
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bone Expansion for Healed Socket
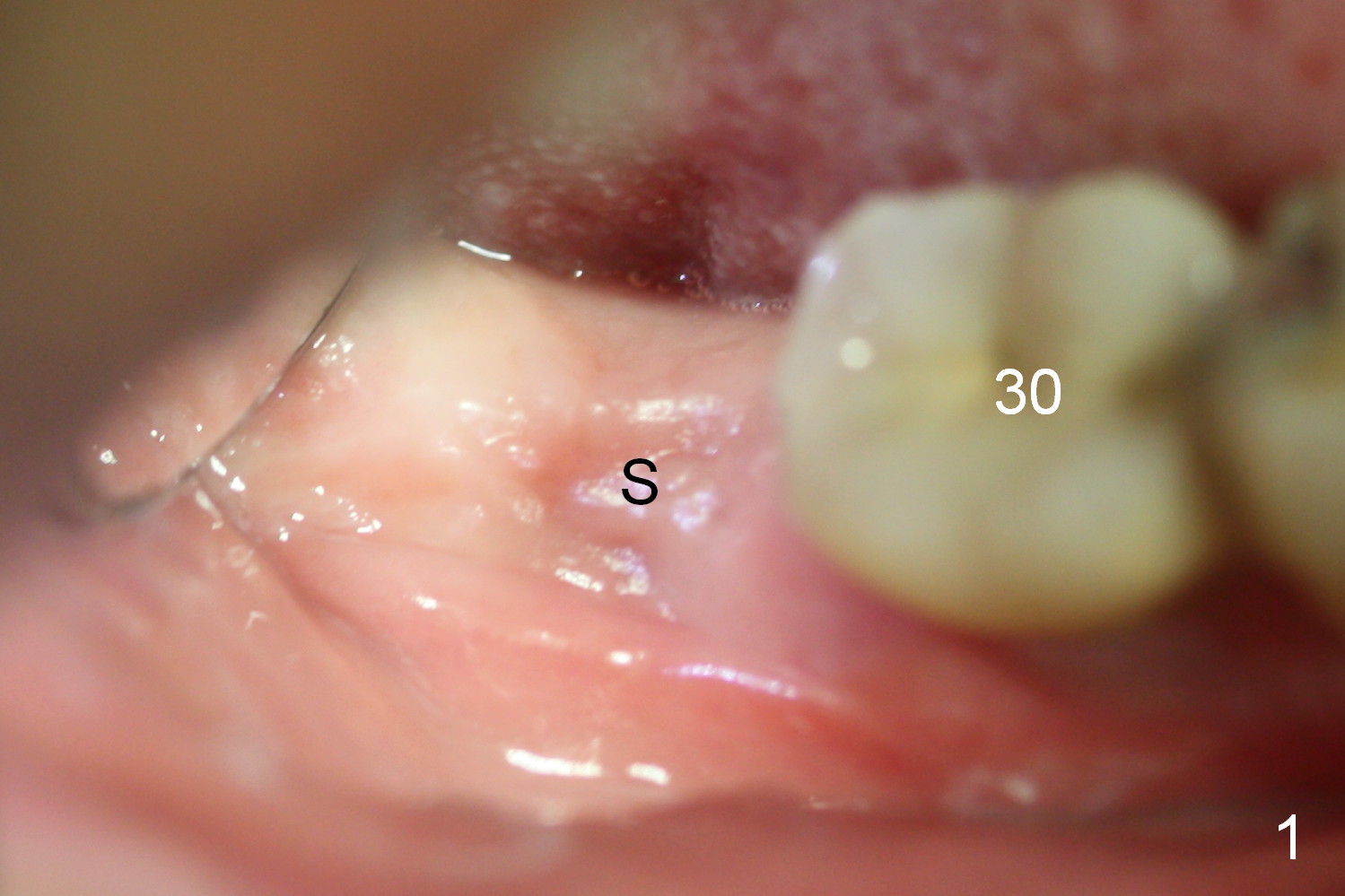
A 75-year-old man has apparent history of bruxism. The distal root of the tooth #31 had vertical fracture after root canal therapy. The tooth was extracted ~ 2 months ago while he returned to home country. It appears that there is buccal plate atrophy (Fig.1 S: socket).
