






|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
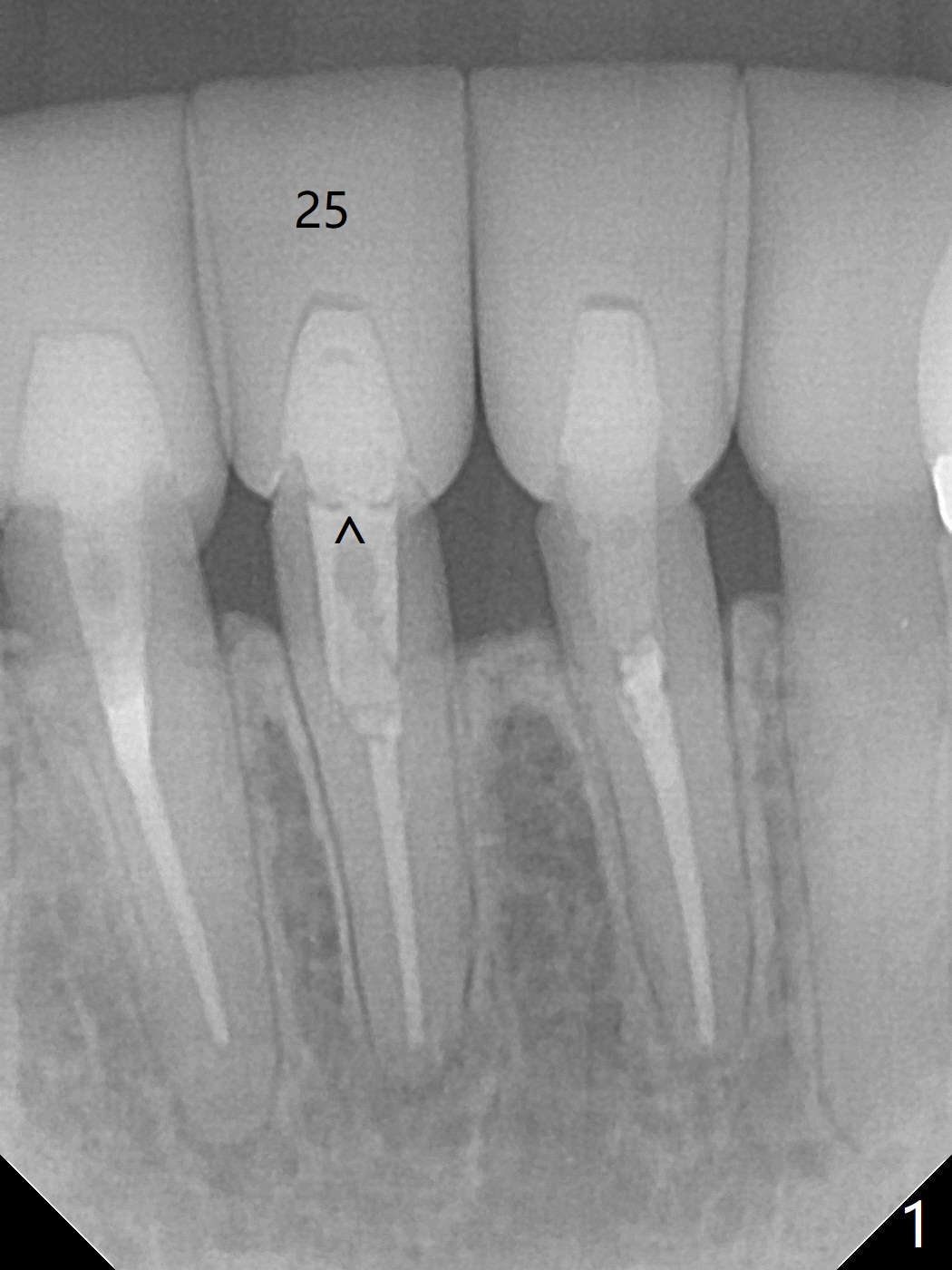
How to Avoid Poor Trajectory?
