
|
|
|
|
|
|
|
|
|
|
Place Immediate Implant Deeper at Lower 2nd Molar
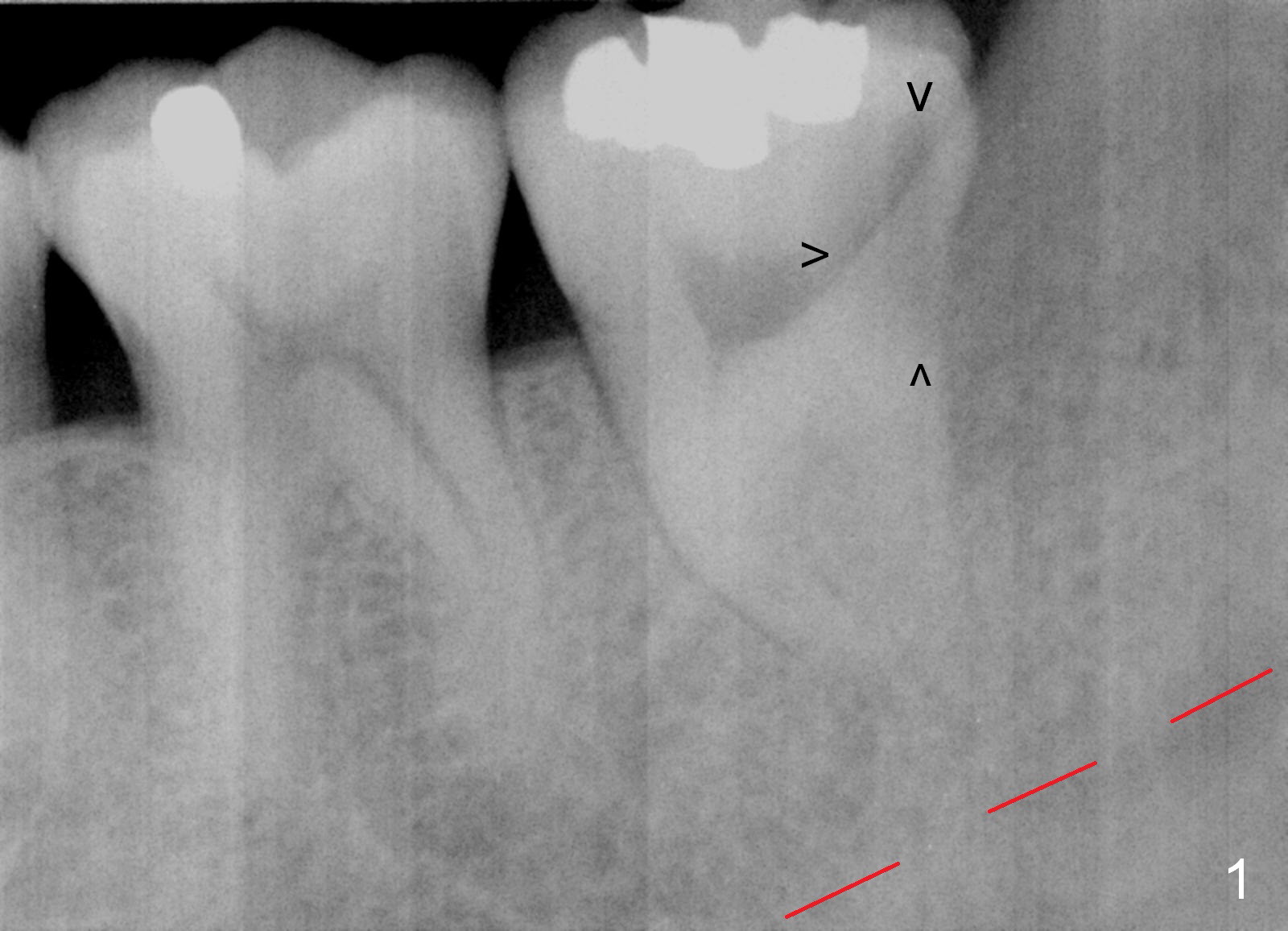
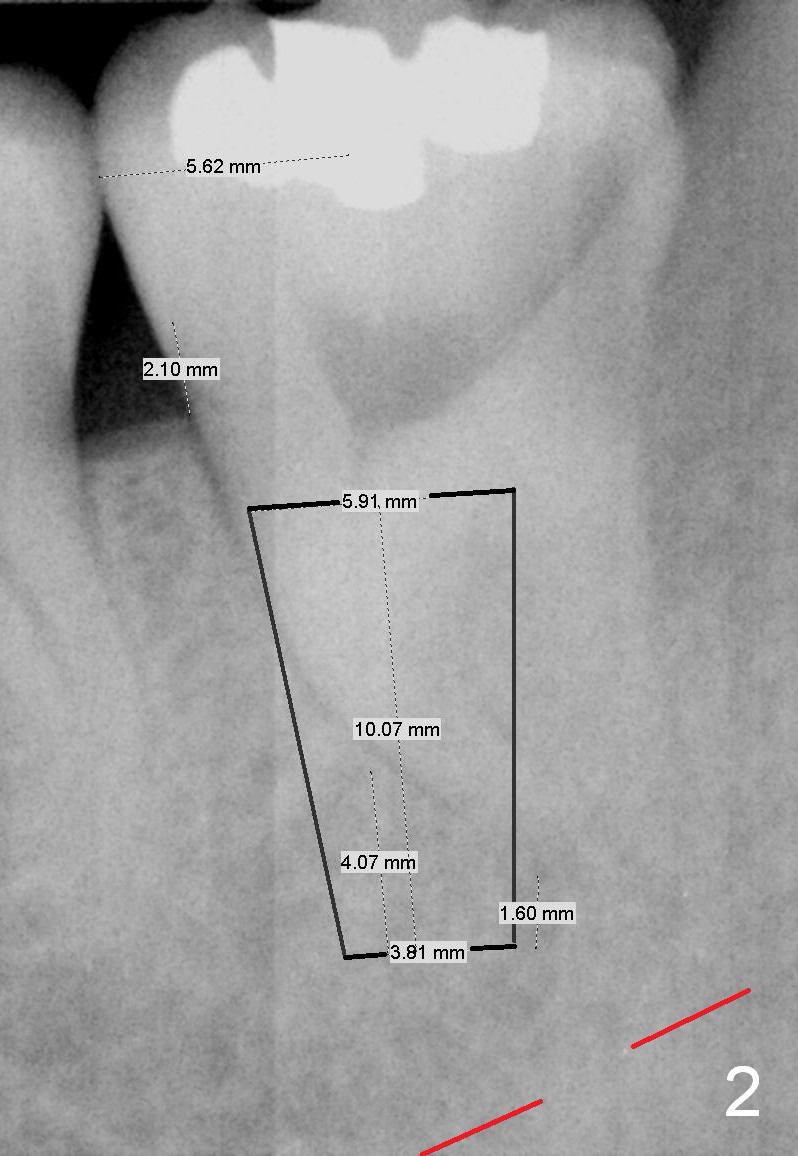
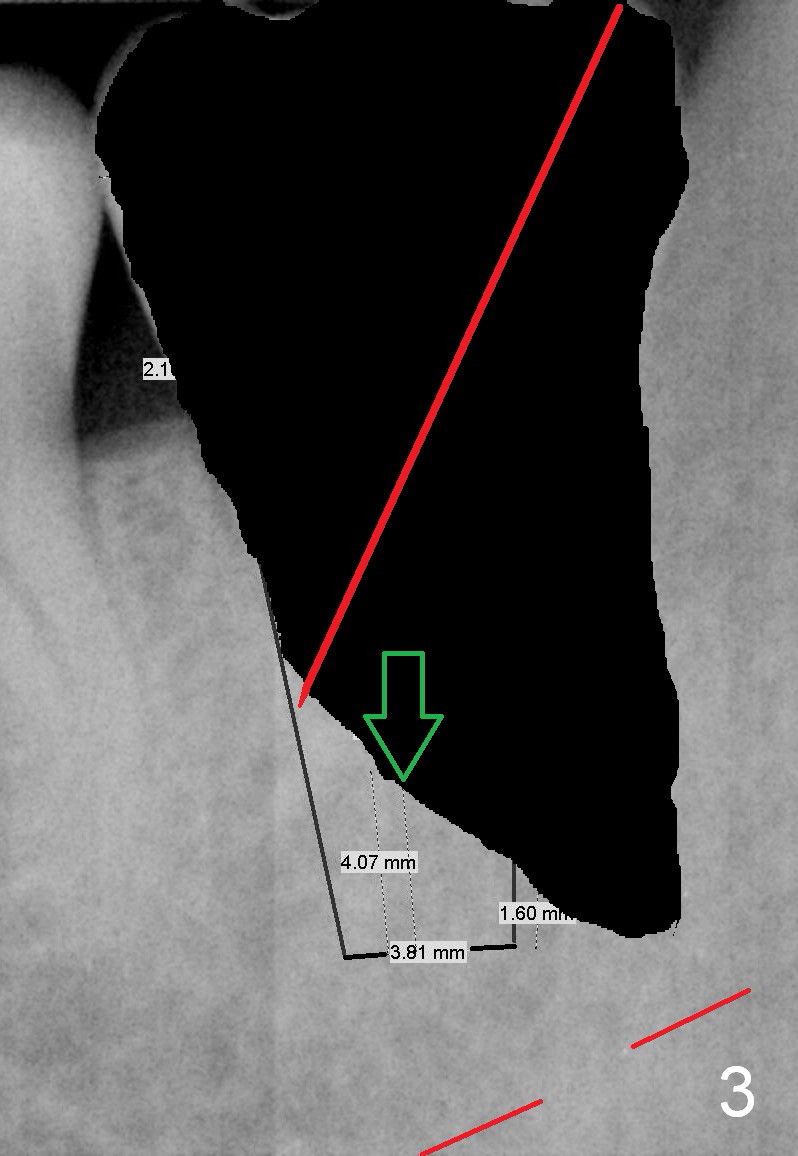
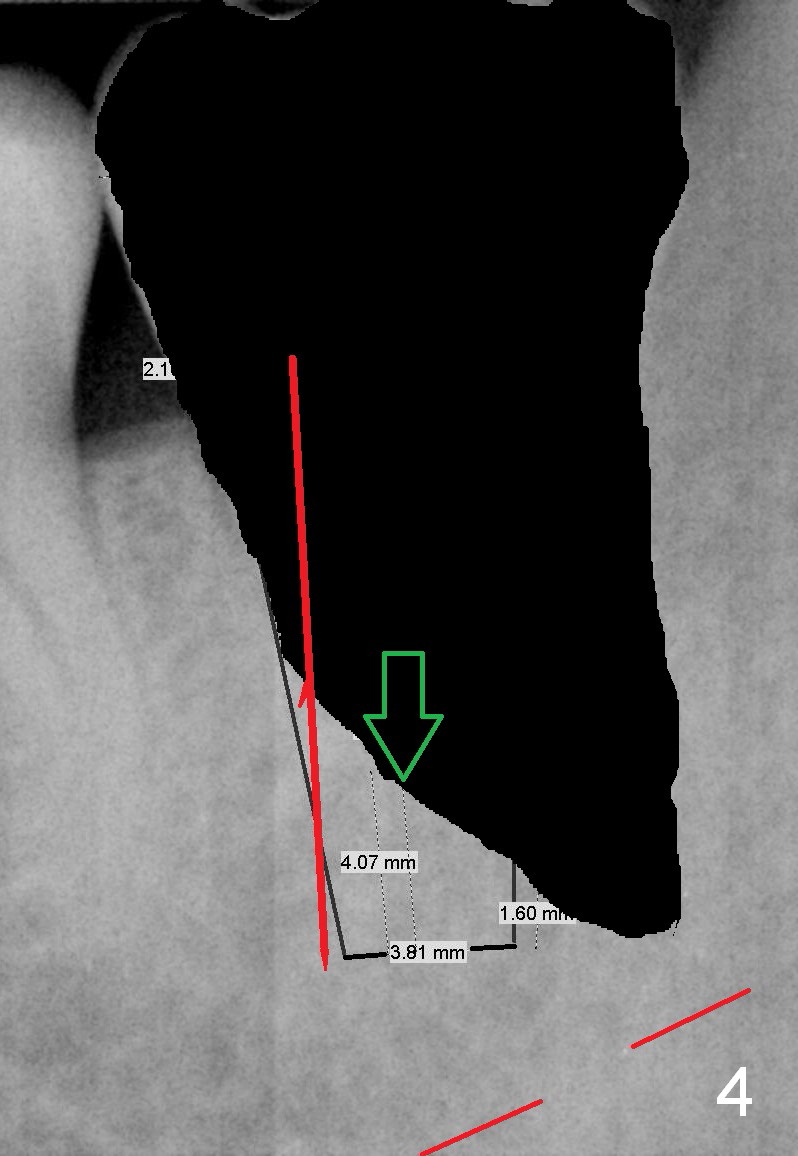
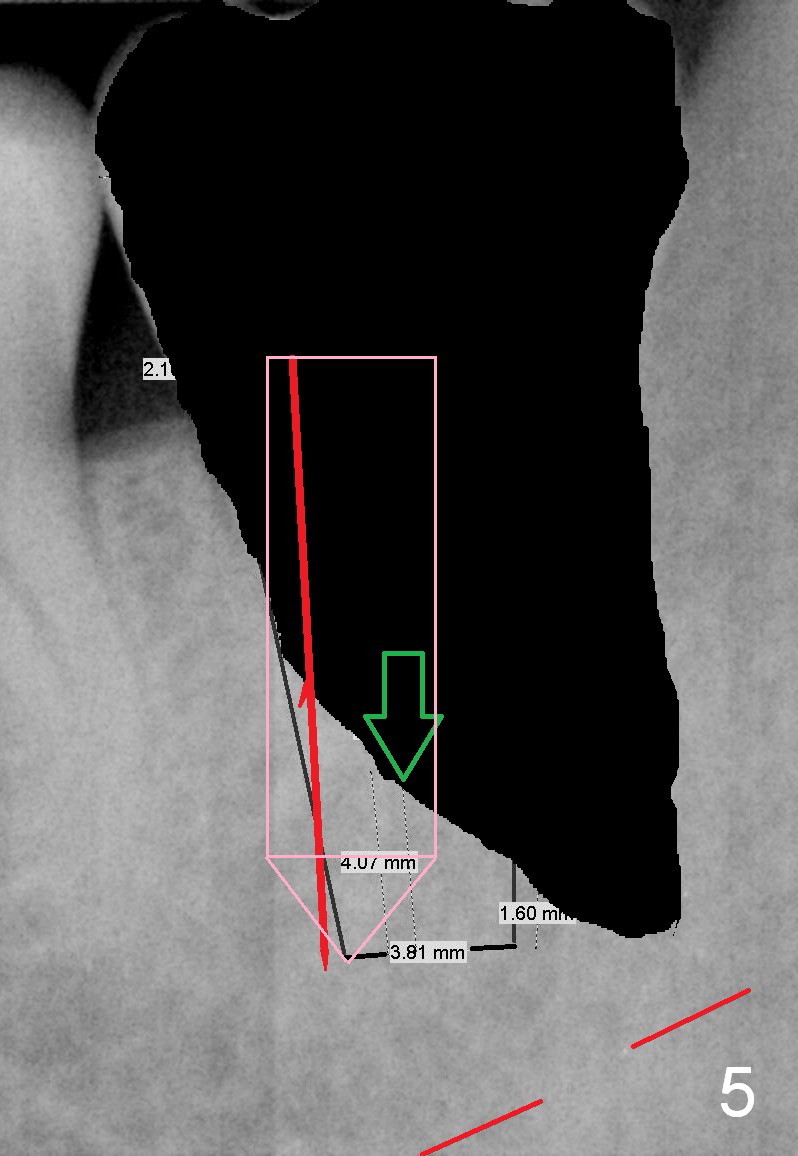
A 34-year-old man has distal deep caries of the lower 2nd molars. Root canal therapy turns out to be difficult on the right side due to bleach leakage. It would be also difficult to restore the