

,%20Vanilla.jpg)






|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
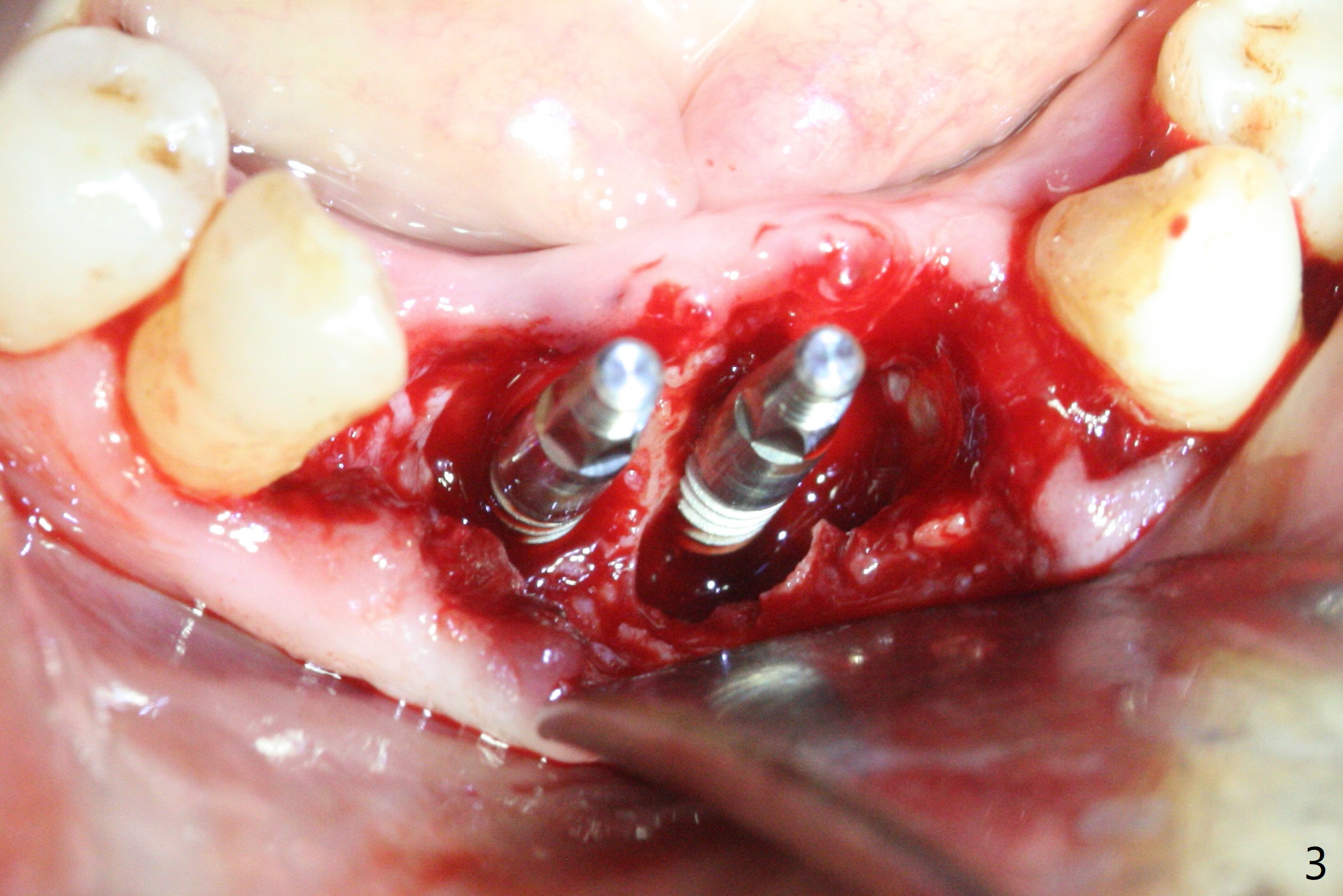
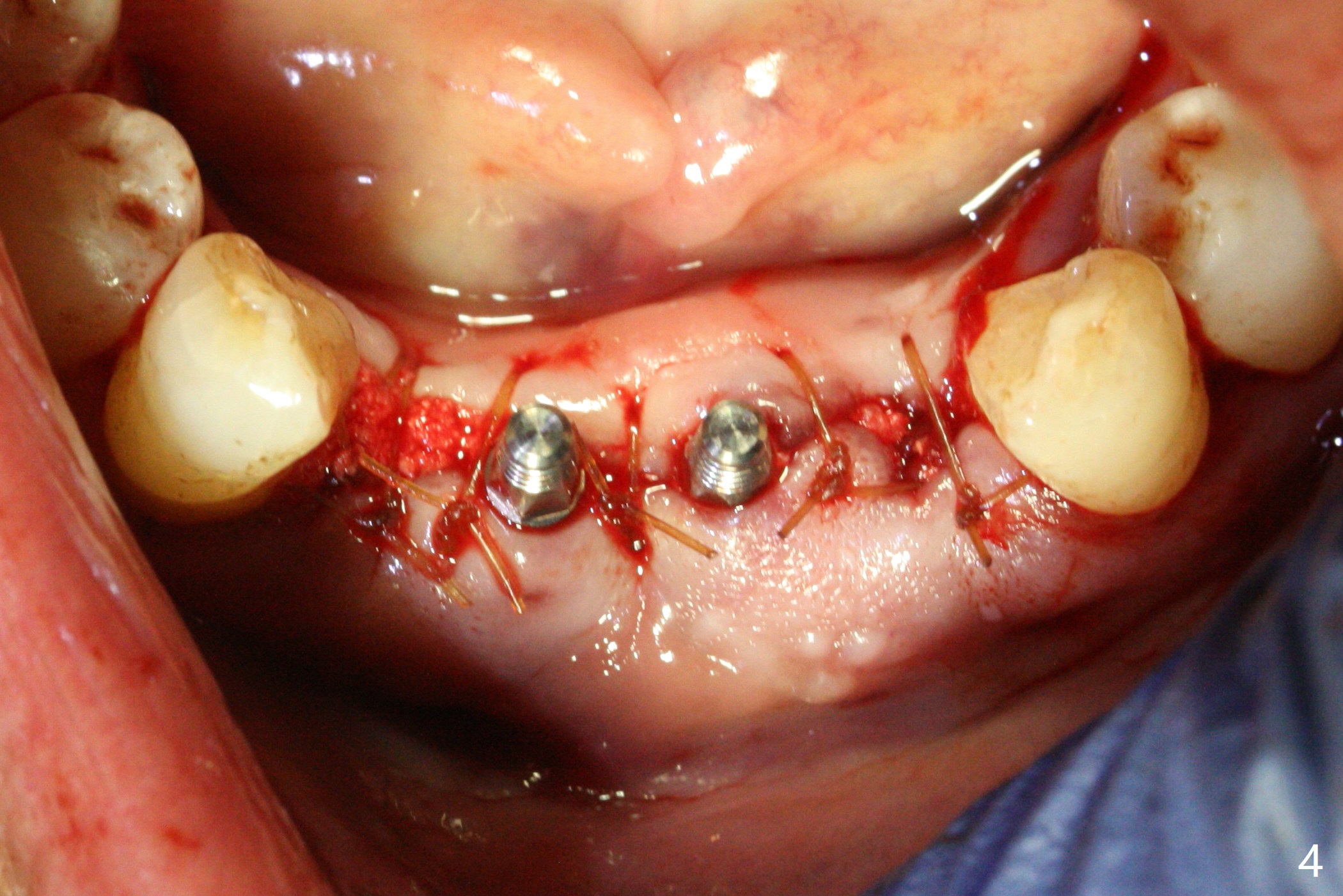
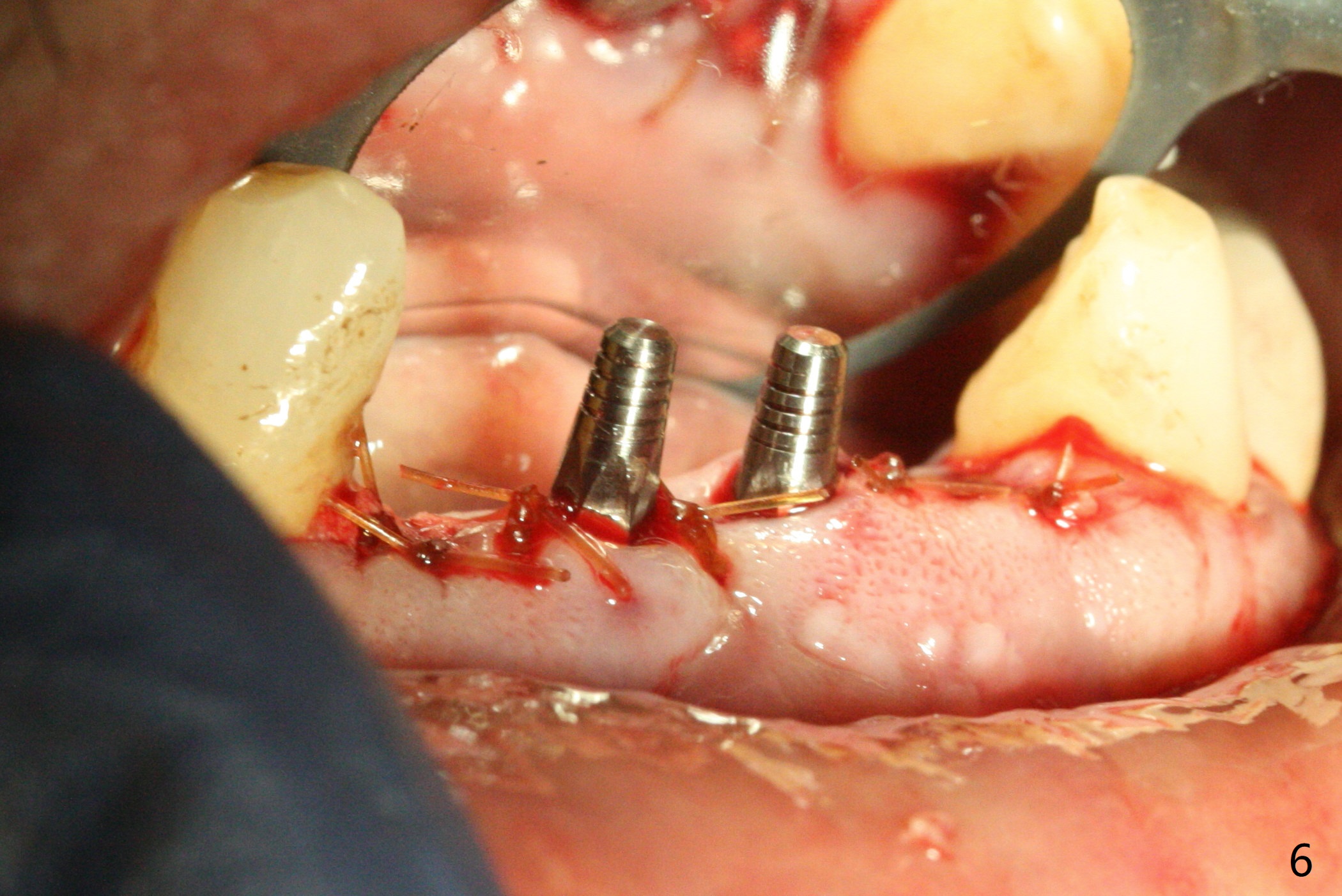
Two 1-Piece Implants for 4 Incisors
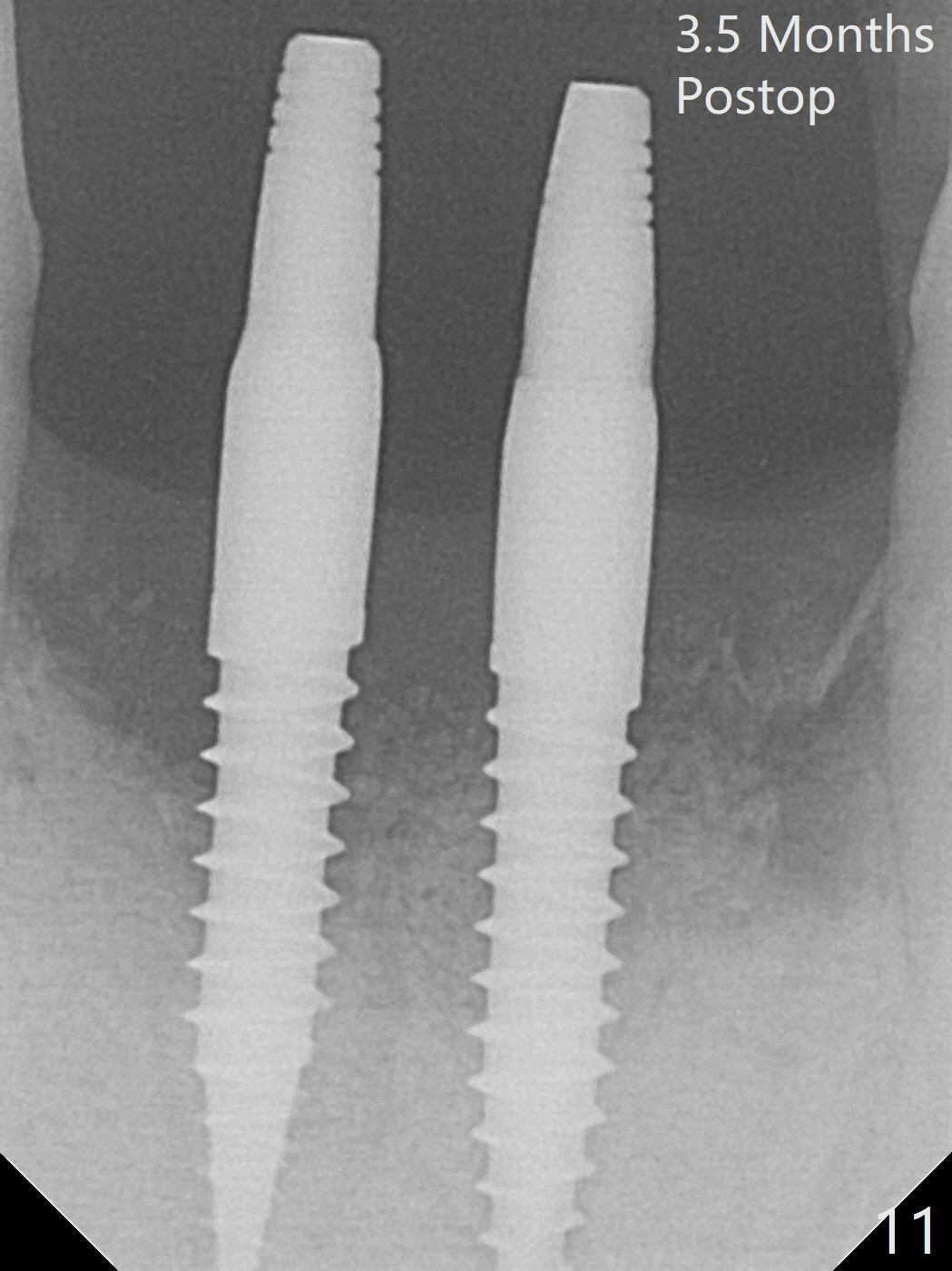
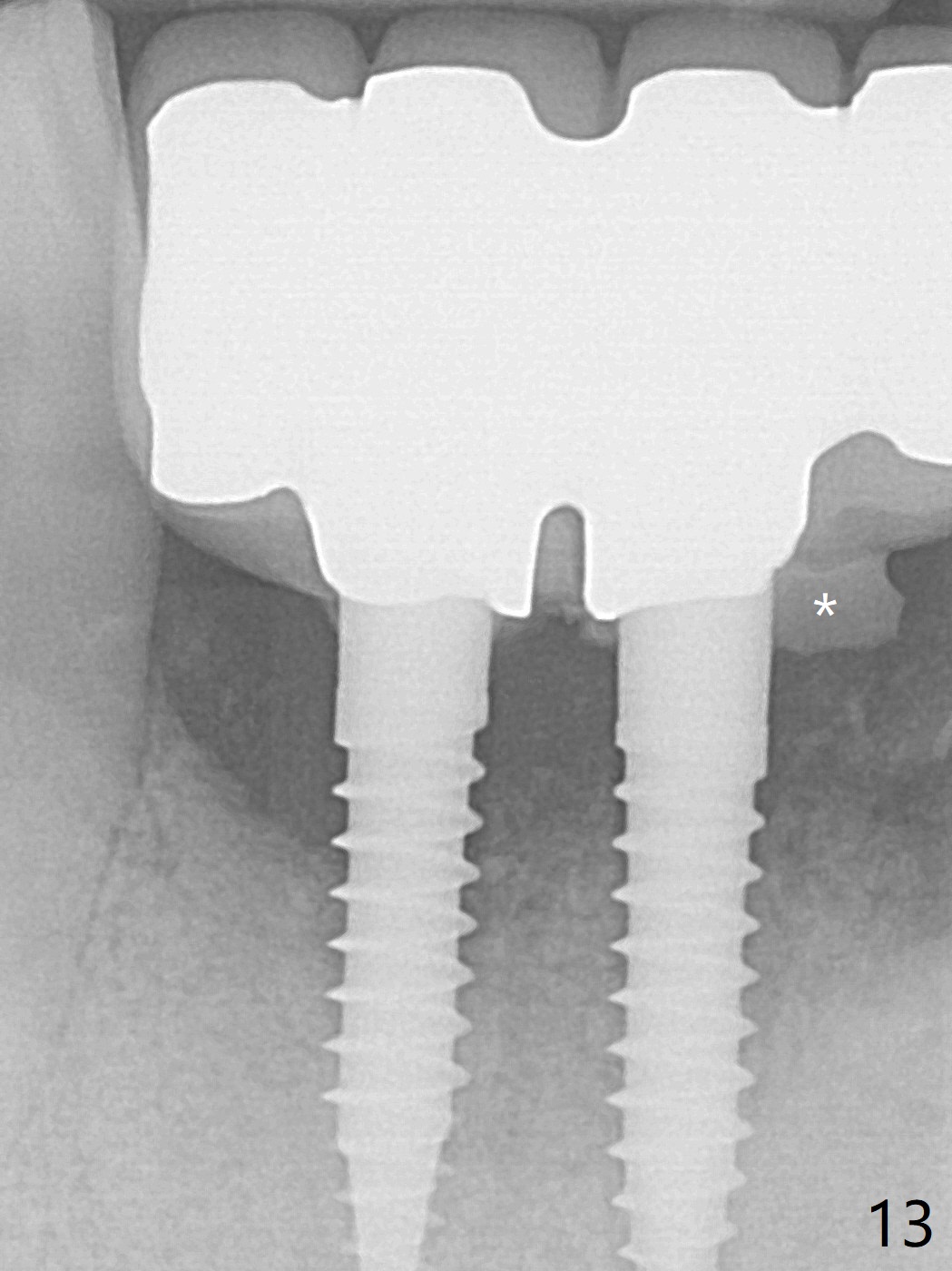
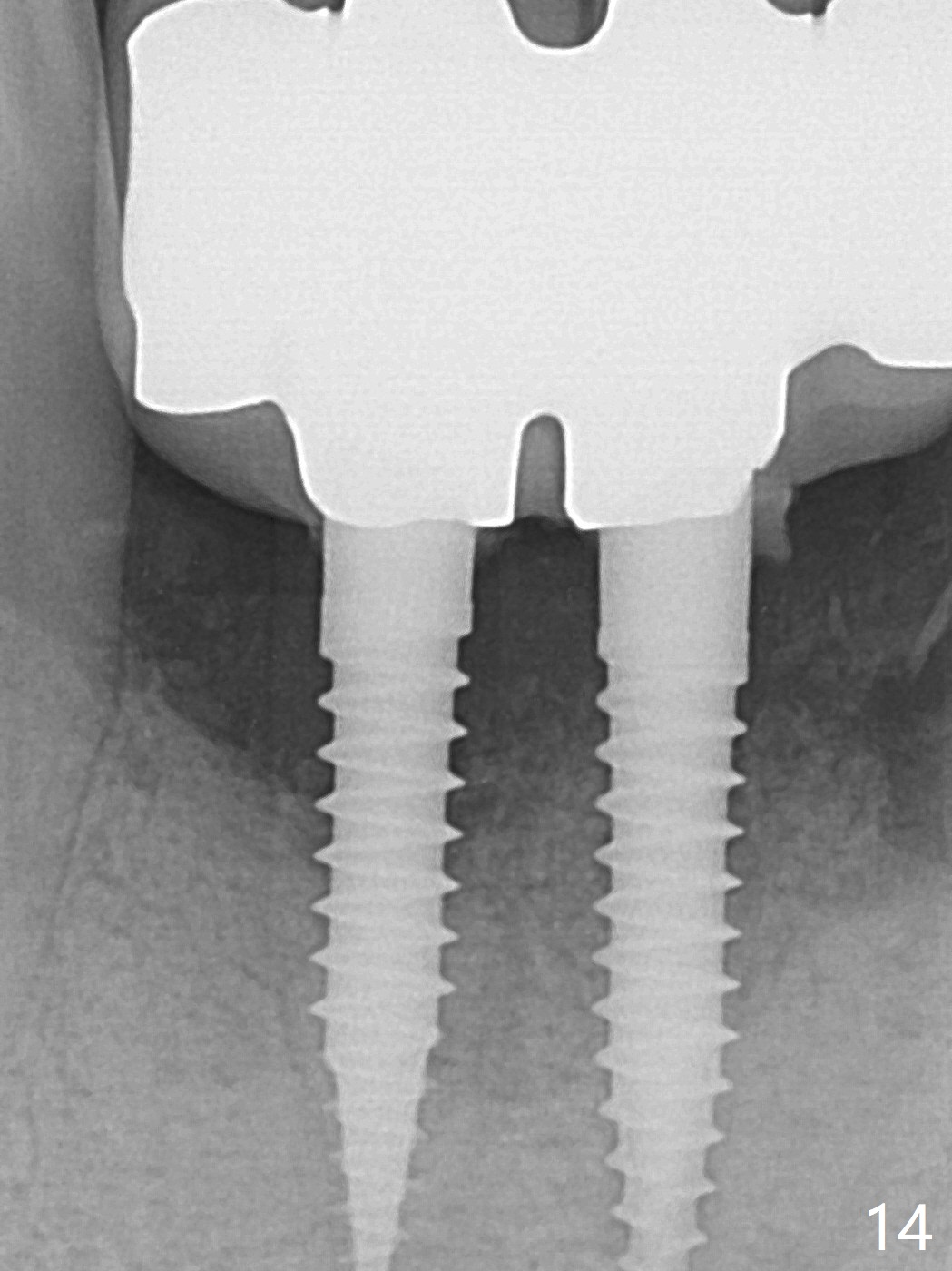
