|
|
|
|
|
|
What is Your Treatment Option?
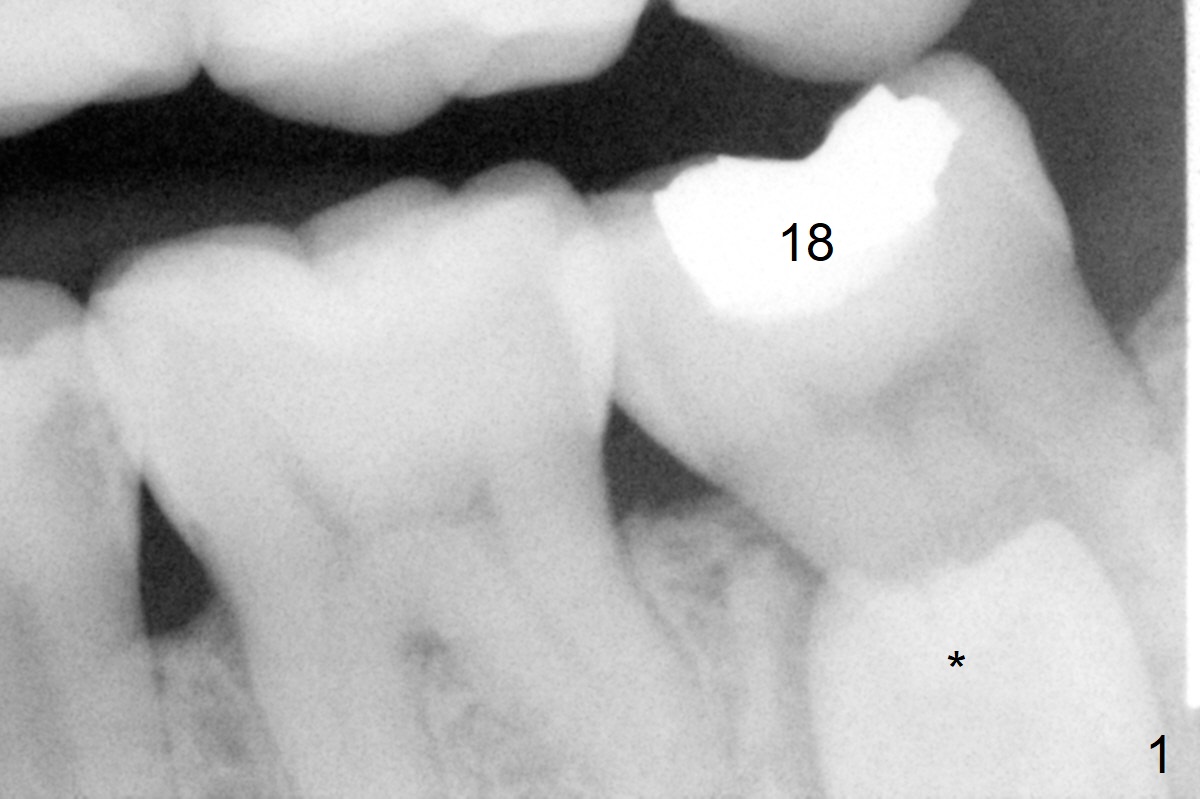
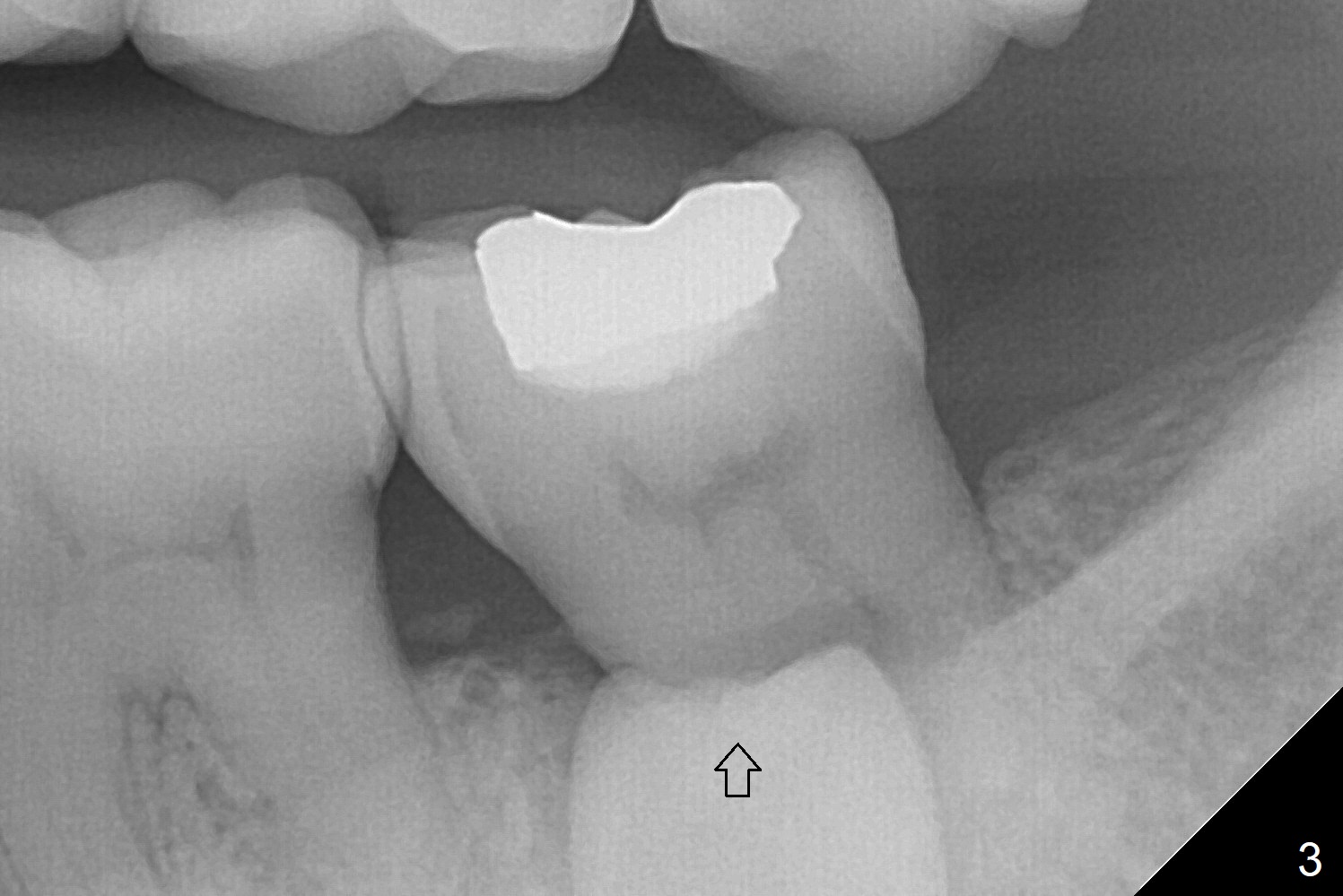
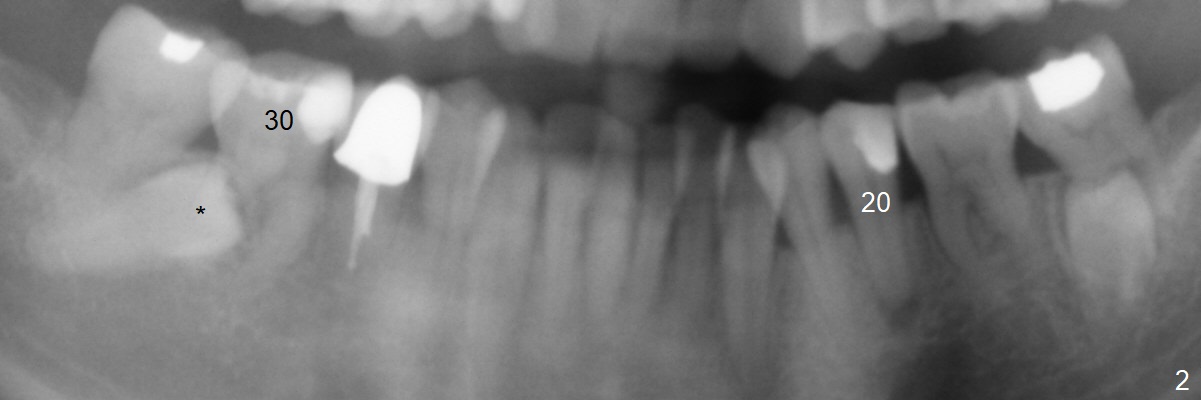
A 45-year-old woman with severe crowding (Fig.2) presented to my office 9 years ago; the tooth #18 appears to have root resorption, most likely due to a supernumerary tooth (Fig.1 *). The latter seems to be erupting in 6 and 9 years (Fig.2,3), probably because of immature apex (Fig.2, as compared to the supernumerary tooth in the lower right (*)). Recently the patient has transient sensitivity at #18. The tooth has mobility I without deep periodontal pockets. If the tooth #18 turns to be non-salvageable, what should be done? The tooth #20 has received root canal therapy, while the tooth #29 has had RCT retreat.
Dr. Ness: What is your question? It is obvious to remove 18 and the
supernumerary tooth, and place an implant. Anything else? Wednesday,
August 30, 2017 10:28 PM
Reply: Thanks. Since the supernumerary tooth seems to have open apex with
potential to erupt, the maxillary molars will be used anchorage after initiation
of ortho (for crowding). With lingual button(s) to be placed on the
supernumerary tooth while the tooth #18 is extracted and elastics between the
upper molars and lingual buttons, the extra tooth may be able to erupt into the
site of #18. If not, extraction and implant. Ortho may involve extraction U4s
and L5s.
Dr. Ness: The supernumerary tooth does not have the root surface area to act as a molar. Not sure that is the best option. Takes too long for an exercise to see if you can do it, not that you should do it. If you do succeed, what do you have? No occlusion unless you make a crown. Likely you'll have a mobile tooth in the end. Wednesday, August 30, 2017 11:42 PM
Good point. So far this has been mental exercise. The patient is conservative and most likely will not let me touch the case.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS,
Antibiotic
Xin Wei, DDS, PhD, MS 1st edition 08/30/2017, last revision 08/31/2017