

,%20500-800%20HU,%20obliterates%20B-L%20space.jpg)
|
|
|
|
|
|
|
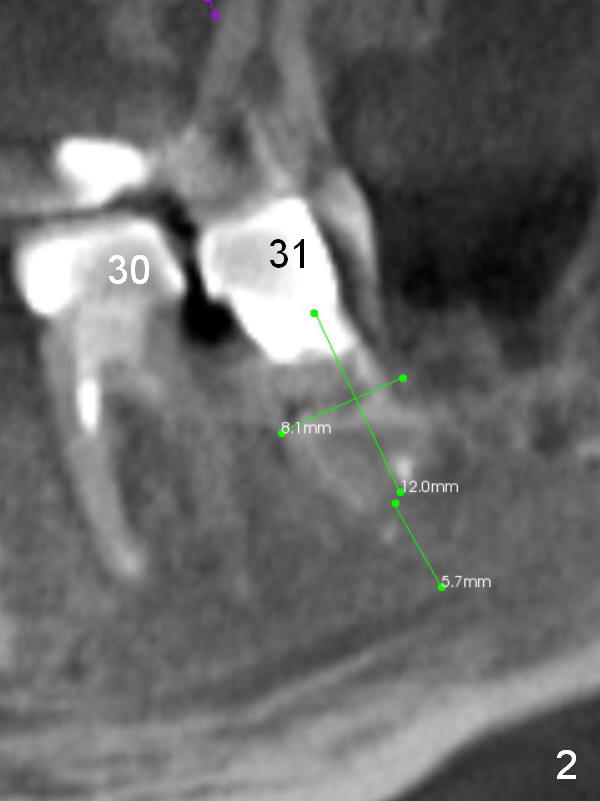
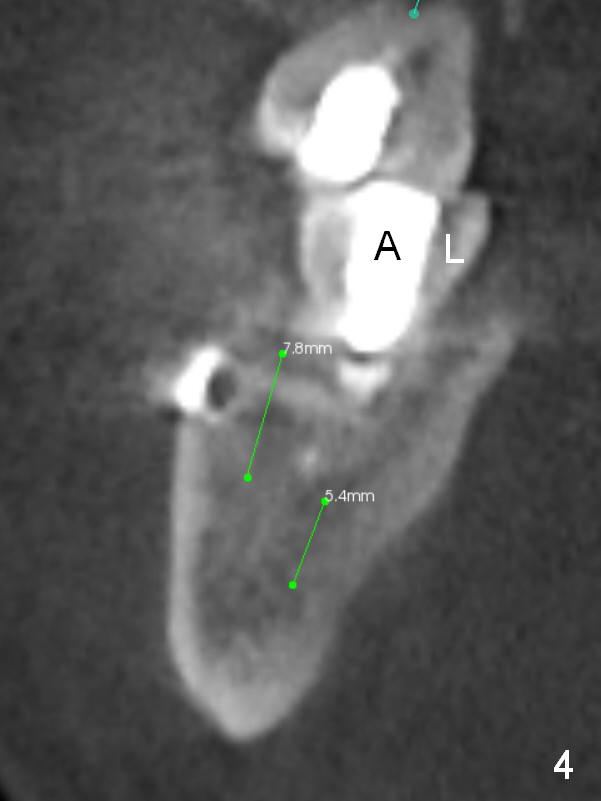
Immediate Implant in Non-Infected Socket
A 39-year-old man (ZC) fractures the lingual portion of the tooth #31 while eating peanut during Christmas (Fig.1 green arrows), a few months finishing #28,29 implant crowns. It fractures between the large amalgam (Fig.3 A) and the lingual portion of the tooth (L). It should be subgingival and nonsalvageable. Prepare crown prep or immediate implant. If the latter is indicated, the socket will be treated with 2% Xylocaine/1:50,000 Epinephrine. The distance between the apex of the socket and the Inferior Alveolar Canal is >5 mm (Fig.2,4). If osteotomy is controlled 3 mm beyond the apex of the socket, it is safe (Fig.3,5). A 5.9x10 or 12 mm implant should be able to engage to the buccal and lingual walls for additional stability (Fig.5), while there will be mesial and distal gaps to be filled with bone graft (Fig.3 red dots).
A 6 mm implant is indicated in the lower 2nd molar socket when there is no infection with enlarged socket. Oversized implants (7,8 mm) may invade the buccal plate.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 12/25/2015, last revision 12/25/2015