

|
|
|
|
|
|
|
|
|
|
|
|
Immediate Implant or Not
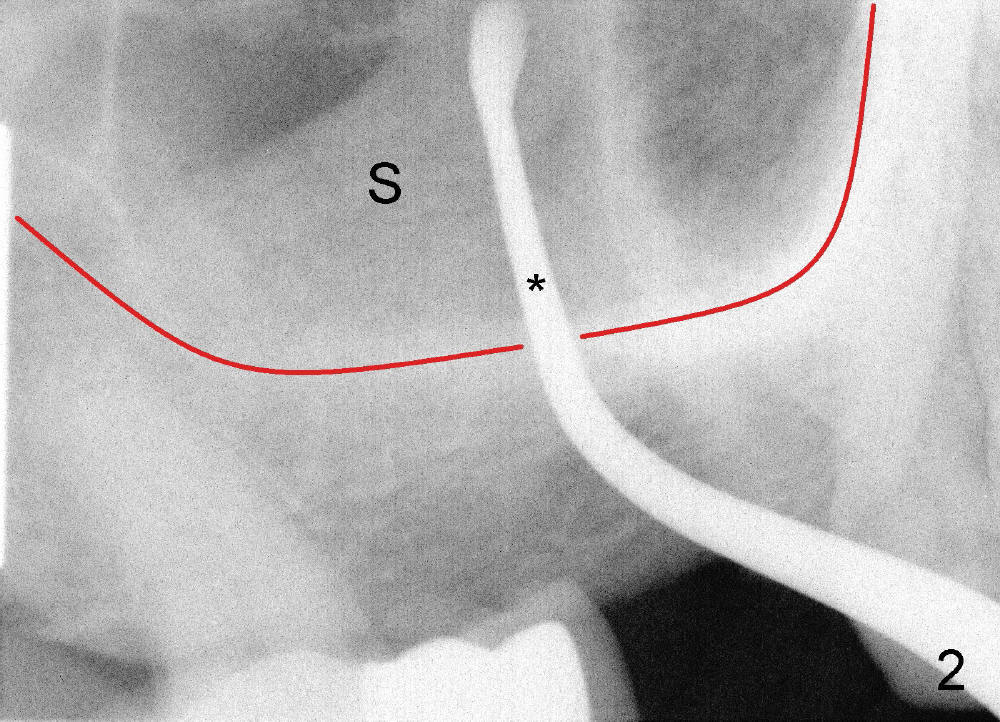
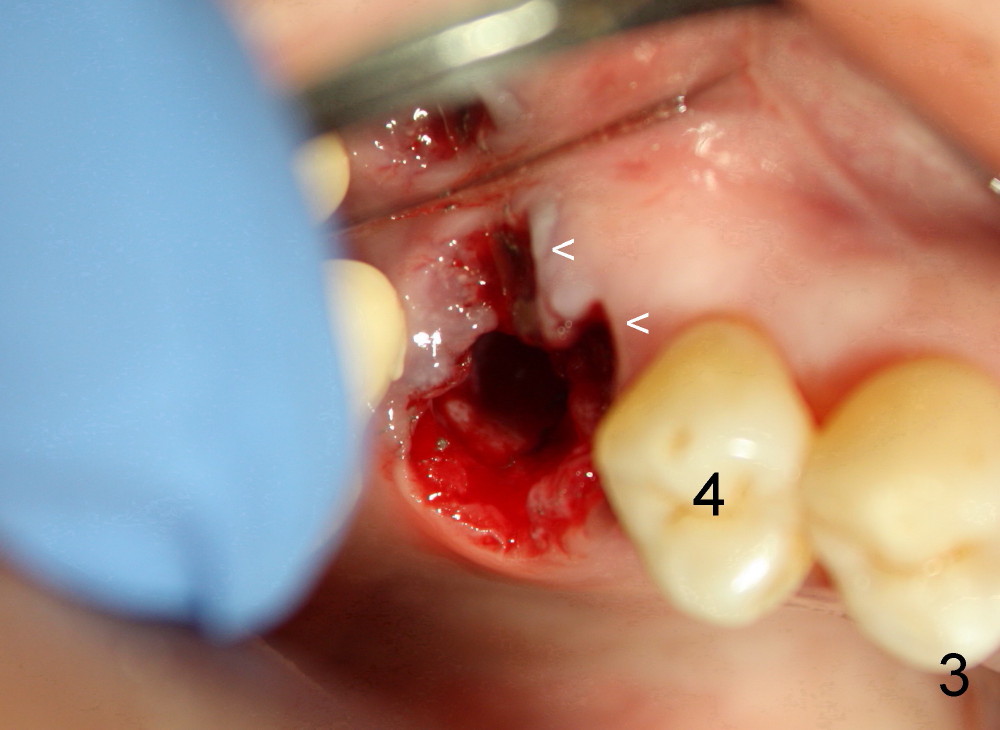
Immediate implant is not placed in this case (#3, the upper first molar) mainly because of inexperience. Apparent contraindications are sinus perforation (Fig.2) and large buccal bony (around the buccal roots, Fig.1) and gingival (Fig.3 <) defects). Even though primary stability may be achieved, implant threads may be exposed.
