.jpg)



Post Cementation
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
3 Years 3 Months
Post Cementation |
Why Implant not Completely Seated?
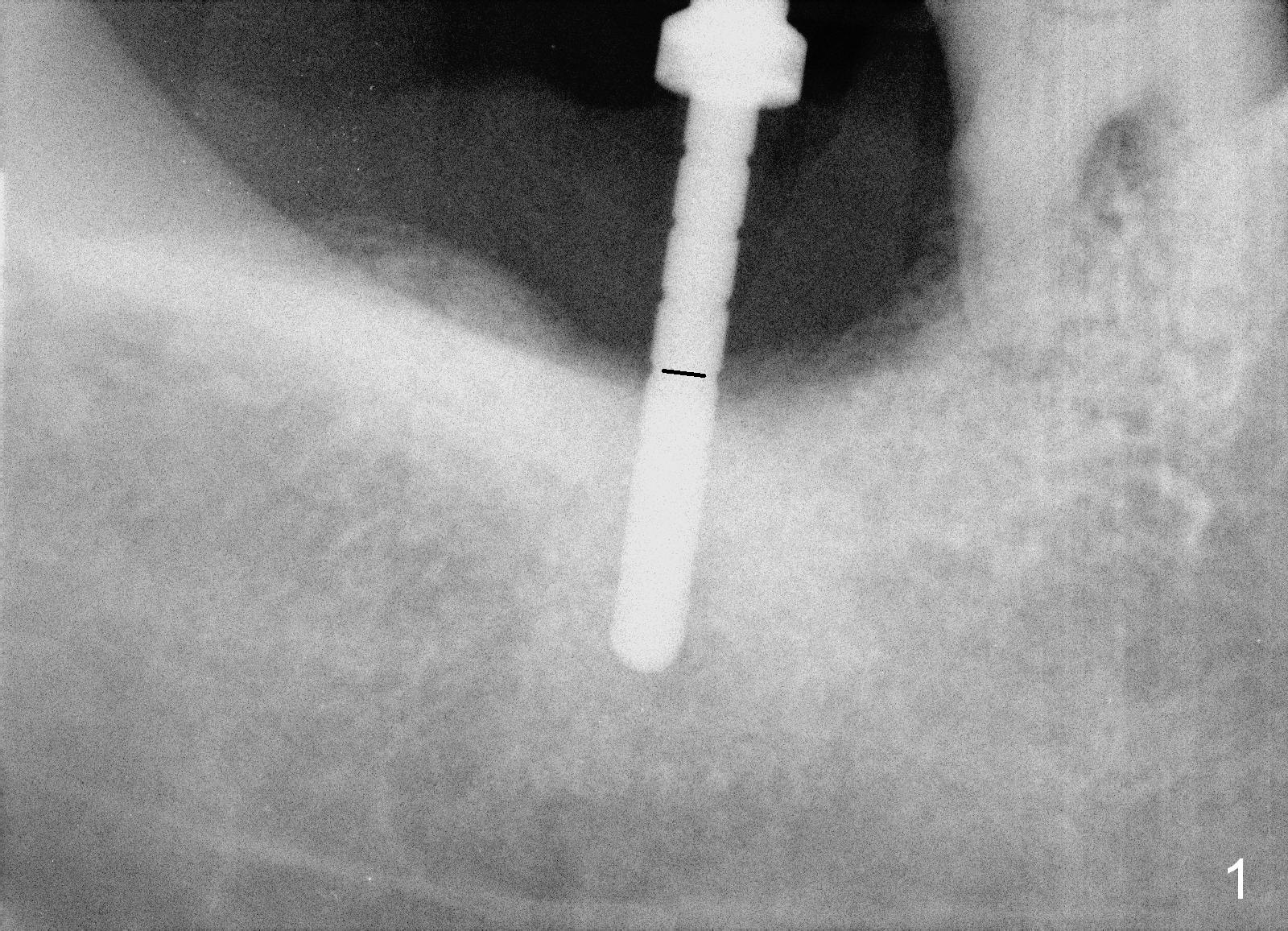
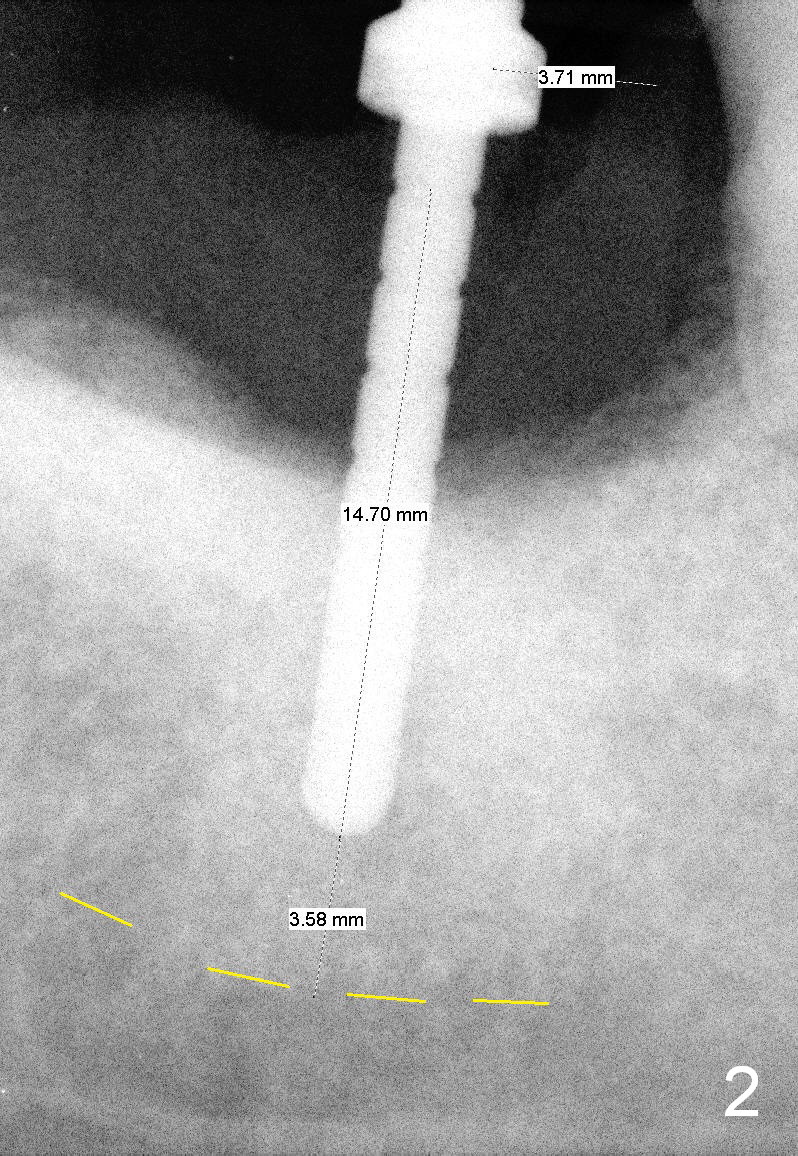
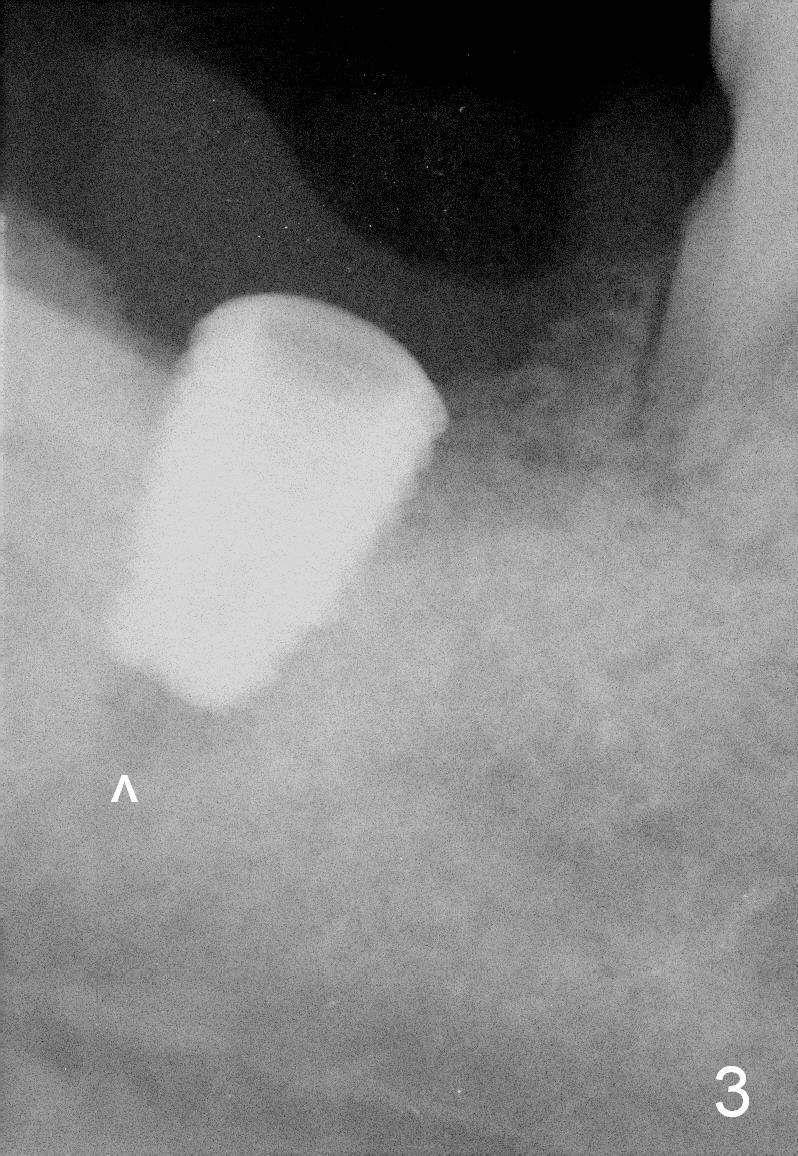
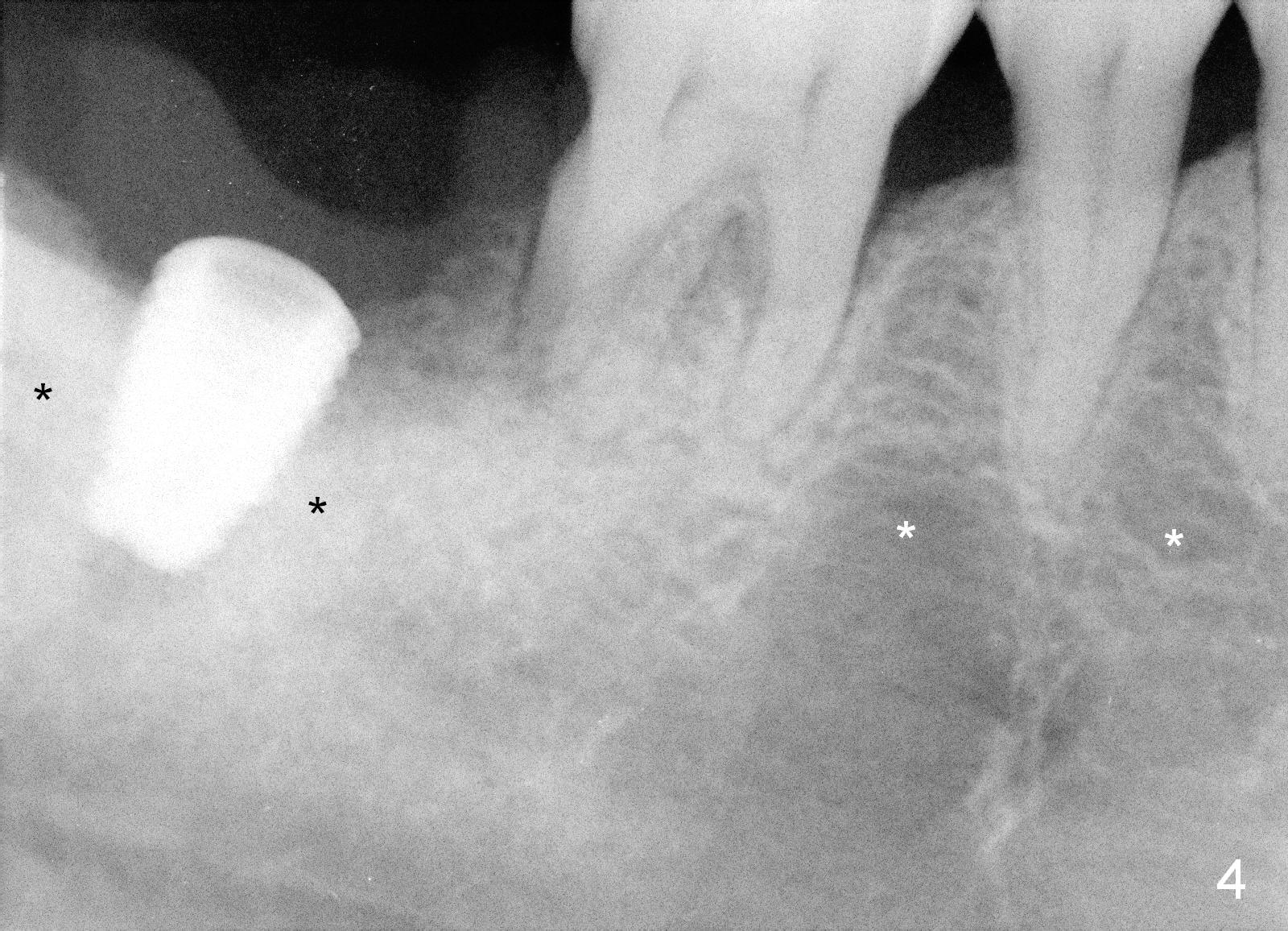
At first infiltration anesthesia is provided. When the anesthetic is administered buccally, purulent discharge is from the buccal sulcus. The tooth #31 has mobility III. There is abundant granulation tissue in the socket after extraction. The buccal plate is absent, while the lingual plate is ~ 1 mm above the bottom of the socket. The osteotomy is initiated lingually with a 2 mm pilot drill (stopper set at 8 mm). The 1st intraop PA is taken with a parallel pin (Fig.1 black line is the mark of 8 mm). The depth of the osteotomy is 14 mm from the gingival margin (Fig.2) with 3 mm away from the upper border of the Inferior Alveolar Canal (yellow dashed line). Further osteotomy is finished with reamers following Inferior Alveolar Nerve block for pain control. A 5.9x8 mm implant is not completely seated (insertion torque >60 Ncm; Fig.3,4; arrowhead: the apical end of the osteotomy). Further torque (Fig.5) results in failure of the engagement of the implant driver to the implant. There is a remote possibility that the newly formed buccal plate is fractured. Why is the implant not completely seated?
First of all, the bone density at the site of #31 is much higher (Fig.4 black *) than that around the neighboring teeth (while *). Second, a 5.3x8 mm drill and 5.9x8 mm one if needed should have been used prior to implant re-insertion.