Incision will be made to determine pattern of bone resorption and where to initiate osteotomy. Although the soft tissue of the socket (Fig.1 S) has healed, the bone must be still healing (soft, Fig.2 radiolucent socket). Use DIO starter drill, 2 mm pilot drill set at 12 mm (4 mm implant spacer) and short and marked parallel pins. Keep the last pin in place and take PA and photos. Change trajectory with Lindamann bur in the cassette if needed. Then start using bone expanders as large and deep as possible. The bone beyond the socket may be not as soft. Keep the largest expander in place and take photos. We want to confirm that not only is the buccal plate able to be expanded, but also the plate can be increased coronally to certain degree.
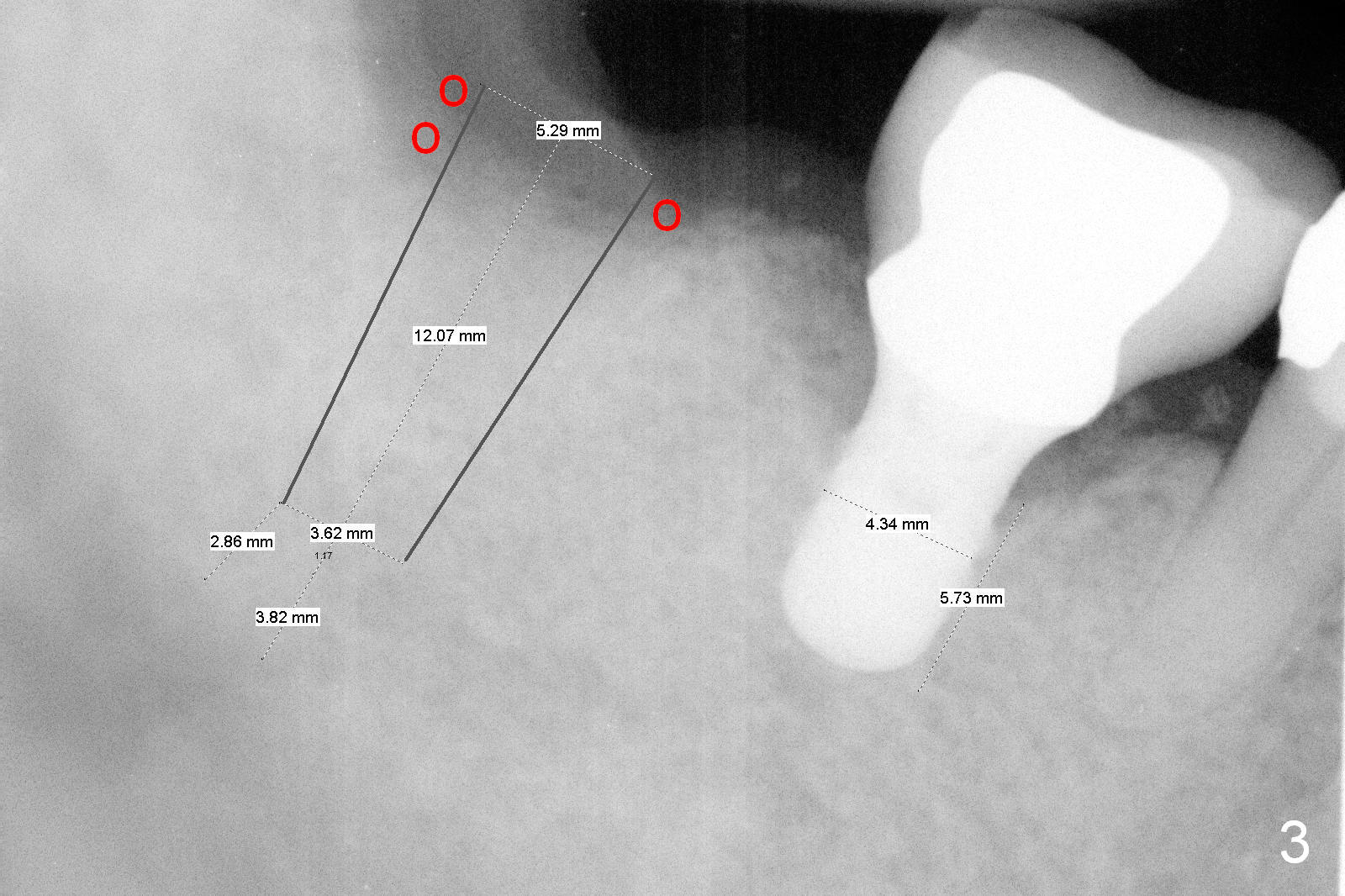
Fig.3 is a design to place a 5.3x12 bone level implant in the middle of the healing socket. The drawbacks are two folded. First the implant is placed too distally. Second, the implant is close to the underlying nerve.