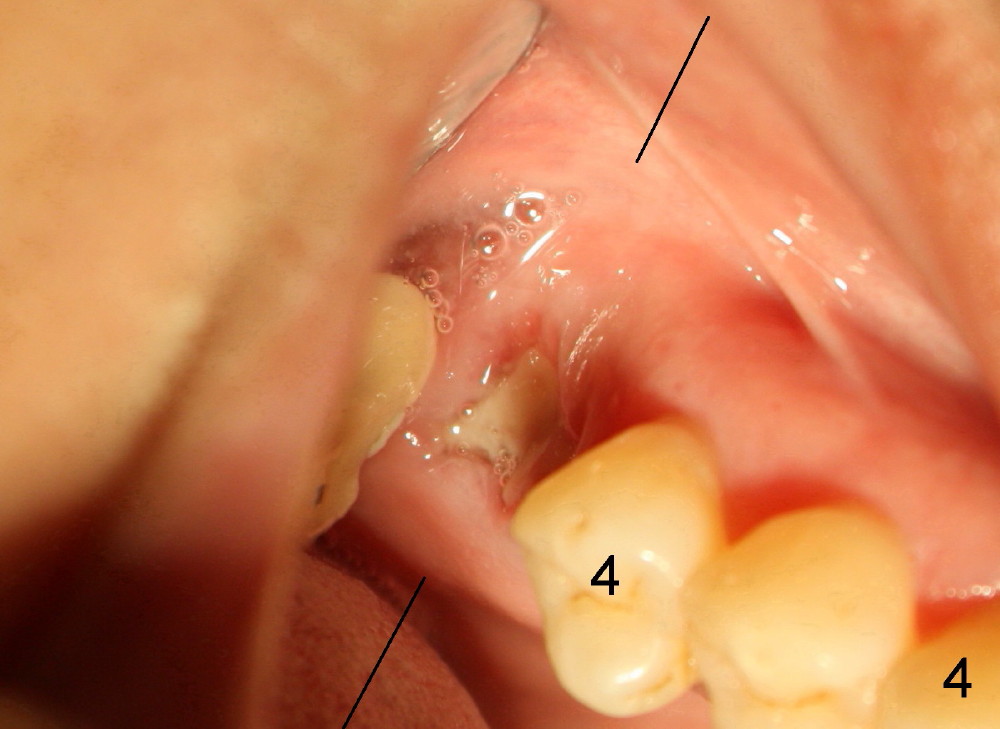
Surprisingly, one week post-extraction the wound heals nicely (Fig.4).
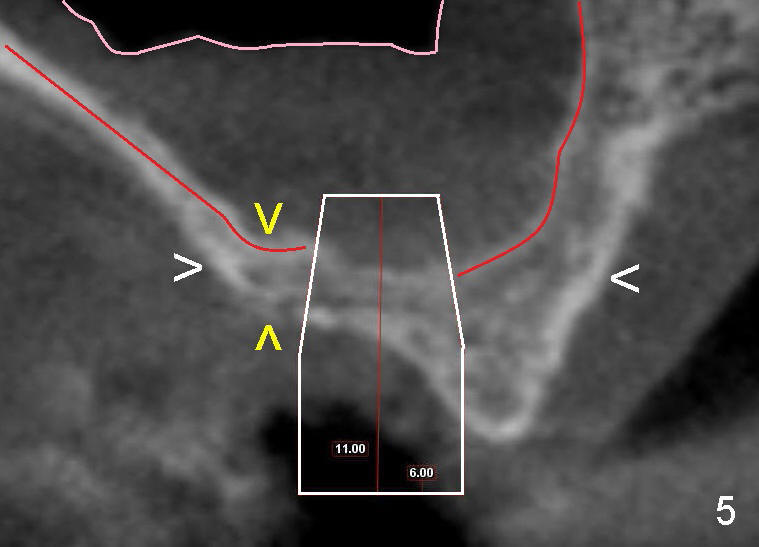
CT coronal section (as shown by Fig.4 black line) shows that the bone of the extraction site is wide (Fig.5 between white >), whereas the height is limited (between yellow >). A wide, but short implant is planned (as shown in Fig.5 white box: 6x11 mm). The apical end of the implant is protruded into the sinus, but probably within the sinus membrane (soft tissue, between pink and red outlines).