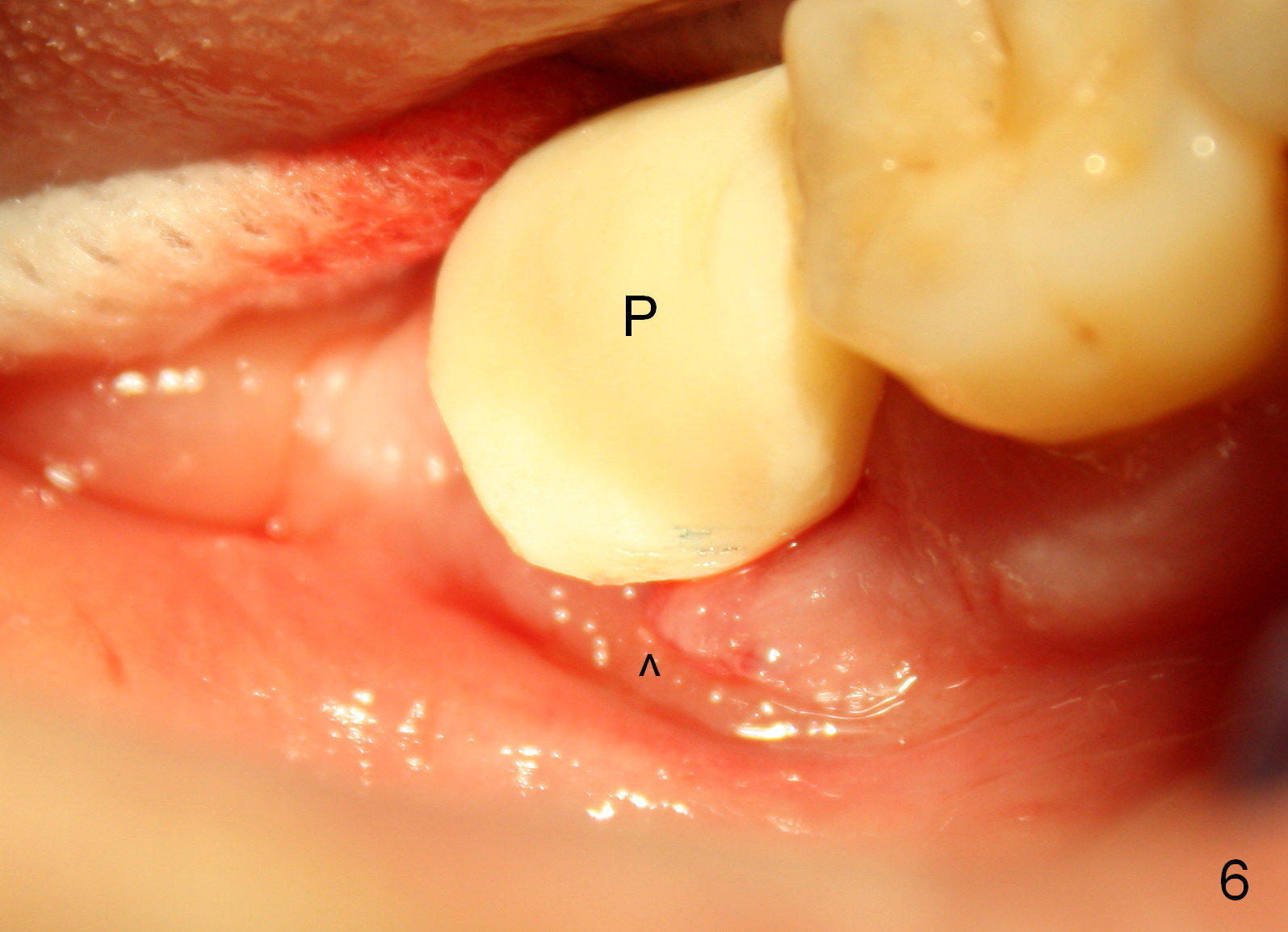
Fortunately the distal crest is at the same level of the implant plateau. With bone graft (Fig.5 *: autogenous bone + Osteogen), the implant threads may not be exposed. Because of the incomplete implant seating, a shorter abutment is used (A: 7.8x4 (4.5) mm). Prior to bone grafting, a piece of collagen membrane (6 month resorption) is placed buccally due to the lacerated buccal gingival margin (Fig.6 ^). An immediate provisional is fabricated and cemented temporarily (Fig.6 P). The opposing is a removable partial denture.