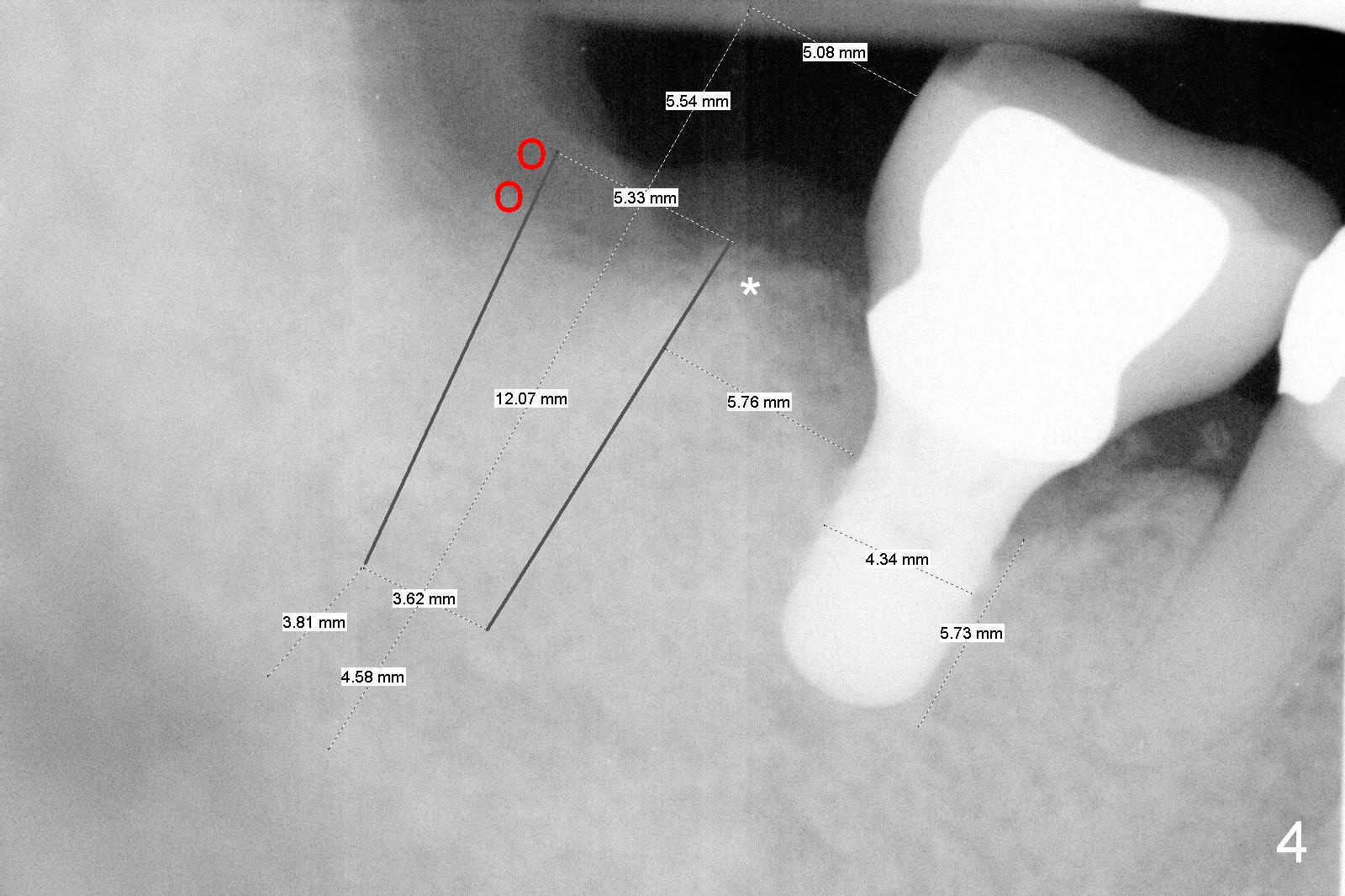
The design in Fig.4 overcomes these 2 shortcomings. The center of the implant is 5 mm from the neighboring tooth. Mesially there is more bone support (*), whereas distally bone graft is necessary (red circles). There is still enough space between the two implants; the minimum is 3 mm.
