
|
|
|
|
|
|
|
|
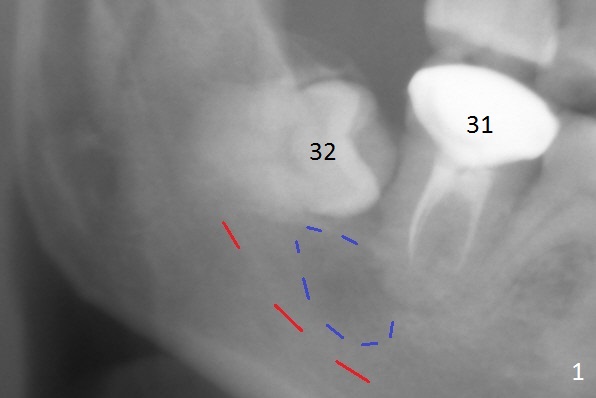
Abscess from #32 or 31?
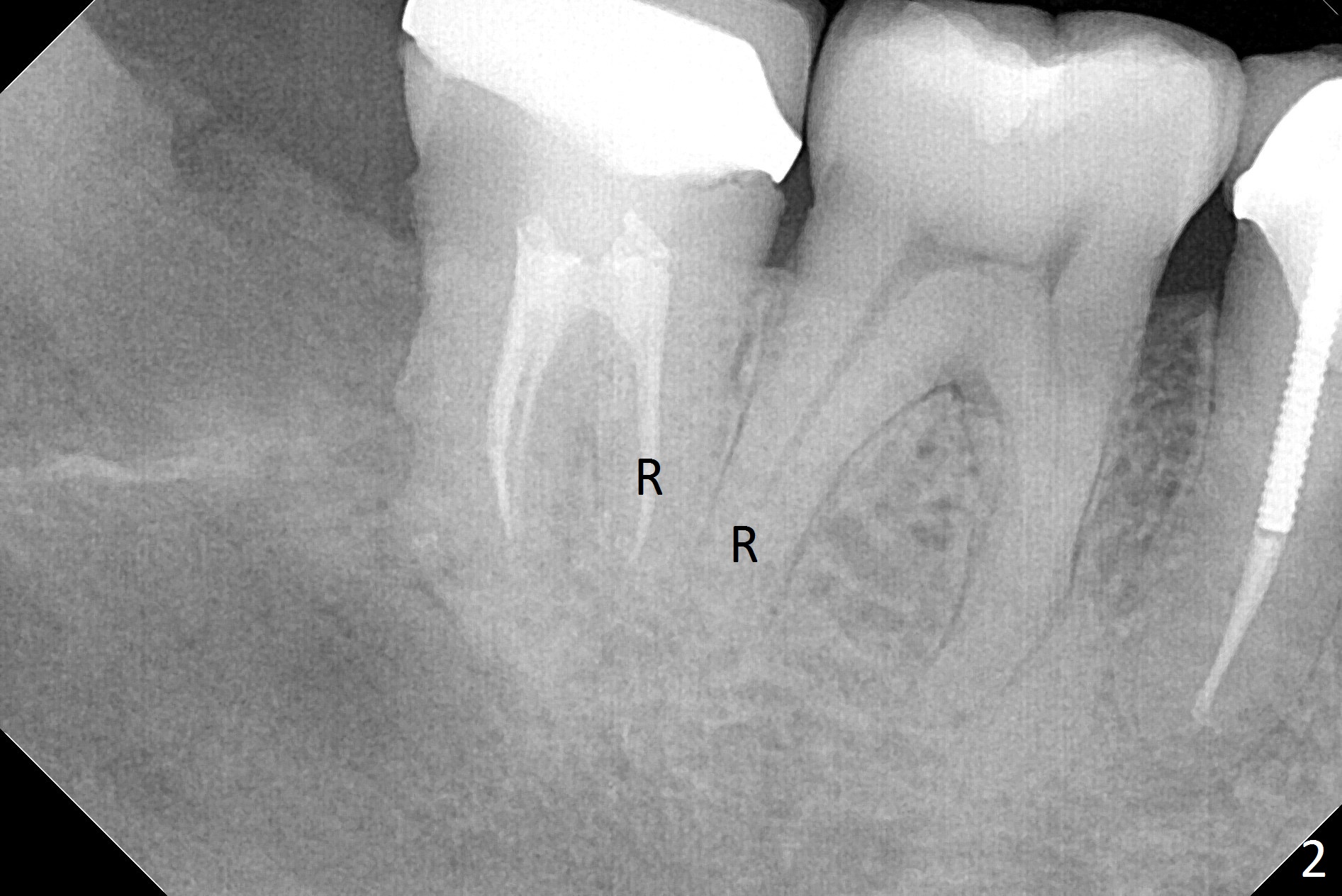
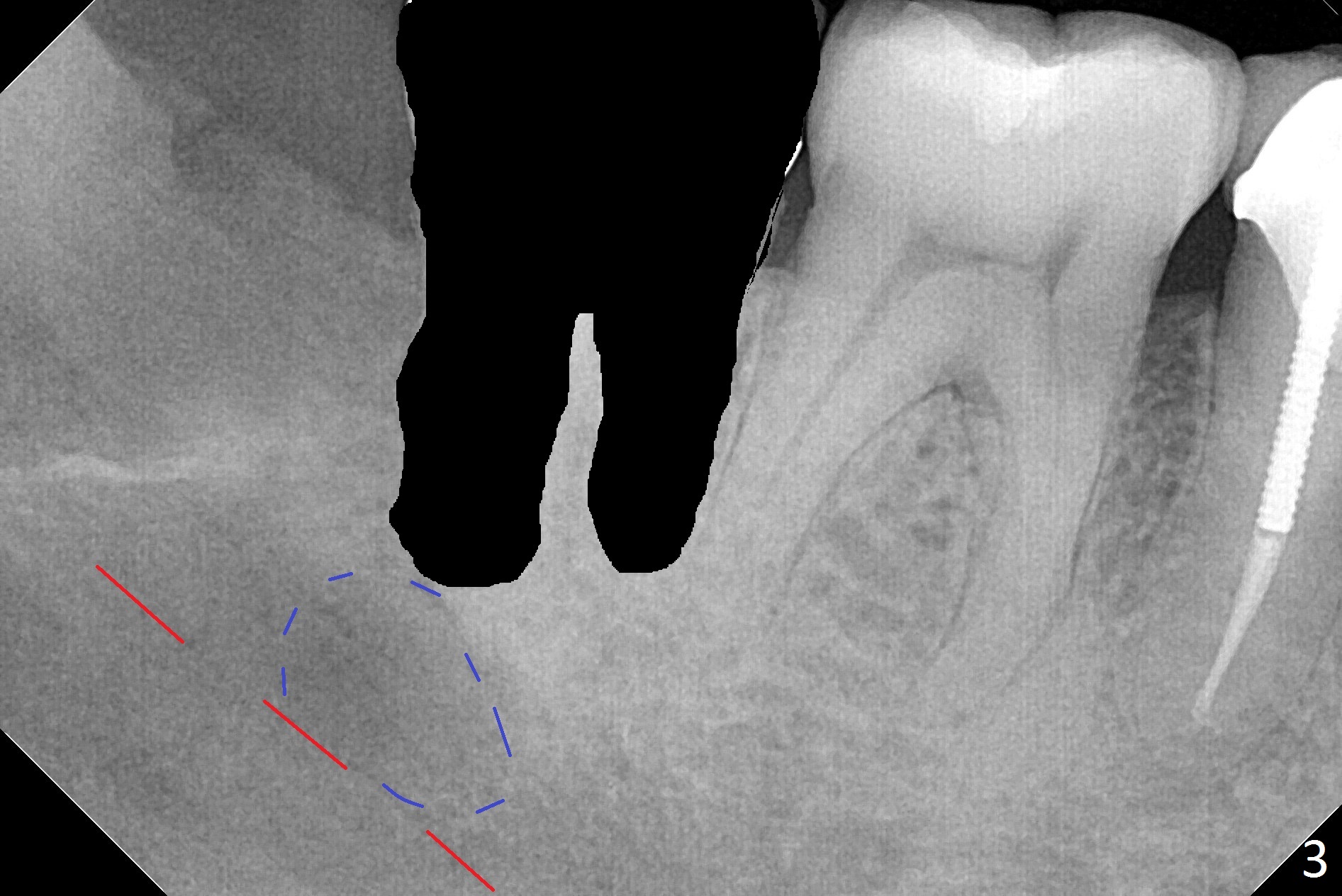
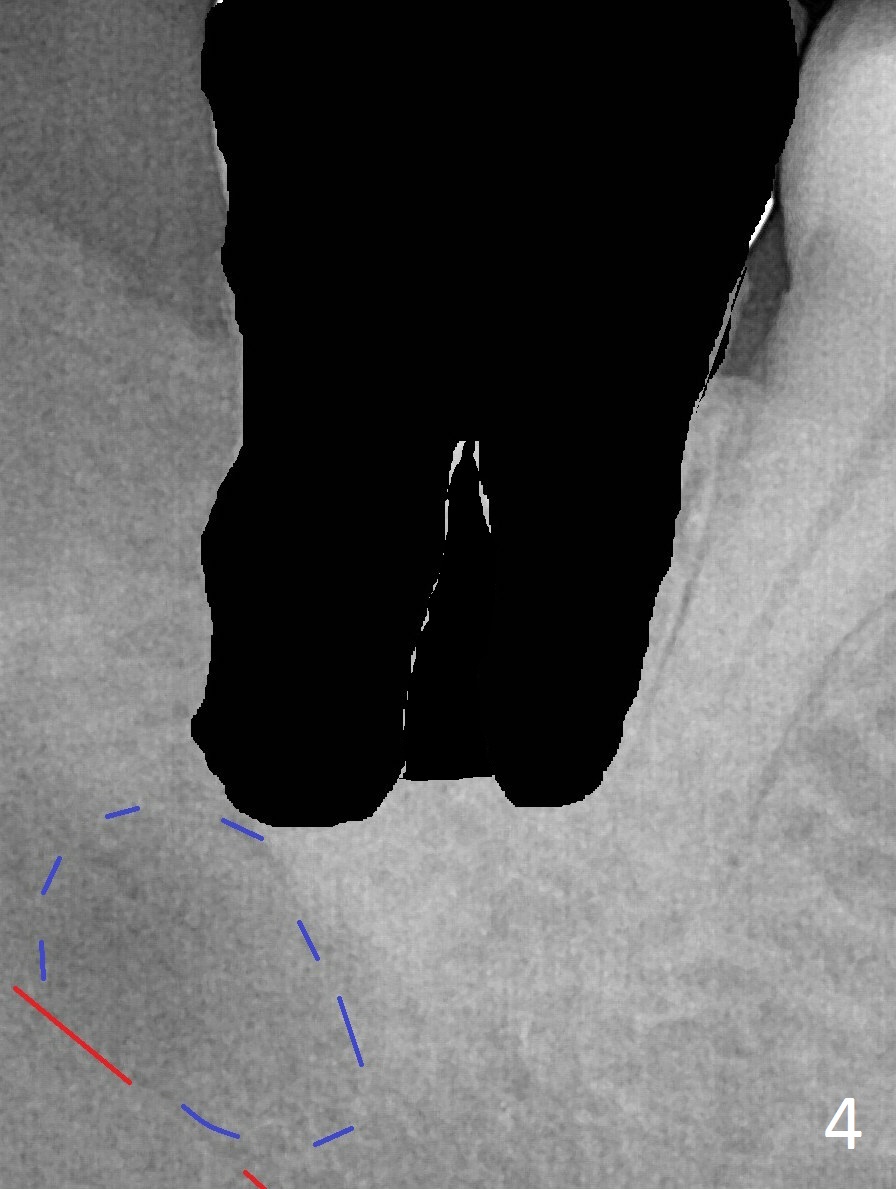
A 45-year-old woman presents to clinic with swelling and pain from the lower right posterior region. The tooth #32 is fully bony impacted. The distolingual gingiva of #31 is erythematous with deep pocket. The tooth is sensitive to percussion. Preop panoramic X-ray shows a radiolucent lesion between #31 and #32 (Fig.1 blue dashed line). Initial impression is infection from #32. Extraction of the latter turns out to be difficult. Purulent discharge is coming from underneath the coronal portion of the tooth. Curettage of the radiolucent lesion leads to hemorrhage. The curettage is not aggressive because of the underlying Inferior Alveolar Canal (red dashed line). Following copious irrigation, a 10x20 mm Osteogen plug is inserted into the socket with incision closure. Postop PA reveals that the roots the teeth #31 and 30 approximate to each other (Fig.2 R). In case the tooth #31 needs to be removed (Fig.3 black area), osteotomy for immediate implant will be established in the middle of the septal stump (Fig.5 red arrow) after removal of the coronal septum (Fig.4). CBCT may be necessary for determination of the osteotomy depth.
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS,
Antibiotic
Xin Wei, DDS, PhD, MS 1st edition 04/09/2017, last revision 04/09/2017