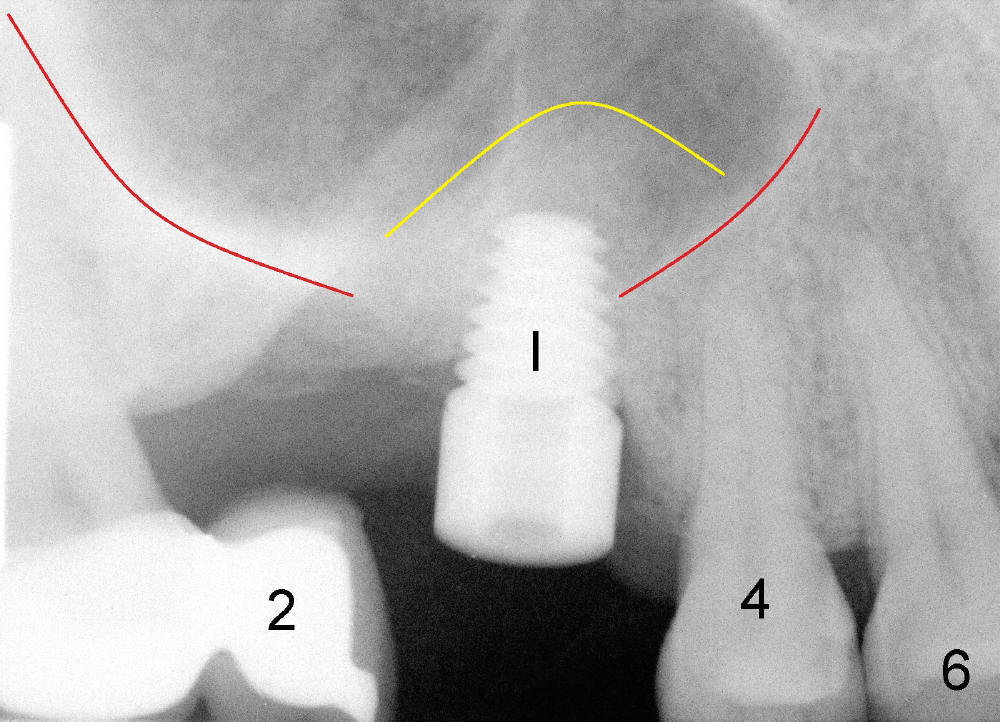
One month after extraction, a tapered implant is placed (Fig.6: I, 6x11). In fact with proper bone manipulation (sinus lift), bone is pushed into the sinus space with the implant (yellow outline as compared to original sinus floor (red outline)).
