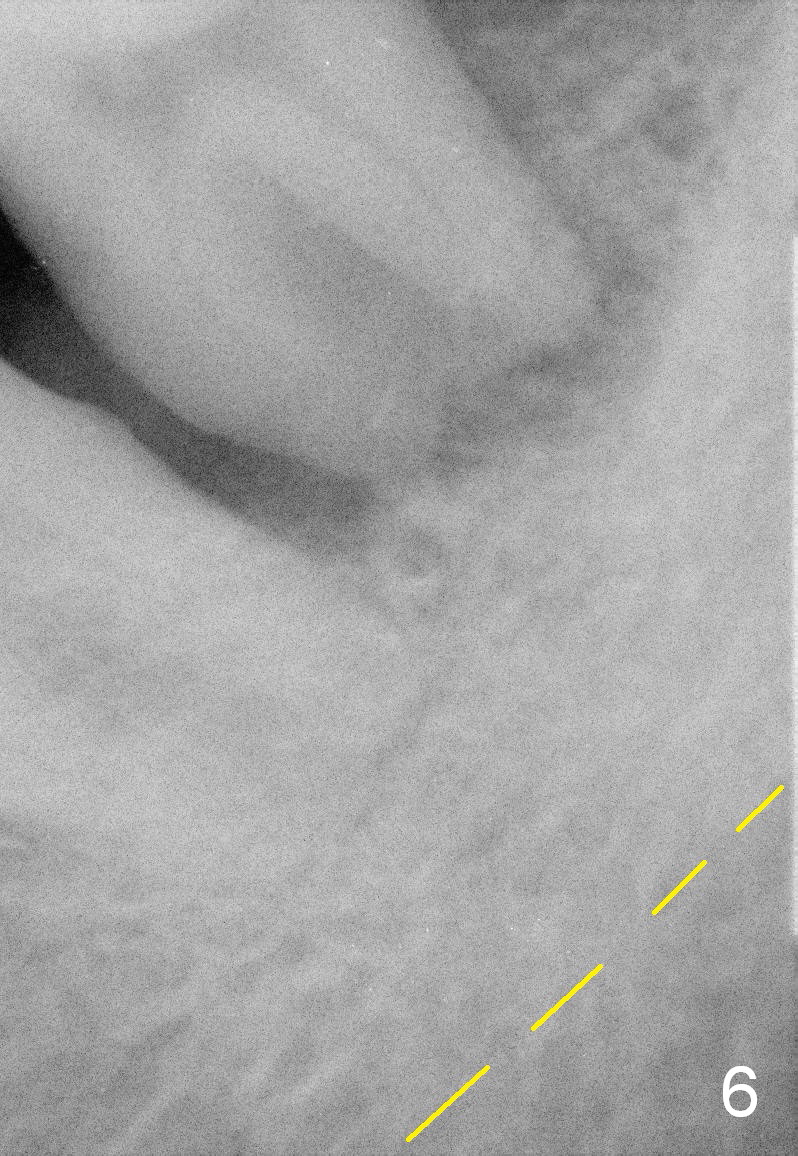
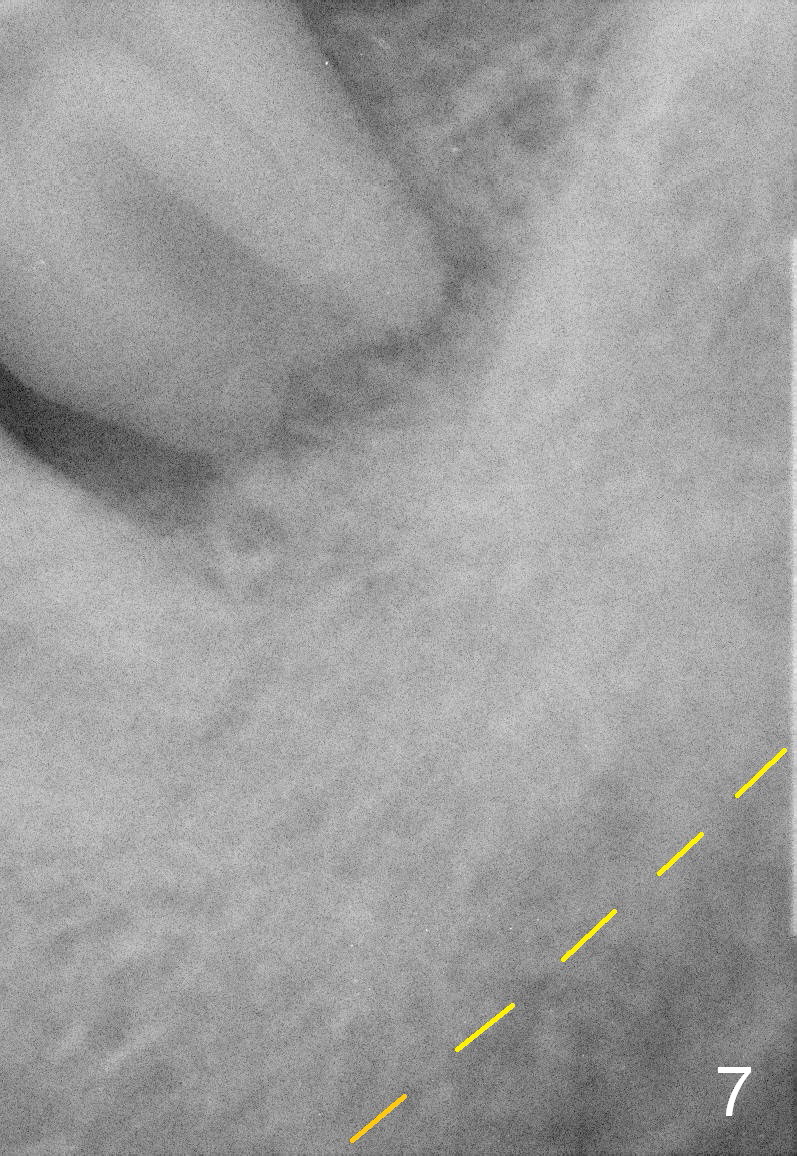
A 63-year-old man has periodontitis. The tooth #18 (probably 17) has mobility III (Fig.1). Three more PAs are taken with deeper placement of #2 sensor (Fig.2,6,7) to show the upper border of the Inferior Alveolar Canal (yellow dashed lines). The affected tooth has severe bone loss, especially mesially (Fig.2,3 (arrowheads)). No matter whether bone (Fig.4) or gingiva (Fig.5)-level implant is placed, the threads should be covered circumferentially by bone, native or grafted (red circles). In Fig.5, the threads are apical to black arrowheads, whereas the rough surface, which should be also contacted by bone, is the lower half above the black arrowheads.
Measures of infection control include pre- and post-op oral antibiotic and Chlorhexidine mouth rinse. Intra-op measures consist of sterile surgical field, intra- and extra-oral sterilization, removal of granulation tissue, application of antibiotic to the socket and copious irrigation. The distal root surface of #19 may have calculus and plaque (Fig.1 *). Scaling & root planing is to be done, followed by application of Emdogain and placement of bone graft.
Return to Lower Molar Immediate Implant
3,12,14,15,
30
Xin Wei, DDS, PhD, MS 1st edition 03/08/2015, last revision 02/16/2018