No matter which design, there is possibility of the buccal threads of the implant. Bone graft is expected. Collagen dressing should be cut in a ring shape, fixed by an abutment.
Also prepare osteotomes (including D shaped) and surgical handpiece and thin surgical bur in case the lingual plate has to be split and expanded.
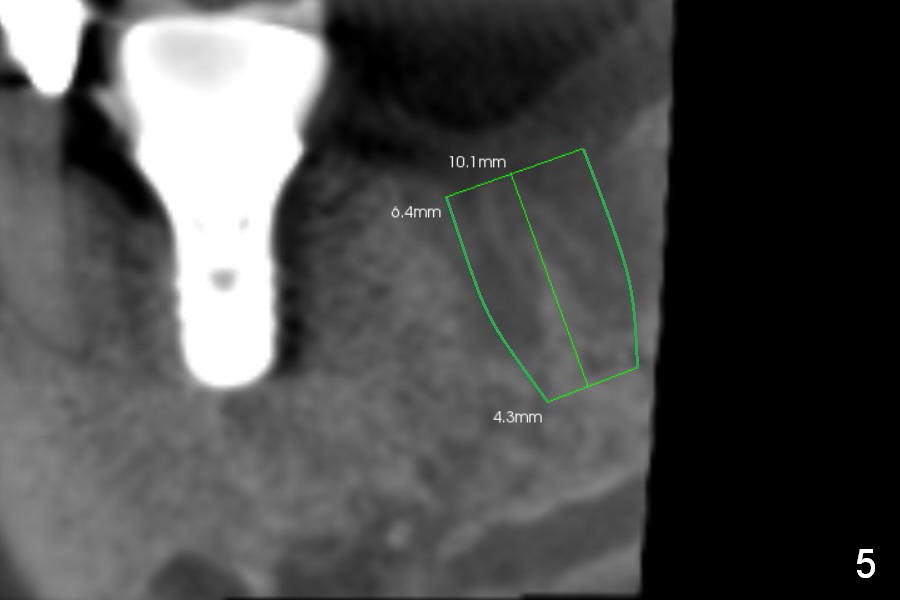
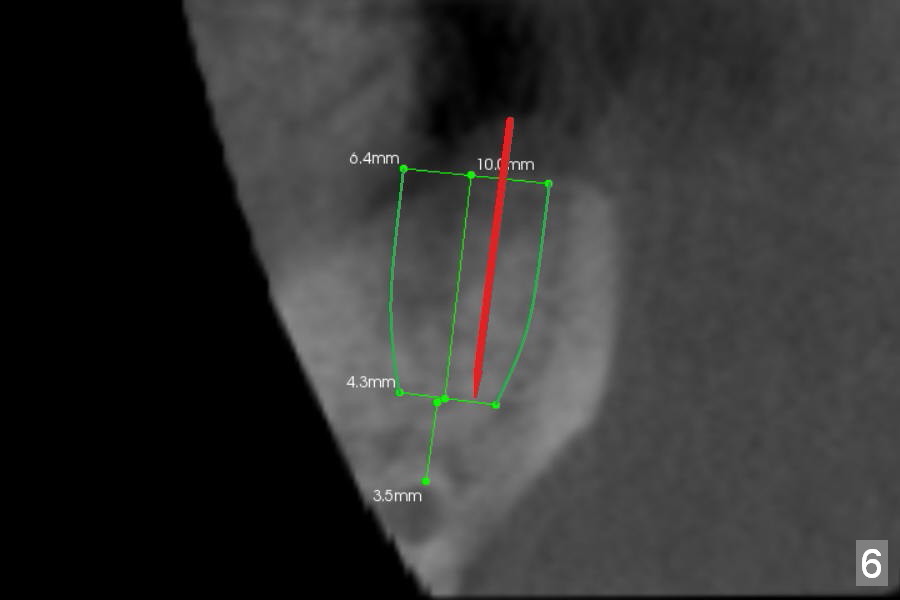
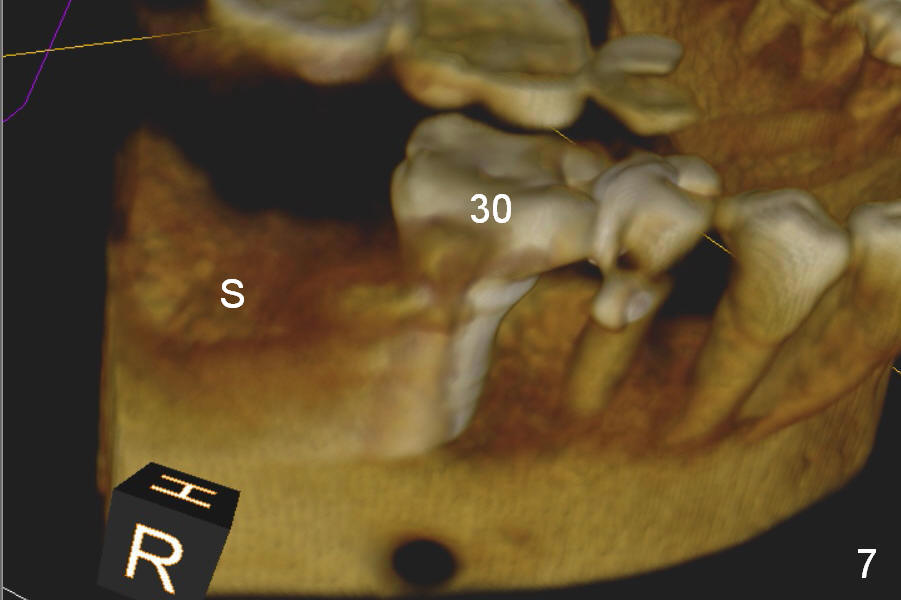