distal defect. Finally he agrees to have extraction and implant. The result is good. He is ready to accept the same treatment for the left 2nd molar (Fig.1 (arrowheads: caries)). Metronidazole will be used for socket decontamination. Place a 5.9x10 mm bone-level implant 2 mm below the mesial crest (hopefully at the same level of the buccal crest) so that there is enough height to place an abutment (Fig.2). The apex of the implant is placed mesial to that of the root, since there is more bone, away from the superior border of the Inferior Alveolar Canal (red dashed line). The osteotomy is to be initiated in the middle of the mesial slope obliquely, more mesial (Fig.3 red line) than the center of the implant (green arrow). Once the lamina dura is penetrated, change the trajectory along the future long axis of the implant (Fig.4 red line). The depth will be 14 mm from the mesial gingival line (Fig.2). As the diameter of drills increases, the osteotomy tends to shift distal (Fig.5 pink arrow).
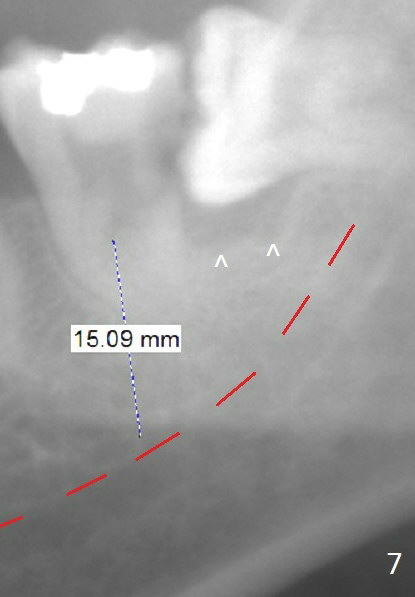
In fact, RCT is tried. Fourteen months later, the tooth remains symptomatic with mobility (Fig.6). Due to the distal defect caused by the 3rd molar (Fig.6,7 arrowheads), the implant should be placed as mesial and deep as possible.
Return to Lower Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
IBS
Xin Wei, DDS, PhD, MS 1st edition 01/21/2016, last revision 04/13/2017