





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
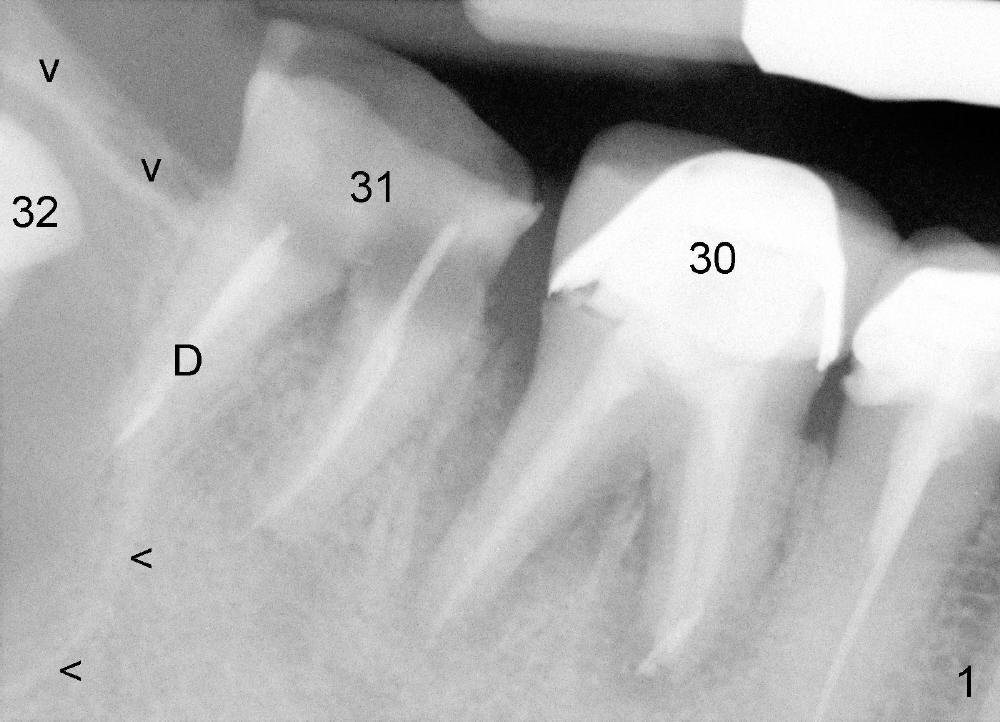
Immediate Implant Next to Dentigerous Cyst
A 47-year-old man requests restoring the tooth #31 (Fig.1). It appears
that the best option is an implant. A close look reveals a possible cyst
