
|
|
|
|
|
|
|
|
Lingual Nerve Block
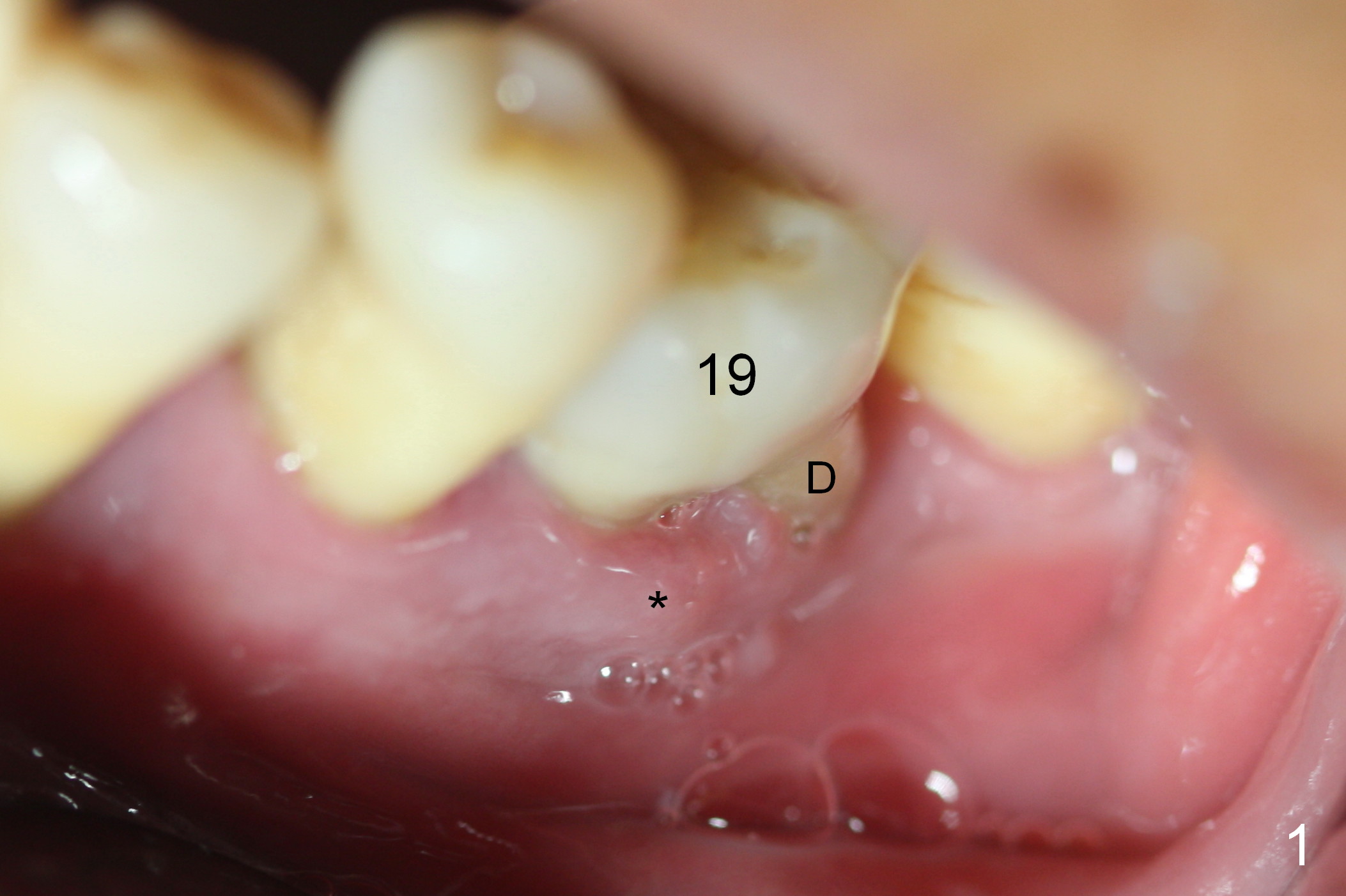
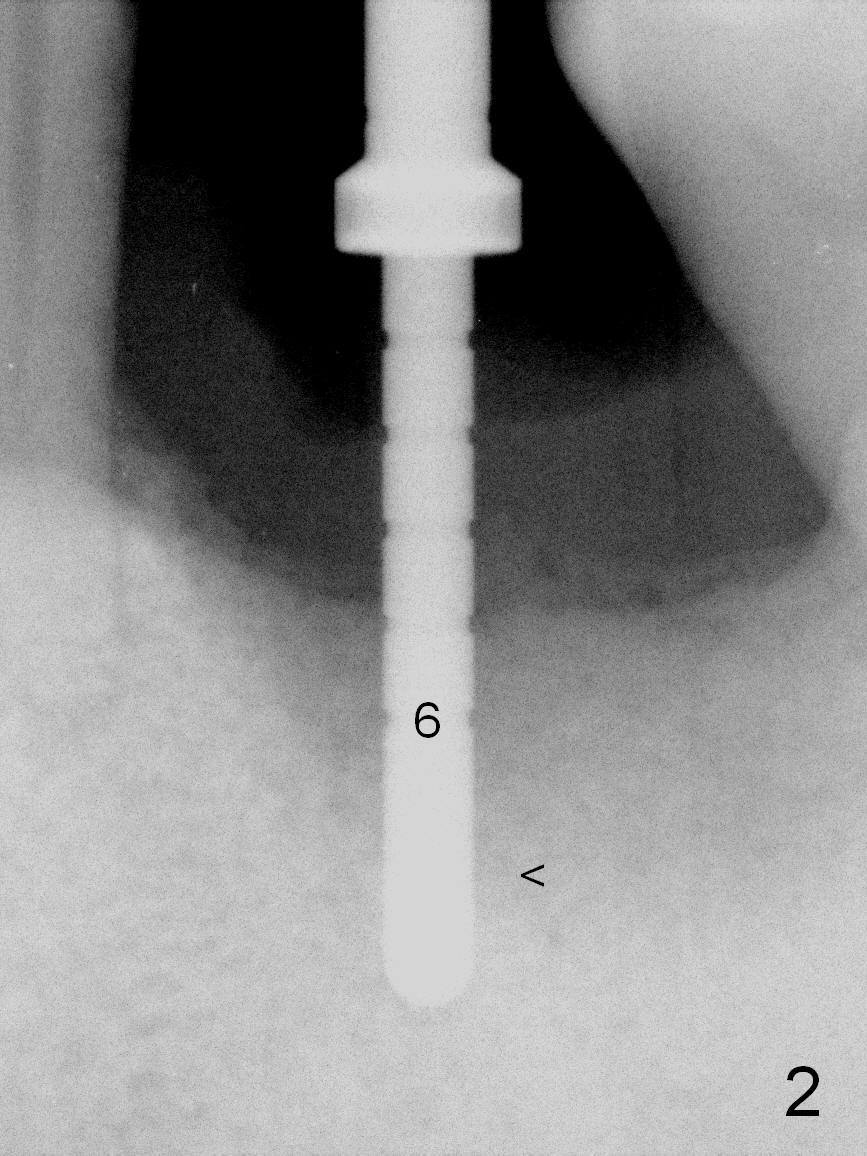
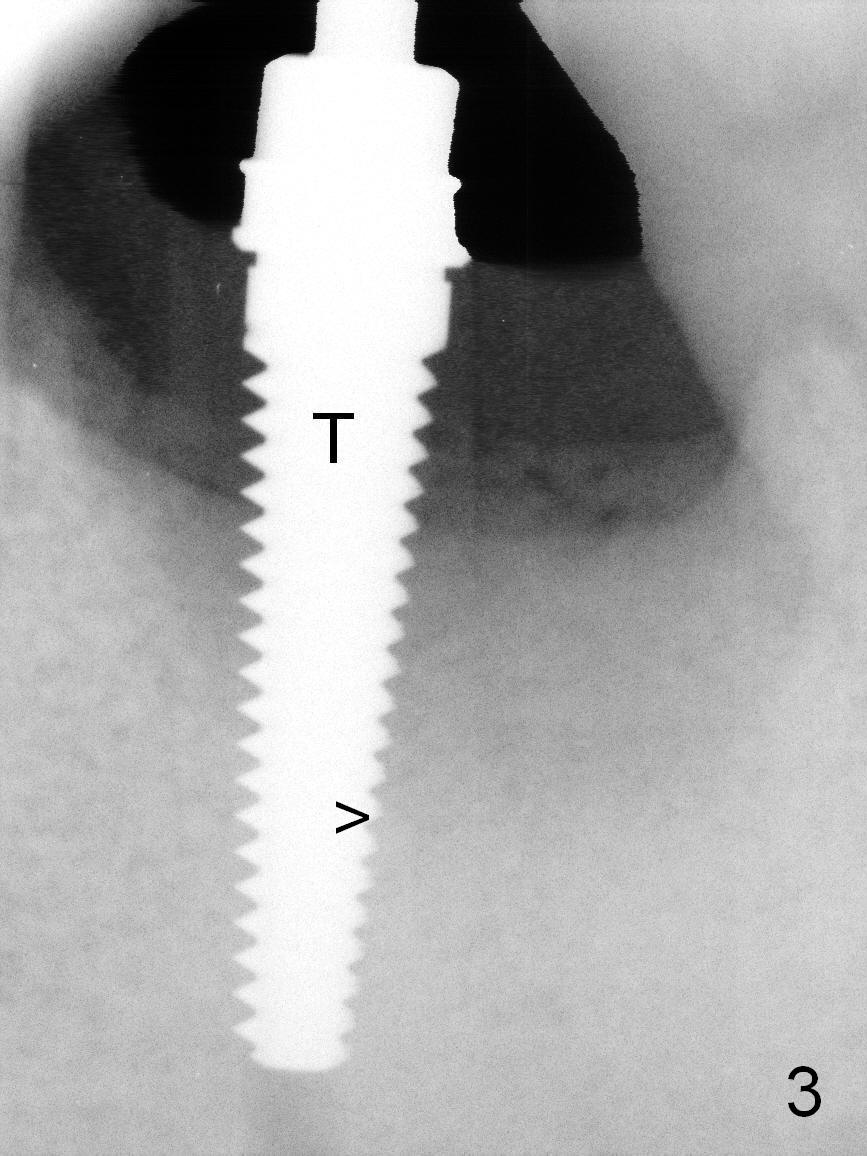
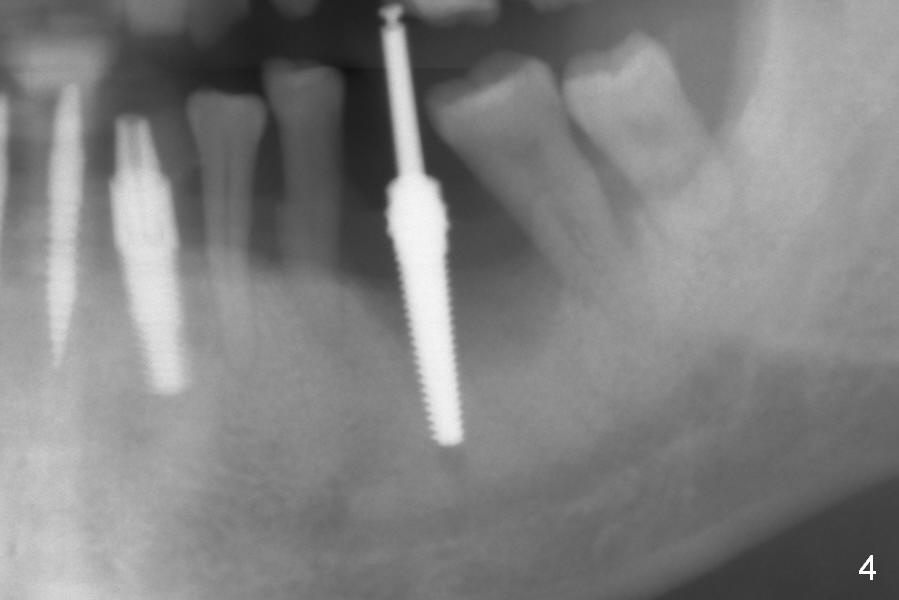
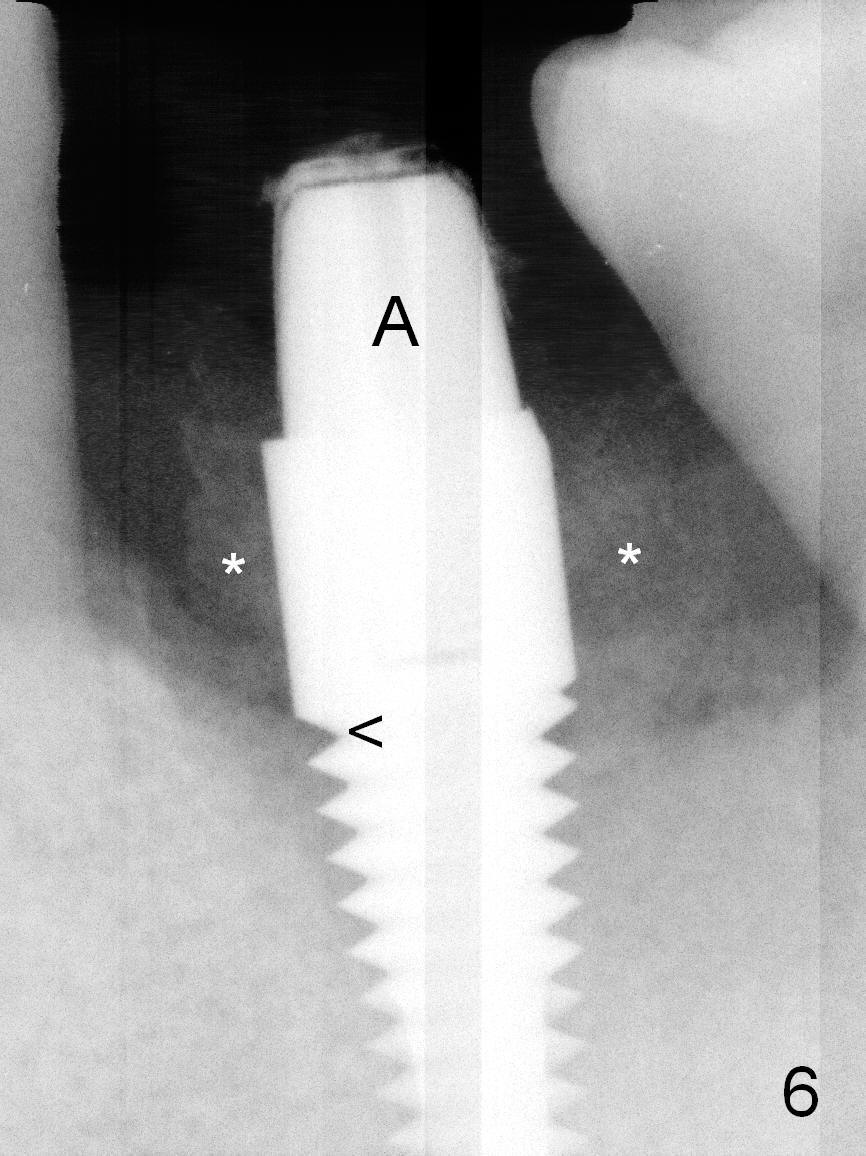
When the patient returns for #19 extraction and immediate implant, there is buccal (Fig.1 *) and lingual gingival swelling. The distobuccal root is exposed (D). Both the buccal and lingual walls are low. There is no