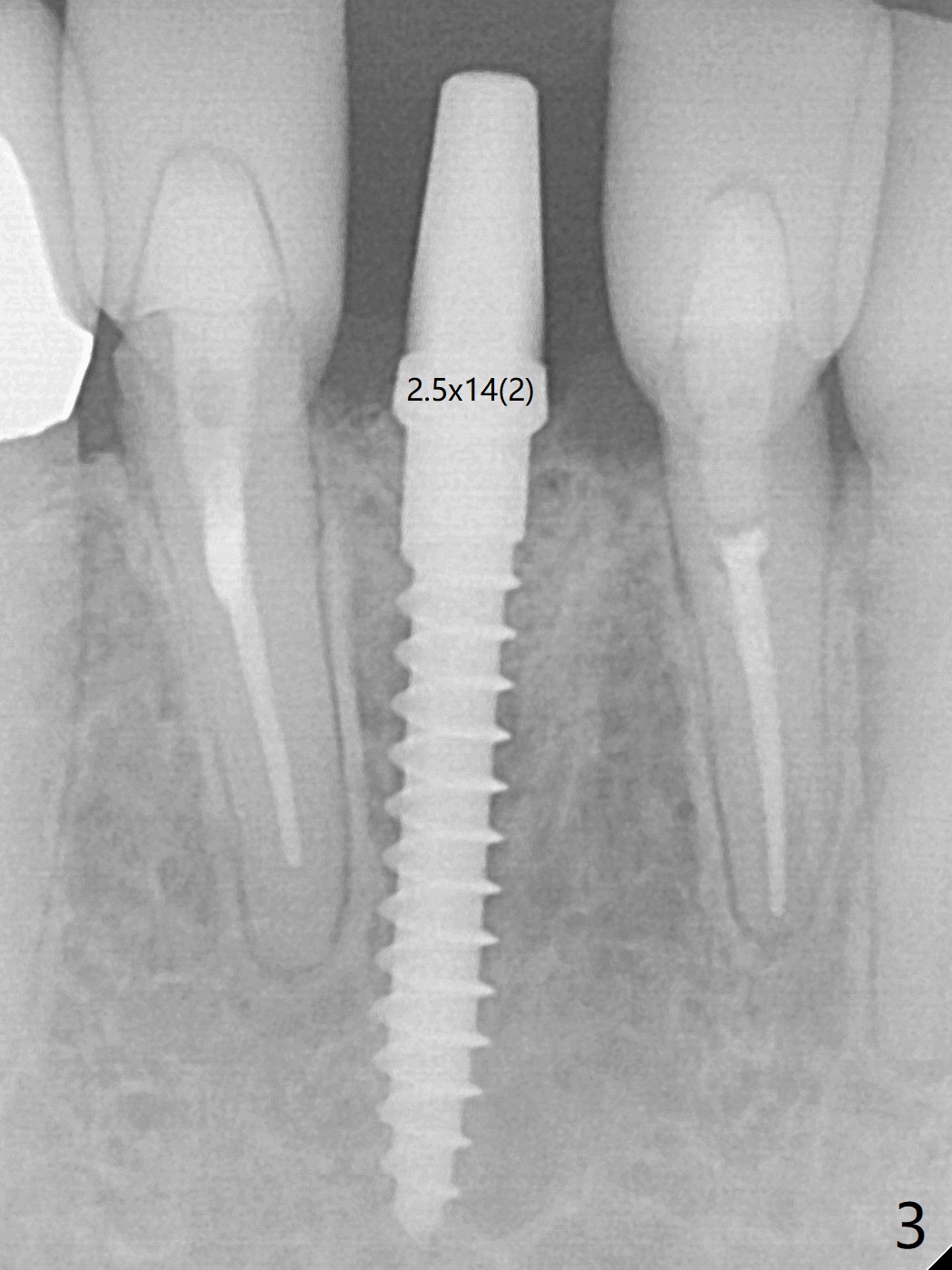
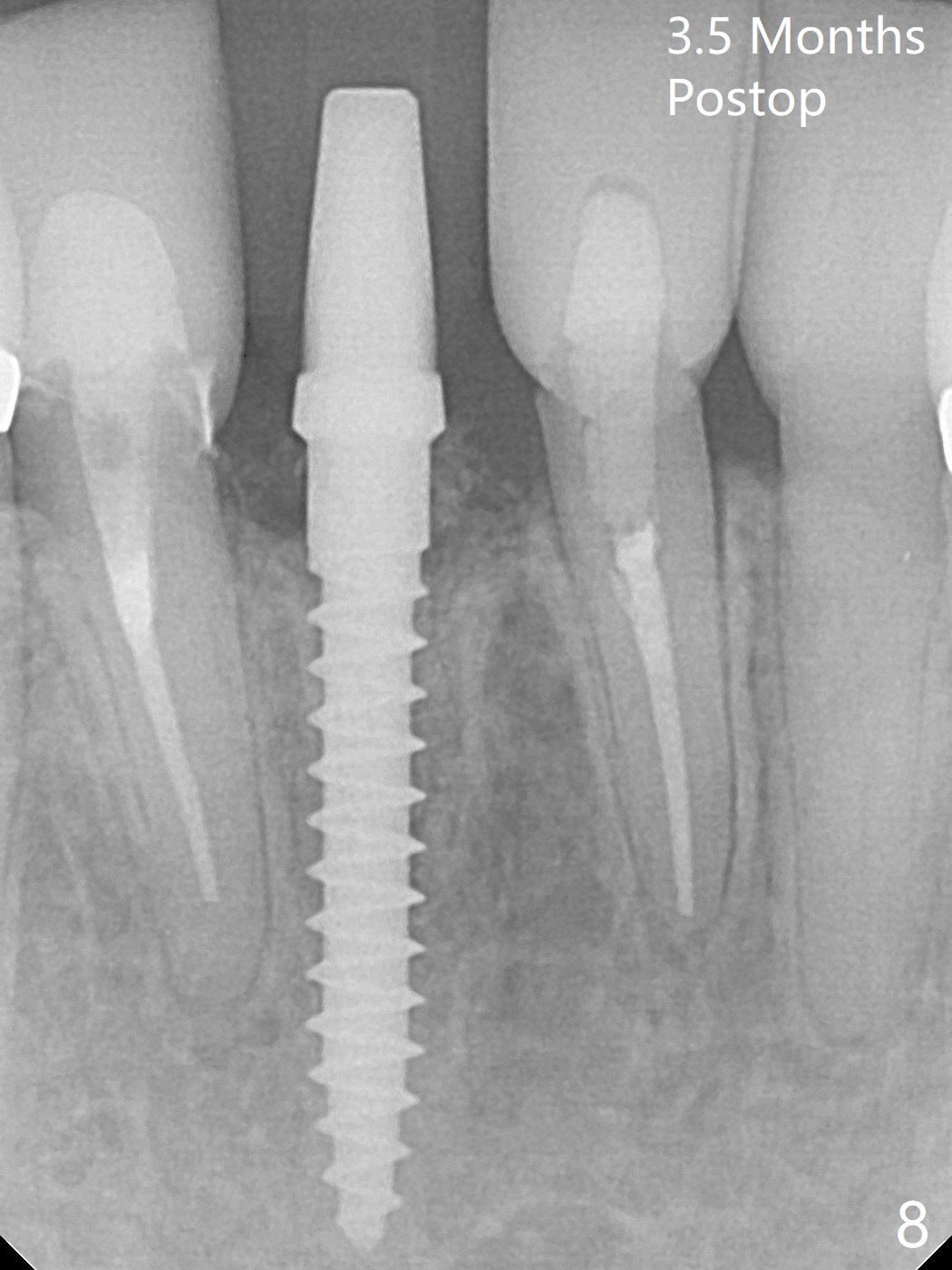
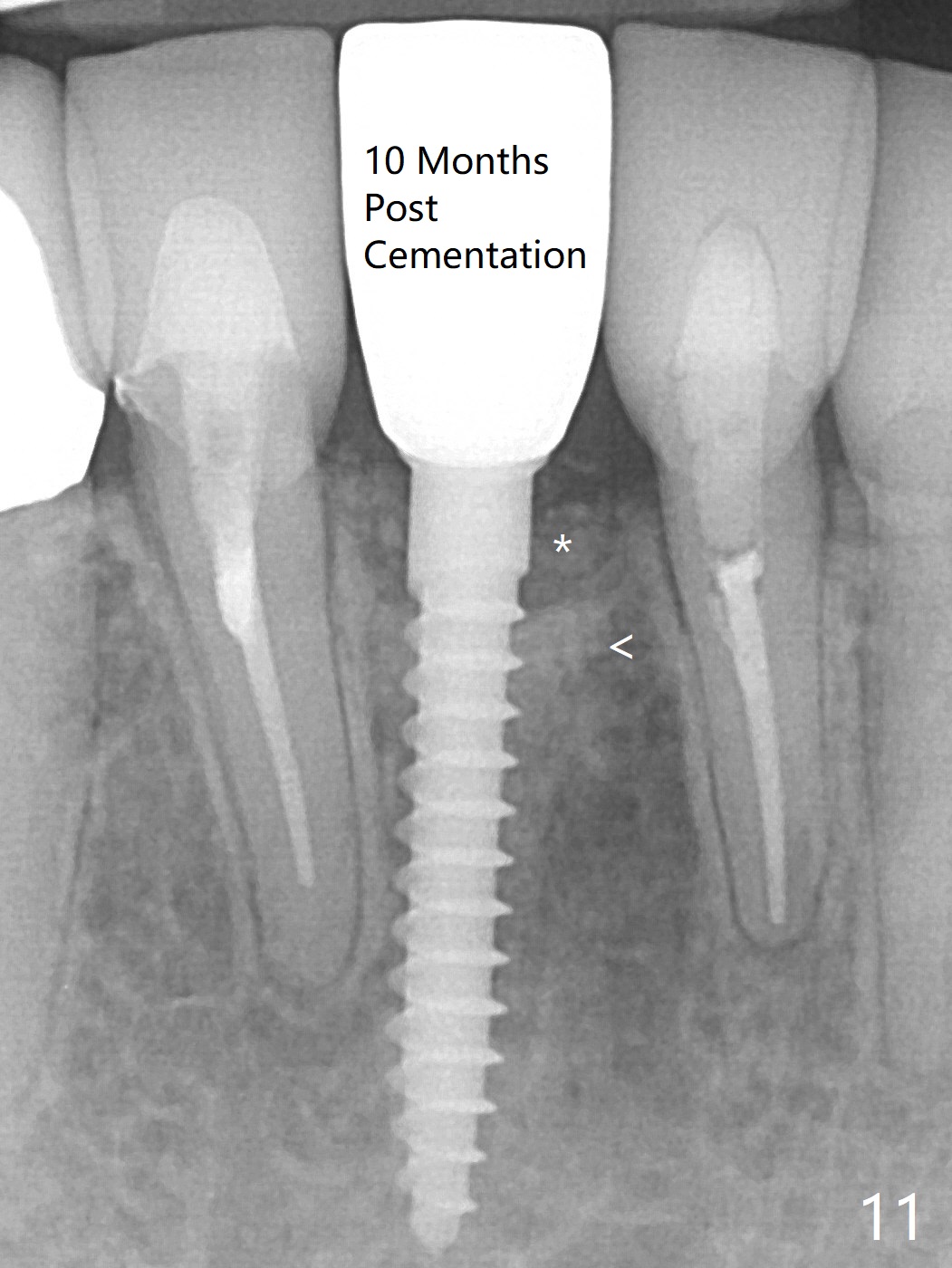
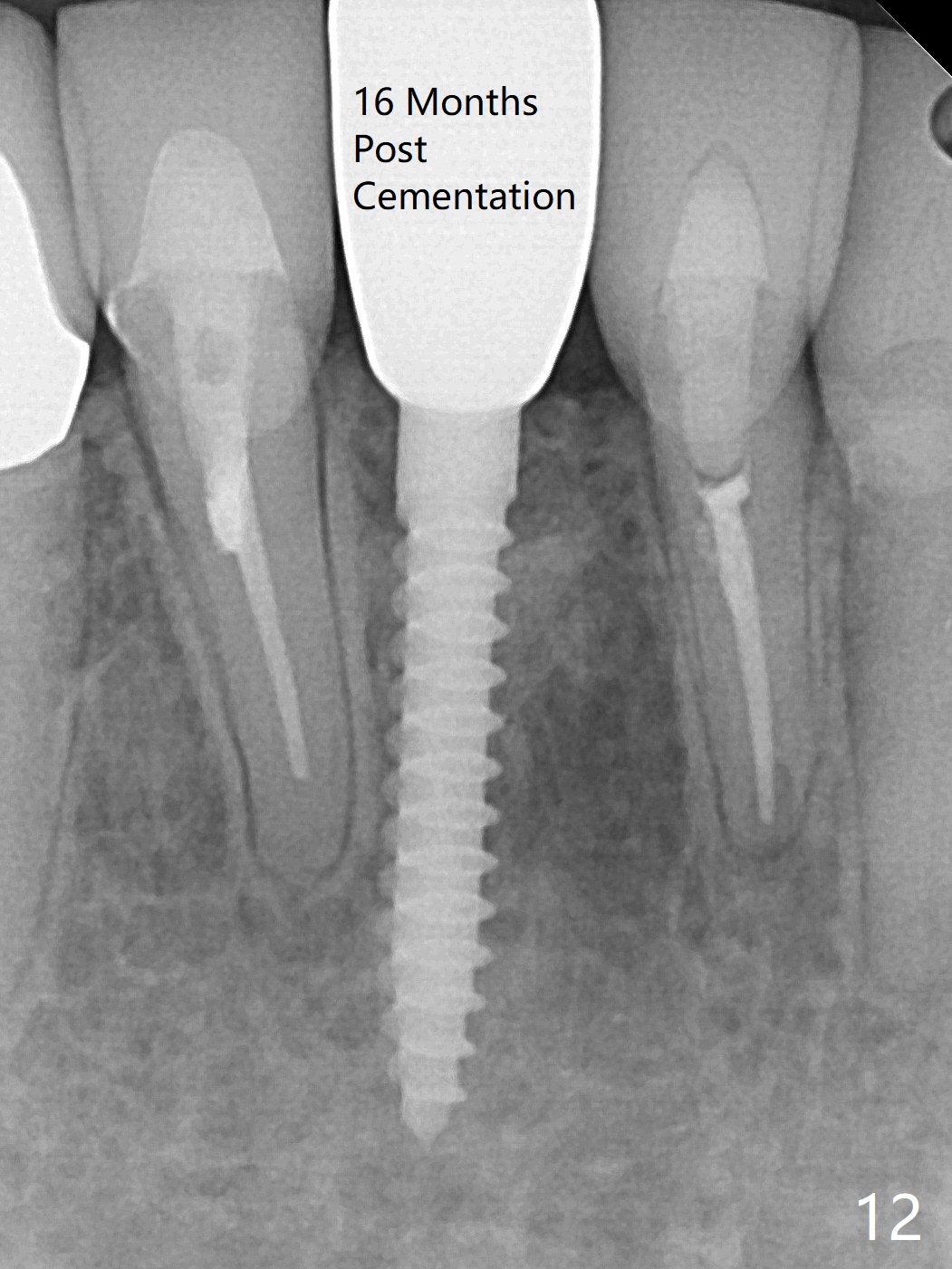
A drawback of implant planning at #25 is not to use a preop PA (Fig.1 (^ fracture line)). The initial trajectory seems to be alright (Fig.2), but a 2.5x14(2) mm implant placed is close to the tooth #26 (Fig.3). In fact the affected tooth is deviated distal; osteotomy should be initiated in the mesial slope of the socket (Fig.4 red line). The final trajectory appears to be perfect (Fig.5). Furthermore the 1st intraop PA should be analyzed carefully (Fig.6). A new osteotomy should be established mesial or the existing one should be moved mesial with Lindamann bur (Fig.7). The distal implant placement may be related to more bone loss in the distal crest 3.5 months postop (Fig.8) and more severe distal papillary recession (Fig.9 *). The bone density increases at the levels of the non-thread and thread portions of the implant (in the original socket) nearly 10 months post cementation (Fig.11 *, <). There is no bone loss 16 months post cementation (Fig.12).
Return to Lower Incisor Immediate Implant, Trajectory Xin Wei, DDS, PhD, MS 1st edition 05/29/2019, last revision 01/27/2021