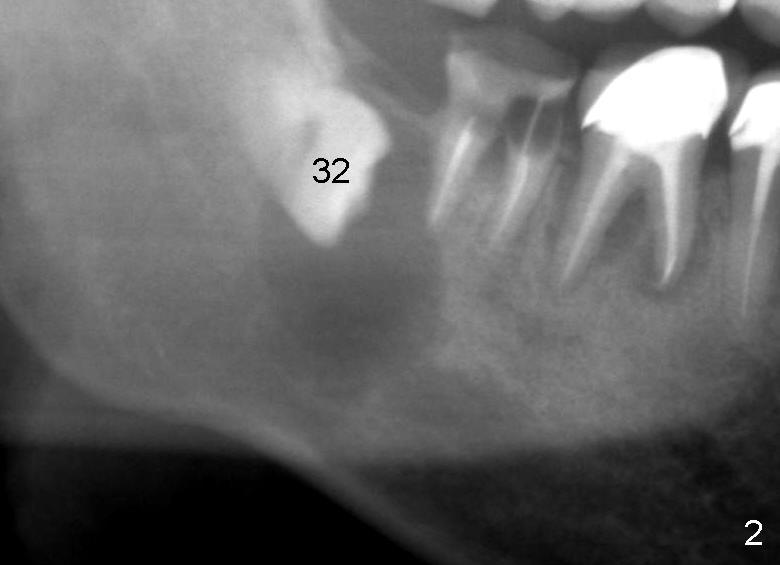
(arrowheads) associated with #32. On the day of surgery, a panoramic X-ray
is taken (Fig.2). The cyst is to be enucleated while an immediate implant
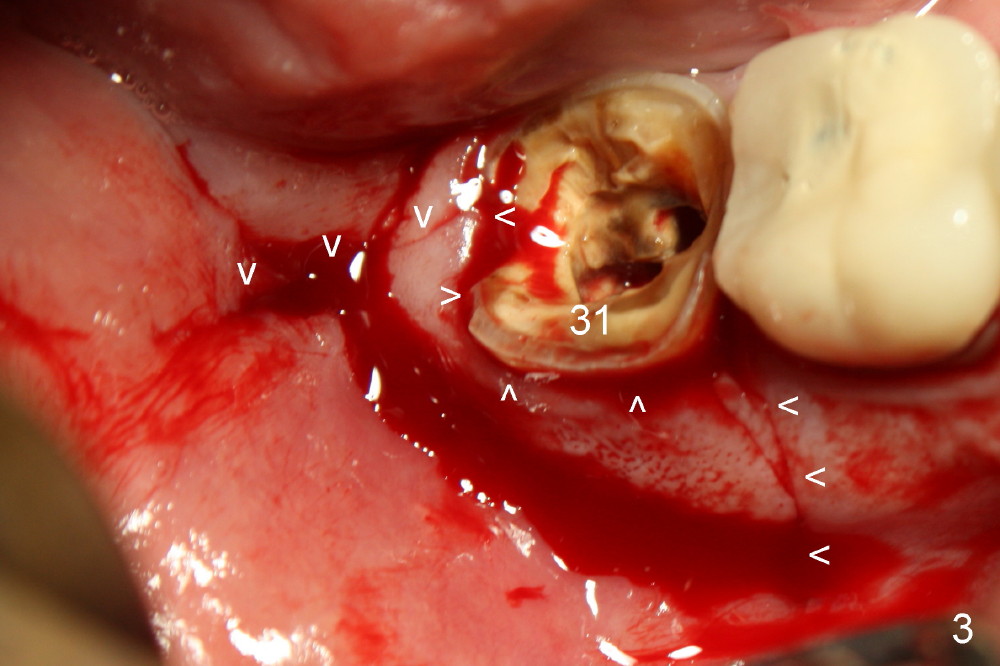
is to be placed in the mesial socket of #31. An incision is made as
