|
|
|
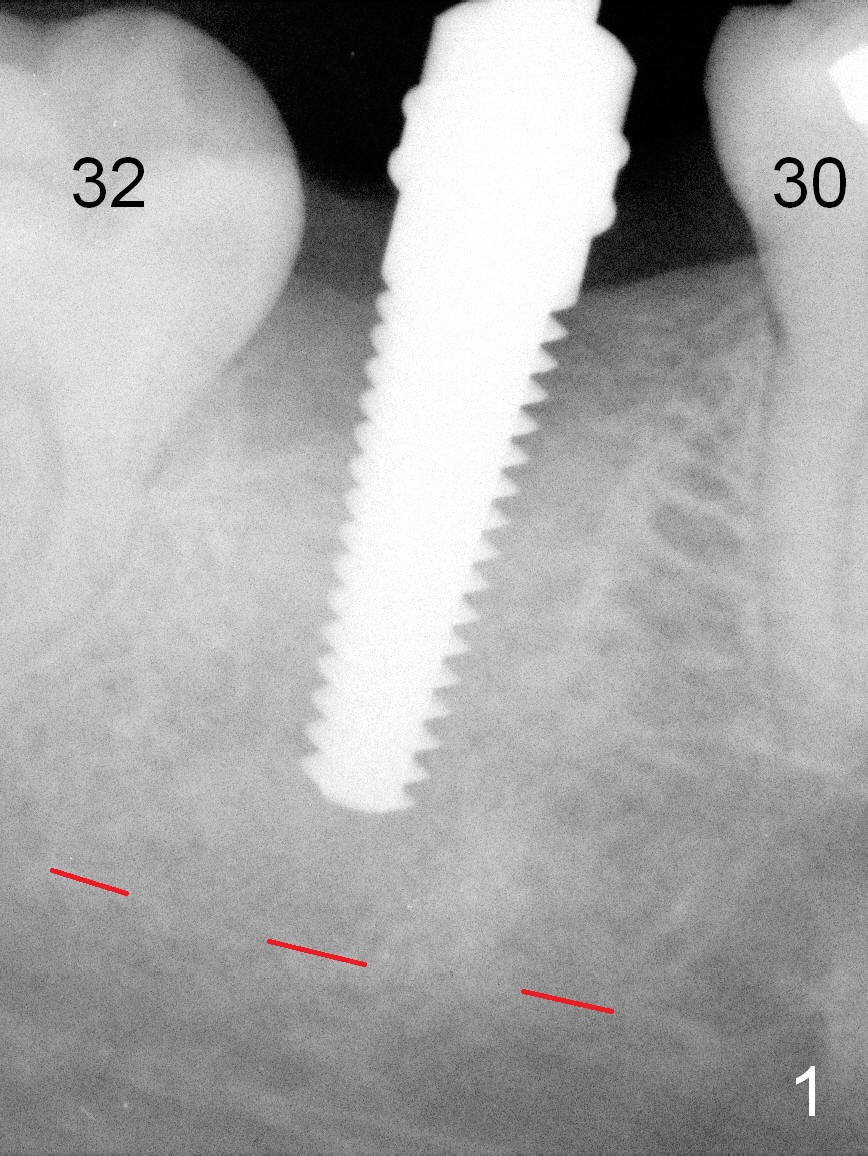
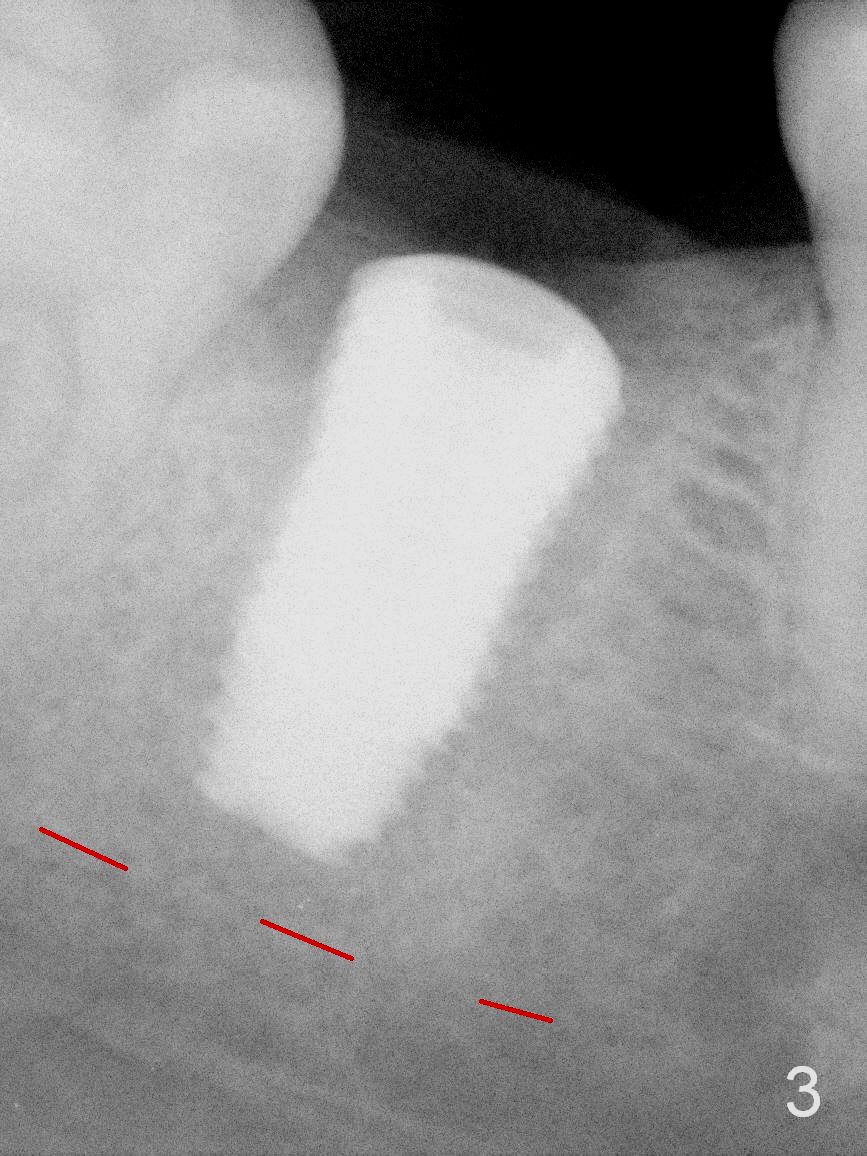
After infiltration anesthesia, the gingiva over the healing socket of #31 looks transparent and tender, 2 months post extraction. The buccal and lingual plates are intact and wide. Osteotomy is initiated by using a series of osteotomes. First, bone scalpels (4,5,6 mm) are inserted into the socket (no incision by traditional scalpel), followed by bone blades (4, 5.5 mm) and rounded tapered osteotomes (2,3 mm). The depth is 14 mm from the gingival margin. The bone expansion and condensation continues with insertion of 4.5 mm (not stable) and 5 mm (barely stable, Fig.1) taps. When a 6 mm tap is inserted, stability is acceptable. Placement of a 7 mm tap would produce satisfactory stability, but it may be too large for the mesiodistal space. A 6.5x12 mm bone-level implant is placed with insertion torque ~ 55 Ncm (Fig.3). In fact the distal of the implant is supracrestal, retrospectively, when periimplantitis develops.
Xin Wei, DDS, PhD, MS 1st edition 08/20/2015, last revision 12/25/2019