When the patient (smoker) returns for treatment, the apical abscess associated with #25 and 26 reduces with oral Amoxicillin. He agrees with 4 incisor extraction because of 2 apical fistulae (Fig.1 >). Osteotomy starts at the central incisor sockets due to mesial root exposure of the canines (Fig.2 arrowheads) and buccal alveolar bone fracture between #23 and 24 (Fig.7). Two of 3x14(4) mm 1-piece implants are placed with ~ 2 mm buccal gap (Fig.3). After Vanilla graft is placed in the bony defects (Fig.5 *) and Osteogen plug, sutures are placed (Fig.4). The implants are then placed deep to decrease thread exposure (Fig.6). Periodontal dressing is applied instead of provisional. Alveolar bone fracture between #23 and #24 accounts for why an implant is less suitably placed at #24 (Fig.7). Three months postop, composite is added to the pontic areas of the provisional (Fig.8 *). When the provisional is seated, the convex pontics press the used-to-be-flat gingiva (Fig.9 arrows). Thus the concave gingiva forms (Fig.10 *) with corresponding papillae (^). In fact the photos of Fig.8-10 is taken ~3 weeks later. Most of the grafted bone remains in place 3.5 months postop (Fig.11). A piece of floss with 2 knots in one end is placed between the middle units of the final bridge before cementation (Fig.12 (4 months 10 days postop)). In fact removal of residual cement is not so simple. It is tedious (Fig.13,14). An asymptomatic buccal fenetration with implant thread exposure is found 2 months post cementation and persists for another month in spite of advice to reduce smoking (1/2 ppd) and use of water pik (Fig.15). The area will be debrided, followed by bone graft and PRF in a month.
Return to Lower Incisor Immediate Implant, Armaments Xin Wei, DDS, PhD, MS 1st edition 04/10/2018, last revision 01/07/2019