The lacerated buccal gingiva appears to have healed 1 week postop (Fig.7). The coronal portion of the buccal plate at #31 remains atrophic (*) as before (Fig.6), which may help the gingiva (Fig.8 (lingual view) *) adapt to the abutment (arrowheads) and the provisional (P).
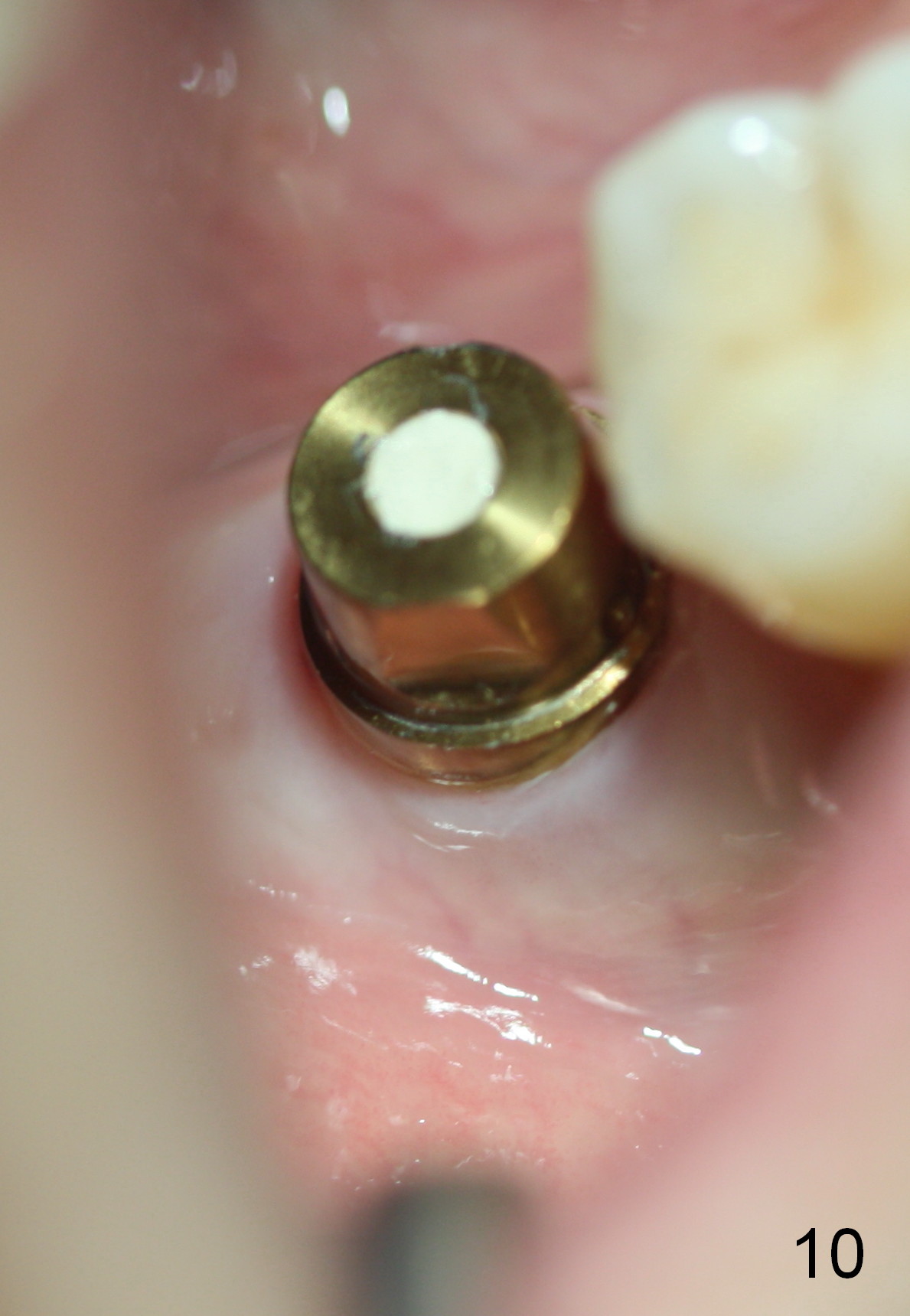
Three months postop, the 1st 2 coronal threads of the implant appear to be covered by low density bone, while the apical radiodensity increases (Fig.9). Twenty days later, the patient returns for final restoration; the gingiva around the abutment is healthy (Fig.10).