septum. After removal of granulation tissue, an osteotomy is established in the bottom of the socket (slightly mesiolingually). The depth is approximately 3 mm in new bone (half of 6 mm and arrowhead). When the depth increases approximately 6 mm in new bone (Fig.3 arrowhead with 6x20 mm tap (T) in place), the Inferior Alveolar Canal is still invisible in PA. Panoramic X-ray has to be taken (Fig.4). So far infiltration anesthesia has been administered. When #2 sensor is inserted in the lingual vestibule, the patient feels pain and nausea. Lingual Nerve block is provided. The patient feels pain when further osteotomy is carried on. Since the depth of the osteotomy is confirmed by panoramic X-ray, Inferior Alveolar Nerve block is added. A 6x17 mm tissue-level implant is placed with clearance from the Inferior Alveolar Canal (Fig.5: red dashed line: the superior border of the Canal). Therefore, Lingual Nerve block allows lower placement of sensor so that the Inferior Alveolar Canal is detectable by PA.
The implant is placed lower by 1 thread (compare arrowheads in Fig.5,6). Bone graft (Fig.6 *) and Osteoplug are placed in the remaining socket (mainly mesiobuccodistally). An abutment (A) is placed for immediate provisional.
Return to Lower Molar Immediate Implant,
Lower Arch Reconstruction,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 12/08/2015, last revision 12/08/2015