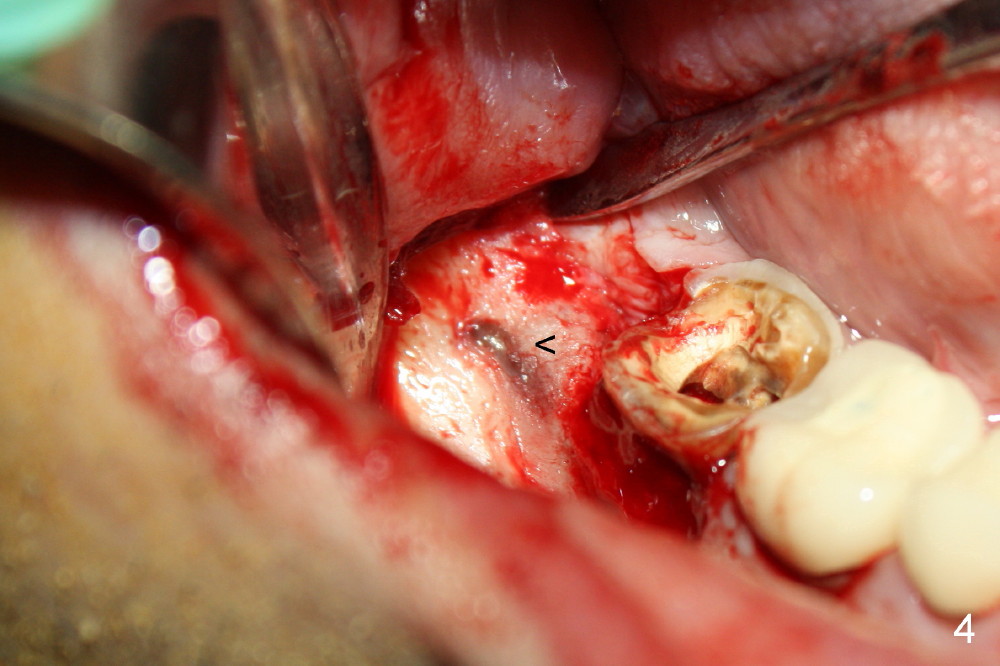
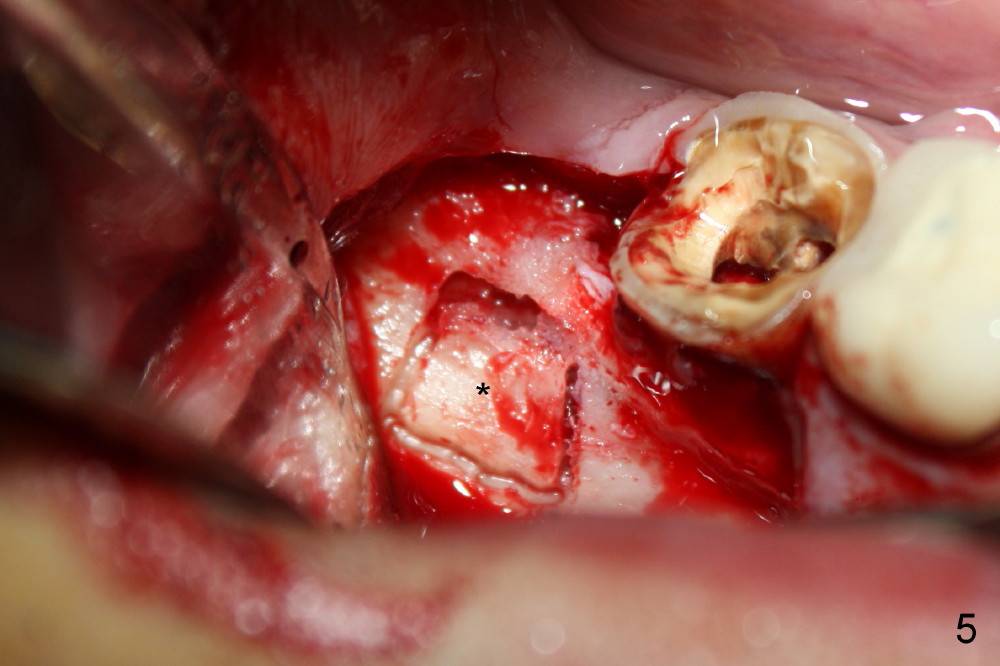
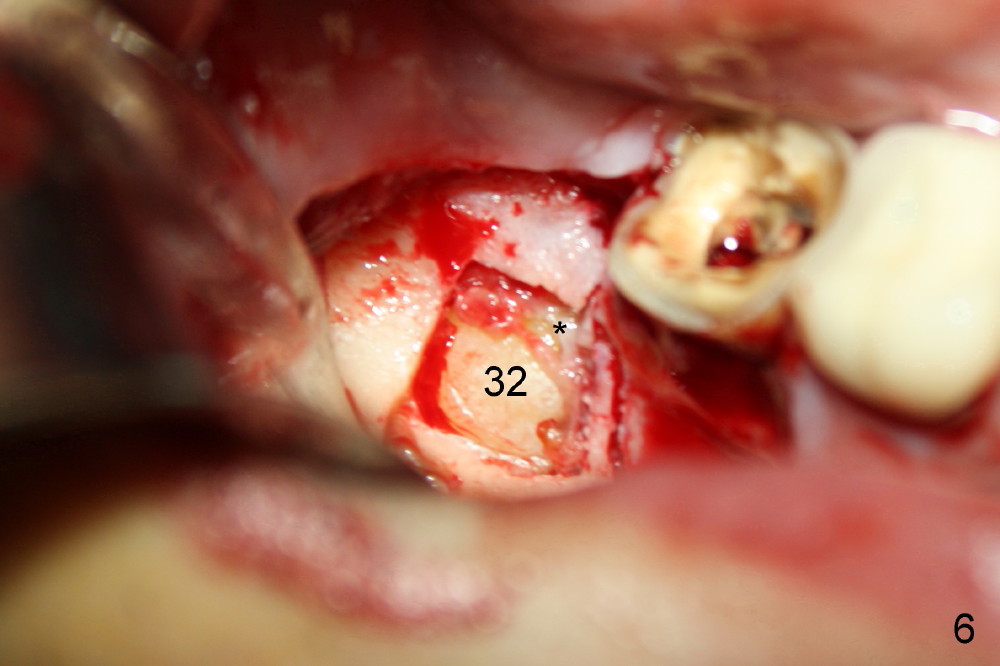
indicated by Fig.3 arrowheads. The bone is resorbed on the top of the cyst
(Fig.4<). A bony window is made (Fig.5*) to expose the impacted tooth of
