

|
|
|
|
|
|
Treat Healed Socket as Infected One M
A 22-year-old man (HW) had #31 extracted without bone graft in other office 2 months ago. The socket appears to have healed asymptomatic. Pre-extraction panoramic X-ray shows periapical radiolucency (Fig.1 <). It is unknown that the lesion was eradicated during extraction or not. To reduce post-implant infection (1,2), oral antibiotic is to be taken preop and the osteotomy, once formed, will be treated with an antibiotic (Clindamycin or Metronidazole) or placebo (2% Xylocaine, 1:50,000 Epinephrine). If autogenous bone is harvested from the osteotomy, the bone will be mixed with an agent before placement. A case will be selected if extraction occurs less than 6 months. The 1st case is assigned to Clindamycin group, the present case to Metronidazole, the next to control as shown below.
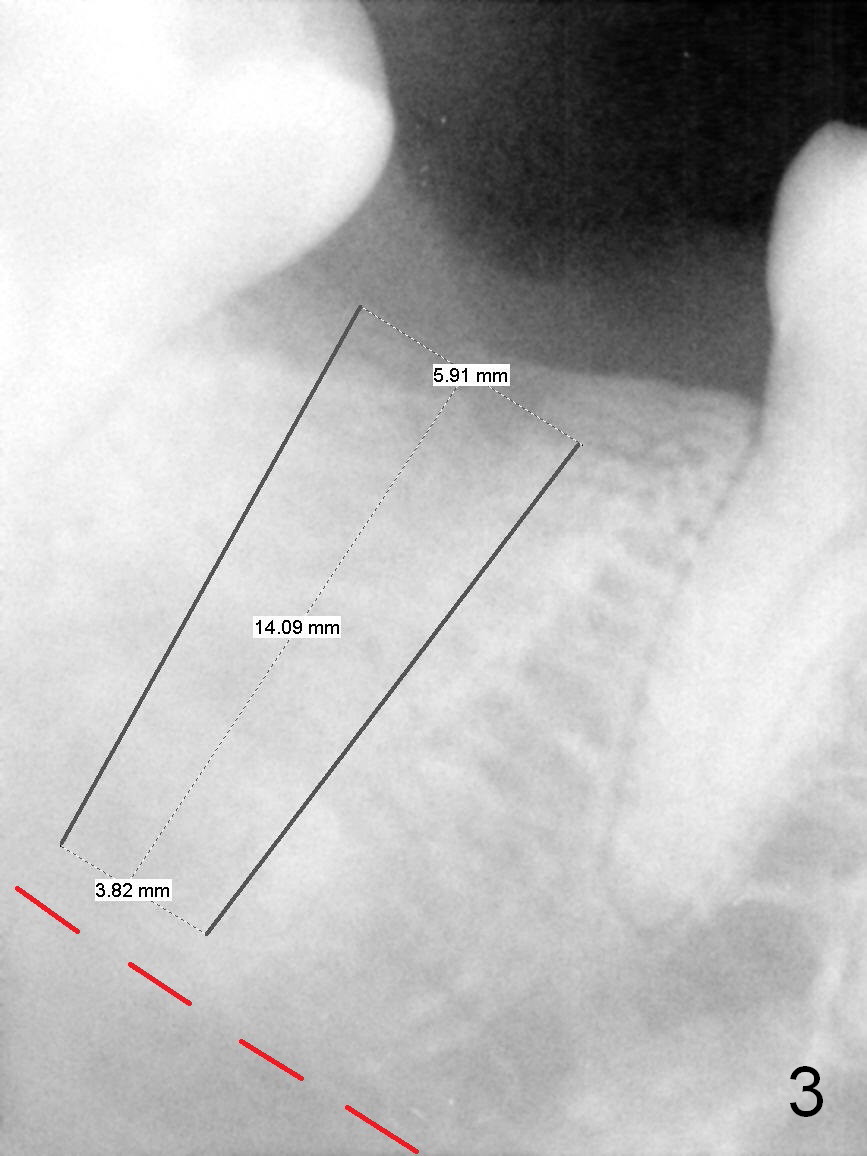
PA in Fig.2 is taken 2 months post extraction, while Fig.3 shows design of a 5.9x14 mm bone-level implant. It appears that the implant is a little too long (red dashed line: the superior border of the Inferior Alveolar Canal). Initial osteotomy depth will be 12 mm. In fact the implant was designed to be supracrestal distal (mistake, even if bone graft is well executed). An incision will be made for visibility.
Return to
Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 08/17/2015, last revision 12/27/2019
Table: Localized Use of Antibiotic for Healed Socket
| Clindamycin | Metronidazole | Control | ||||||||||
| N | A | S | # | N | A | S | # | N | A | S | # | |
| 1 | WJ | 75 | M | 31 | HW | 22 | M | 31 | ||||
| 2 | ||||||||||||
| 3 | ||||||||||||