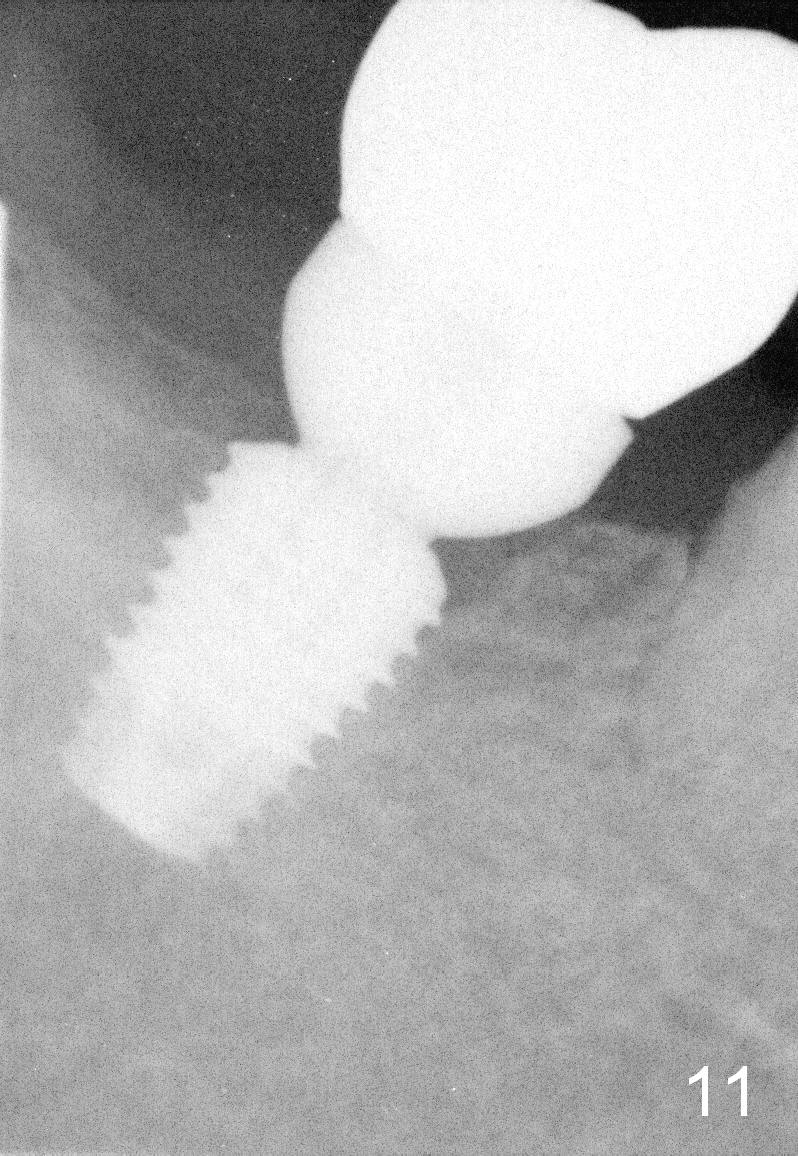
Bone density around the implant increases 6 months post cementation (Fig.11).
Return to
Professionals,
Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 04/13/2015, last revision 11/14/2018