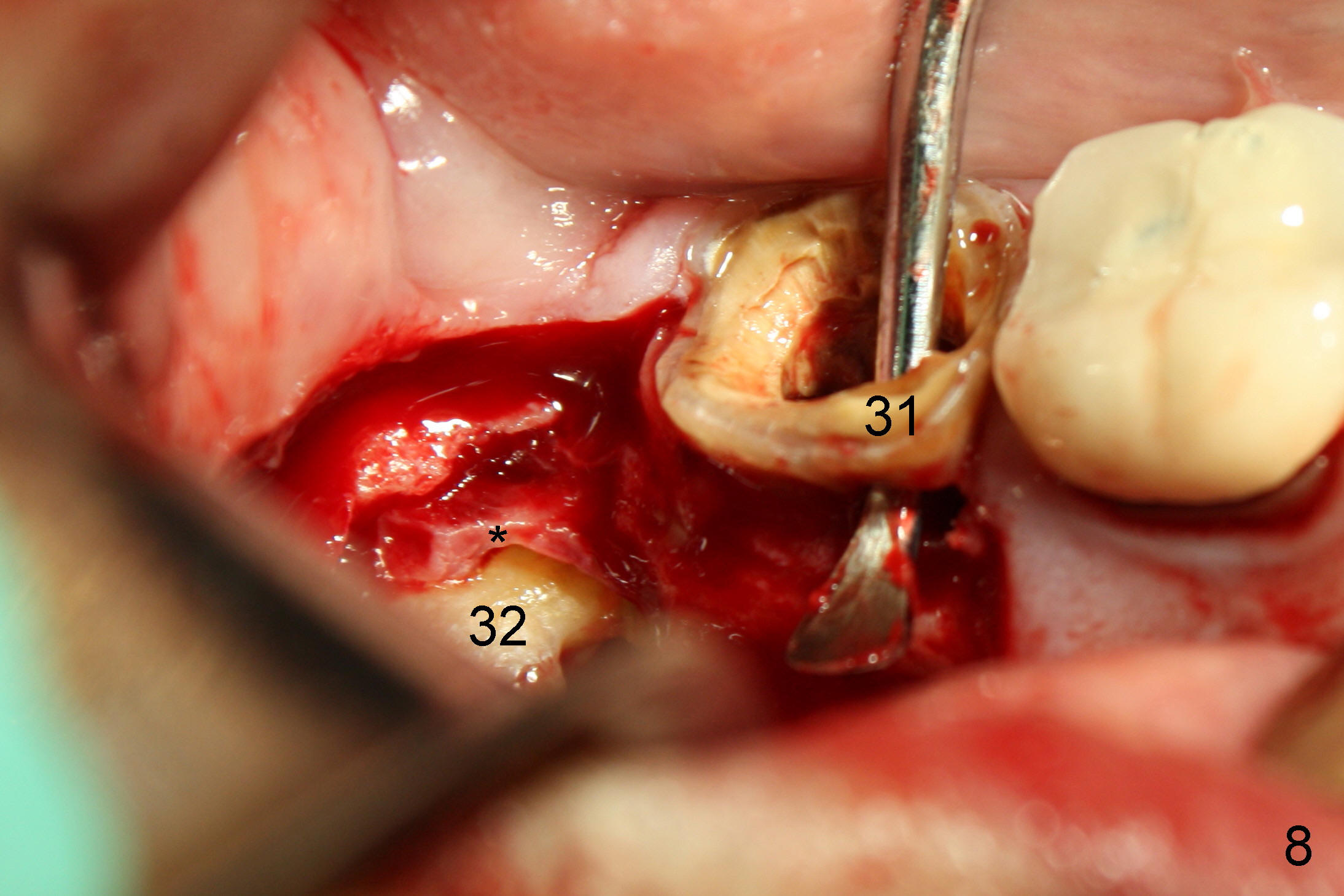
#32 (Fig.6). The latter is sectioned for easy removal (Fig.7 arrowhead);
there is yellowish exudate from the cyst (*). Nonsalvageability of #31 is
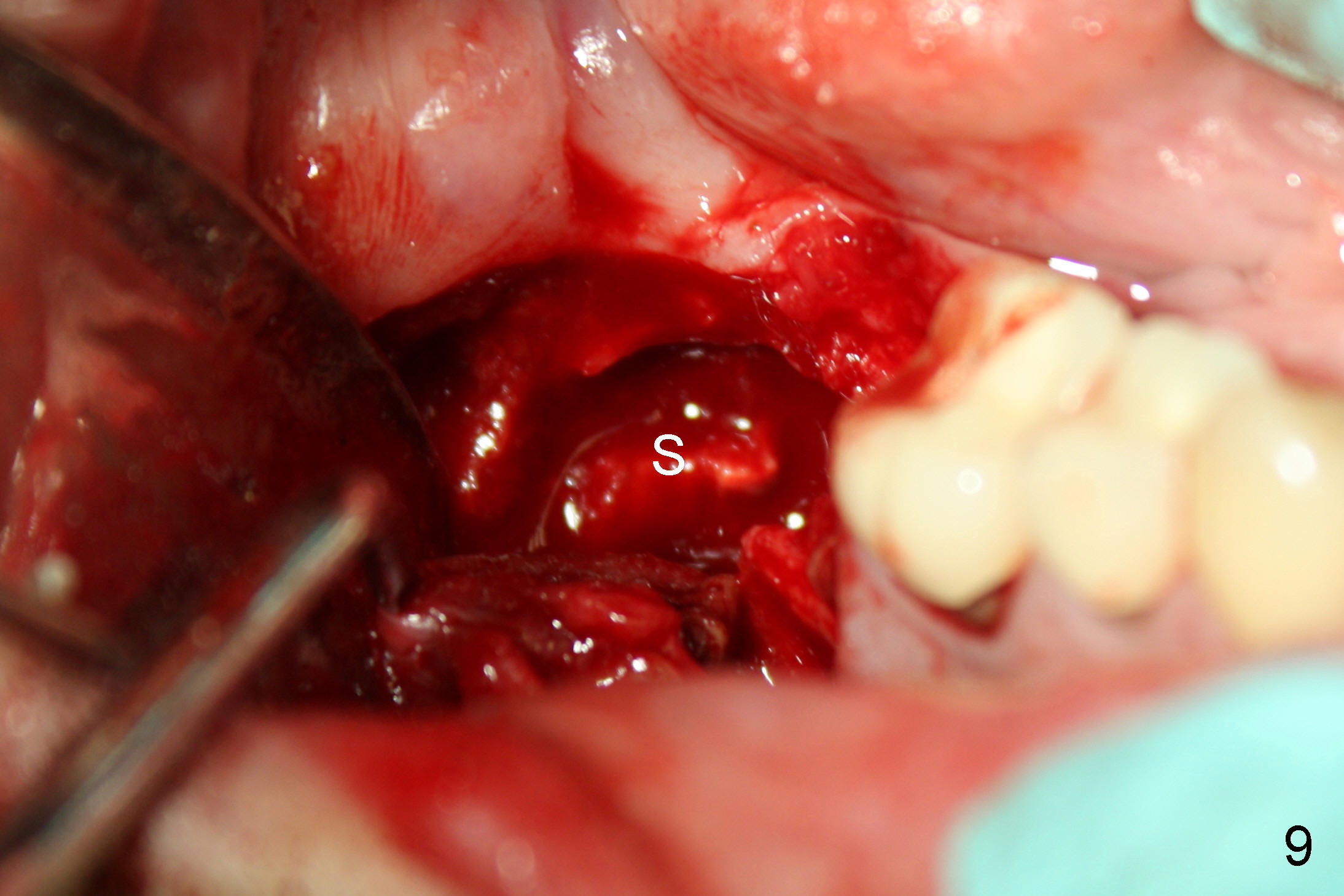
confirmed (Fig.8). Extraction of #31 shows the septum (Fig.9).