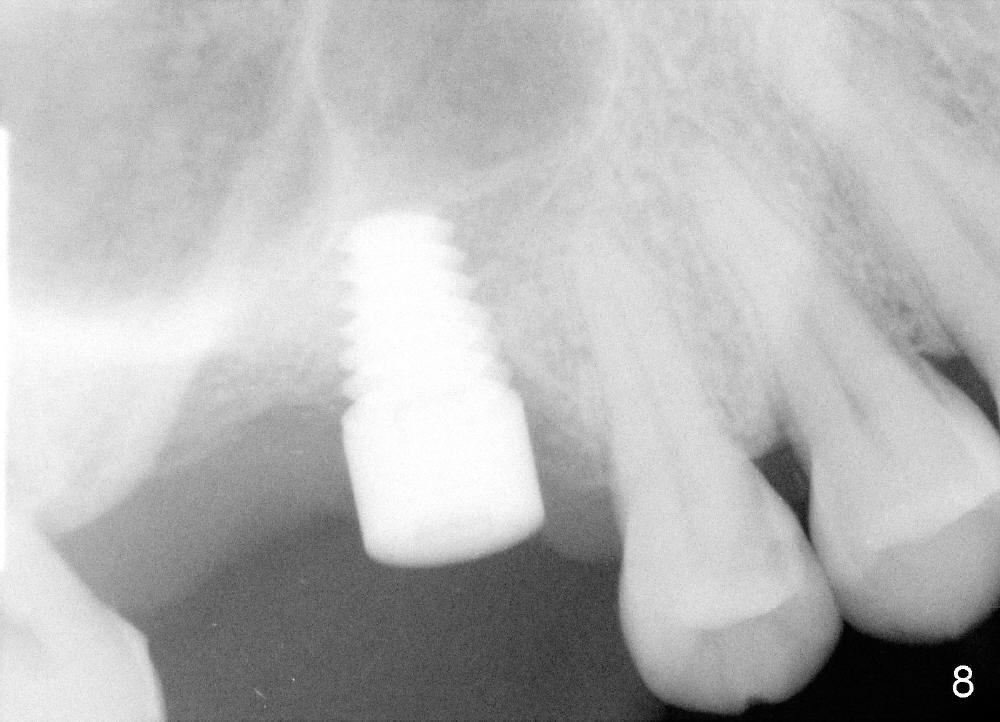
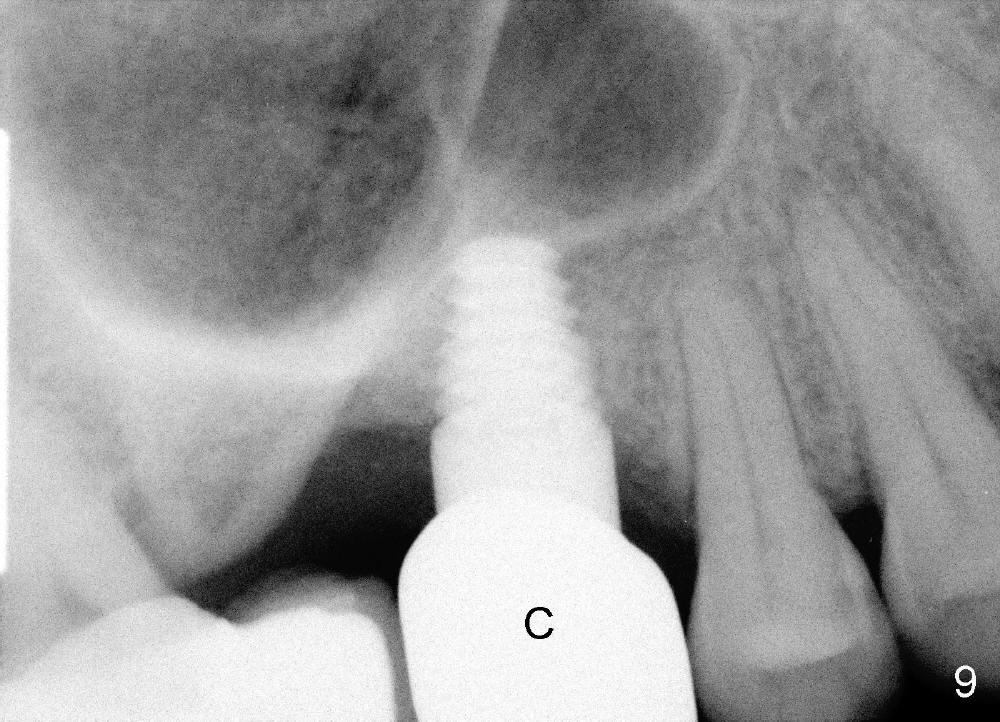
There is no nasal bleeding either after extraction or implant placement. Three and half months post-implantation, the gingiva is healthy around the implant (Fig.7 I). The implant is stable clinically and osteointegrates (Fig.8). Fig.9 appears to show bone growth around the implant 6 months post-cementation.
Since the gingiva heals smoothly after extraction of the affected tooth, precaution of not placing immediate implant is not so necessary.
Hard and Soft Tissue Defects, Introduction to Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 02/24/2013, last revision 12/29/2013