Preop CBCT shows that a 6.4x10 mm implant is appropriate if placed in the middle of the socket (septum), 6 mm from the crown of #30 (Fig.5). Coronal section confirms that because of the lingual slope of the socket, osteotomy should be placed lingually (Fig.6 red line). Three-D image is shown in Fig.7.
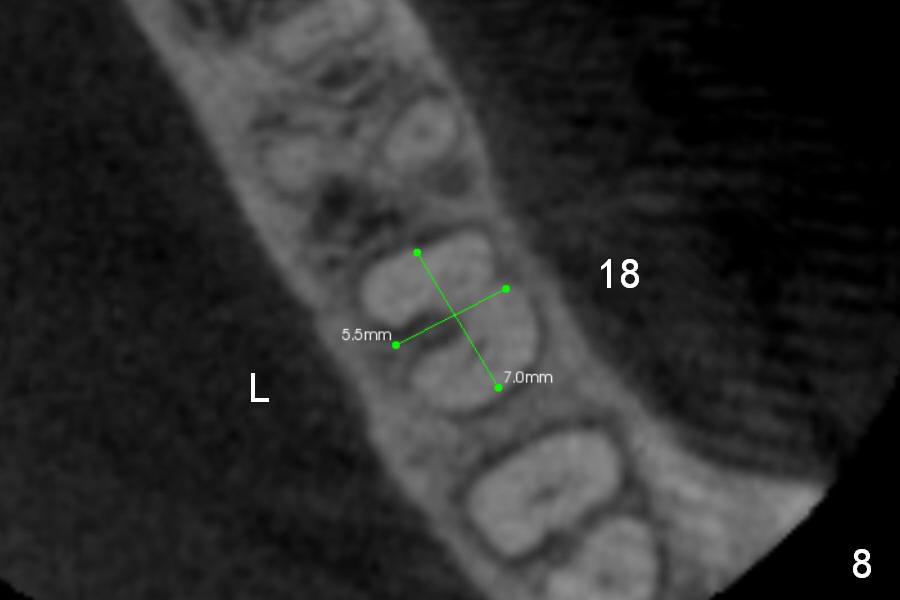
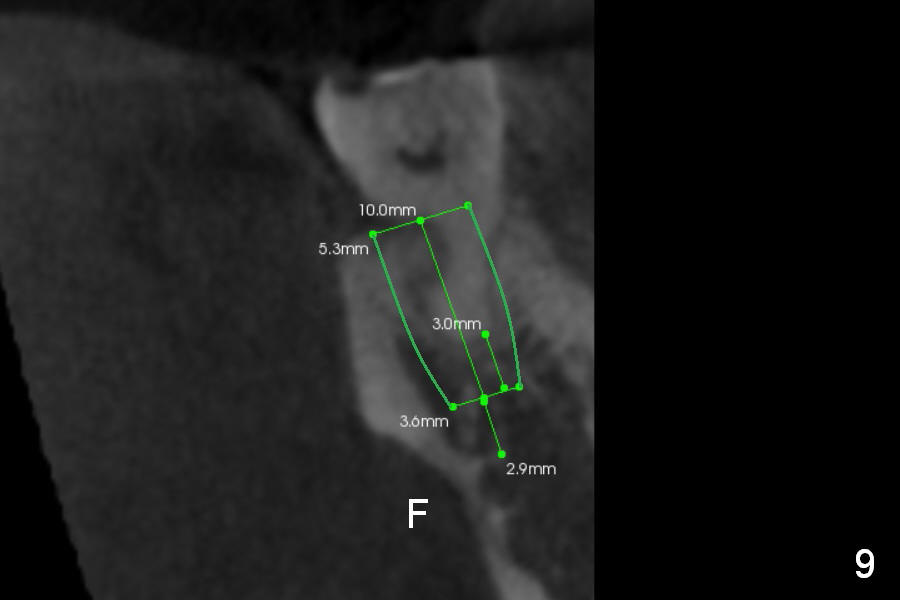
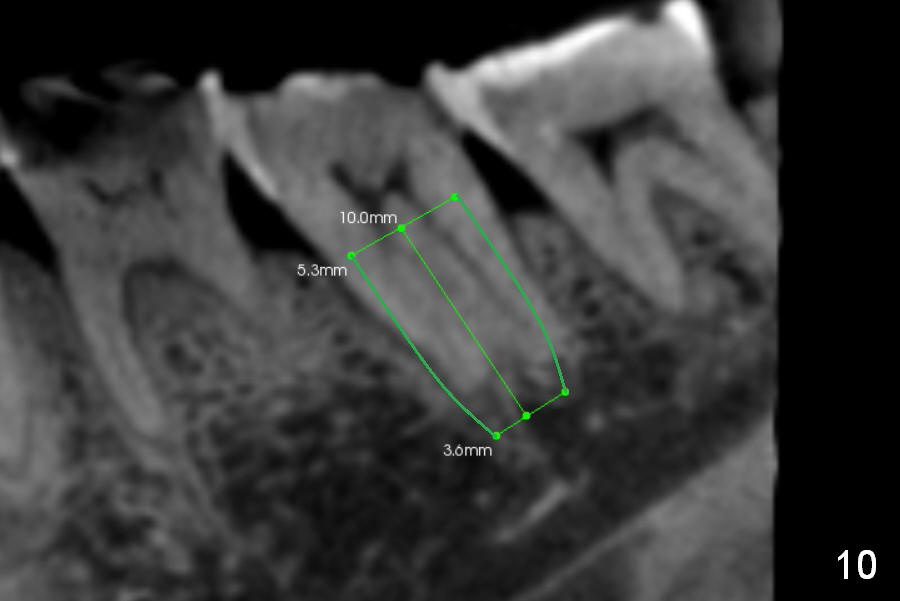
CBCT Analysis of the lower left 2nd molar reveals that the proper implant size is 5.3x10 mm (Fig.8-10). The root is C shaped; limiting factor is buccolingual width (5.5 mm, Fig.8 (axial section)). The major difference between #18 and 31 is the resorption of the buccal plate of the latter (traumatic extraction, Fig.9 (F: submandibular fossa)).
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 07/18/2015, last revision 10/27/2019