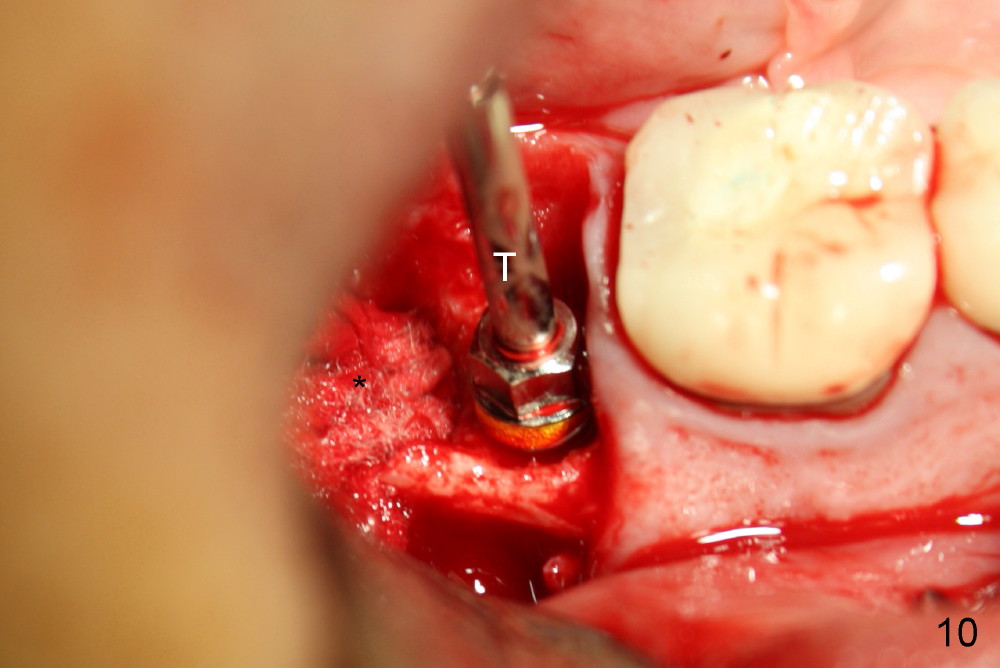
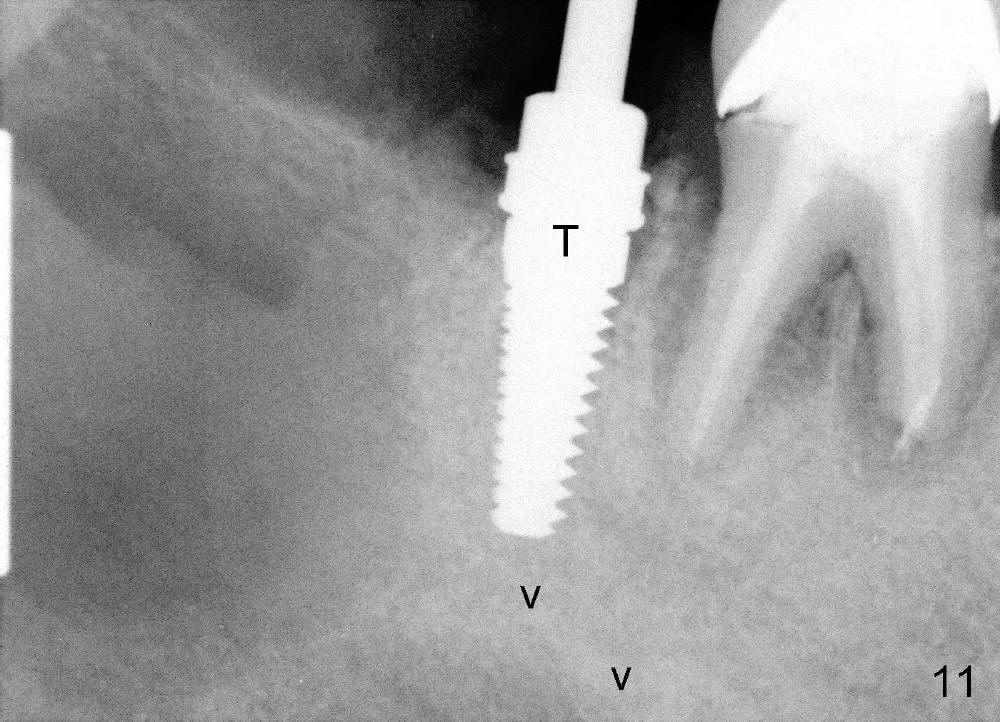
Then the
cyst is removed; hemorrhage is being controlled by gauze (Fig.10 *), while the
osteotomy is created in the mesial socket of #31 (4.5x17 mm tap in place: T
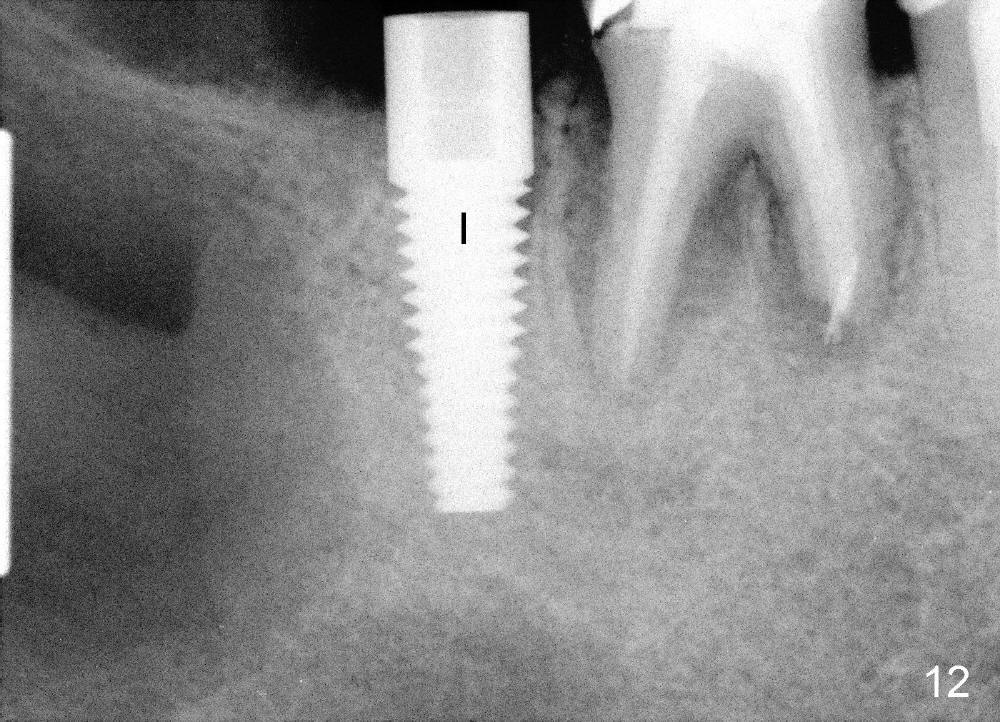
(Fig.10,11)). A 5x17 mm implant is placed with high torque (Fig.12 I).
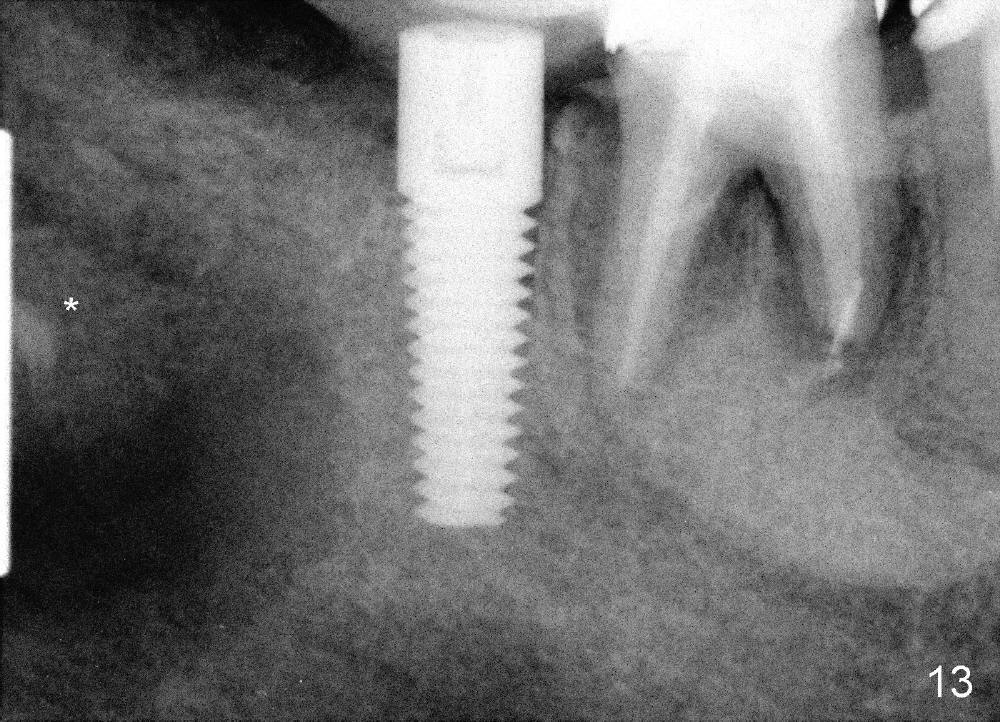
The cystic space is filled by 3 g of allograft (Fig.13 *).
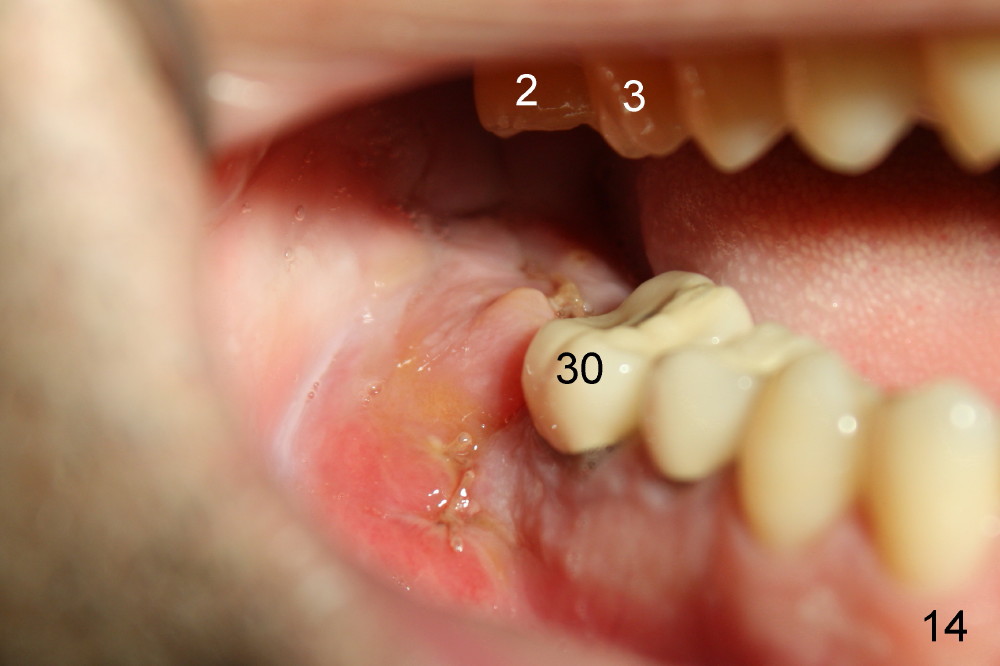
The flap is sutured to cover the gingiva-level implant for hemostasis. Fig.14 shows the wound 7 days postop. The implant is exposed 3 weeks postop (Fig.15).
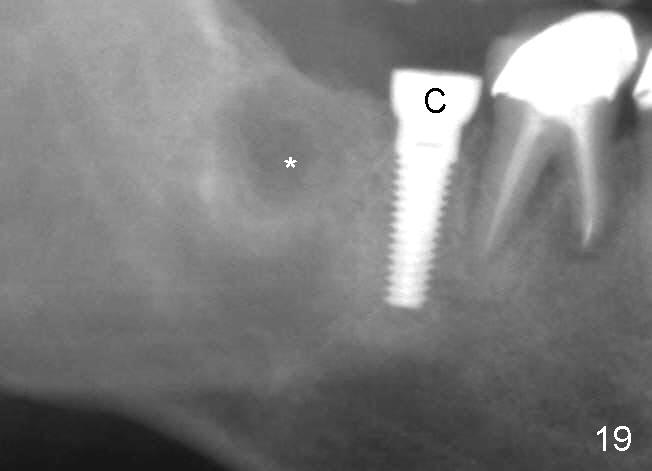
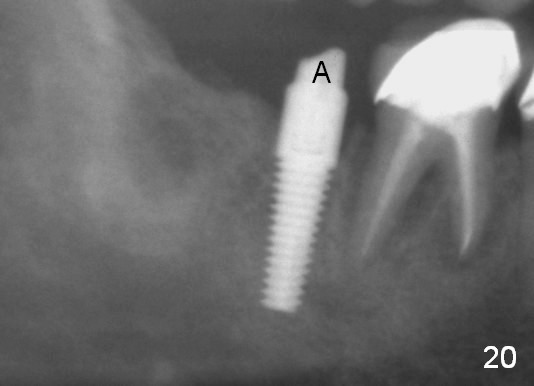
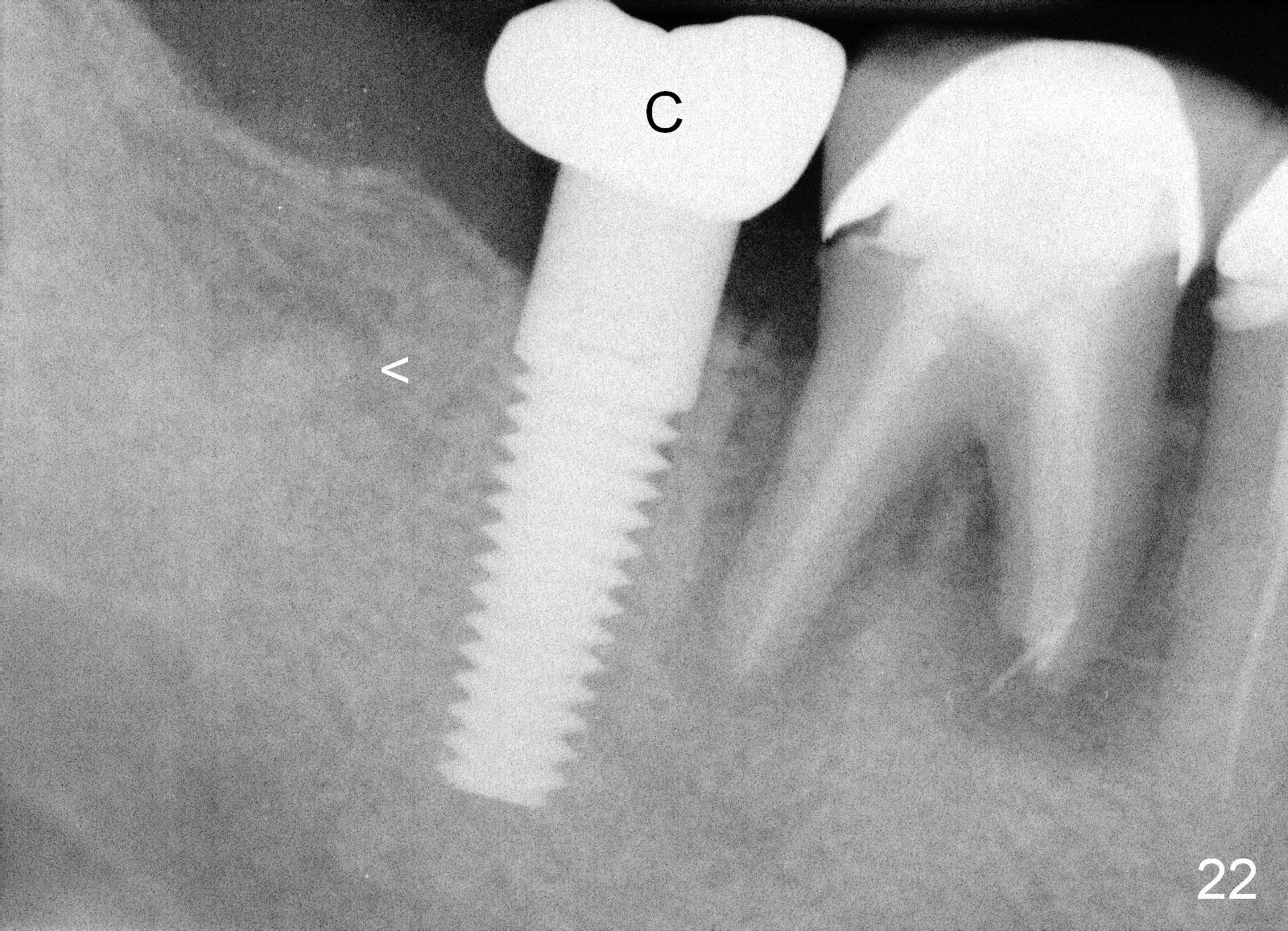
Four months postop, there is a sign of osteointegration (Fig.16 <). Graft particles migrate to the surface of the mucosa (Fig.17 <). A healing cuff is placed over the implant for preparation of restoration (Fig.18 H); graft particles are removed (<). Due to insurance issue, the restoration is yet to finish by 6 months postop (Fig.19 C: healing cuff); the cystic lesion appears to have been decreased concentrically (*). The bone density in the former cyst area continues to increase 14 and 32 months postop (Fig.20 A: abutment; Fig.22). Small piece of bone graft (<) is being extruded distobuccal to the #31 crown (C) asymptomatically 15 and 32 months postop (Fig.21,22).
Xin Wei, DDS, PhD, MS 1st edition 01/07/2014, last revision 09/18/2017