








|
|
|
|
|
||
|
|
|
|
|
|
|
How to Restore Perio-Endo Tooth? M
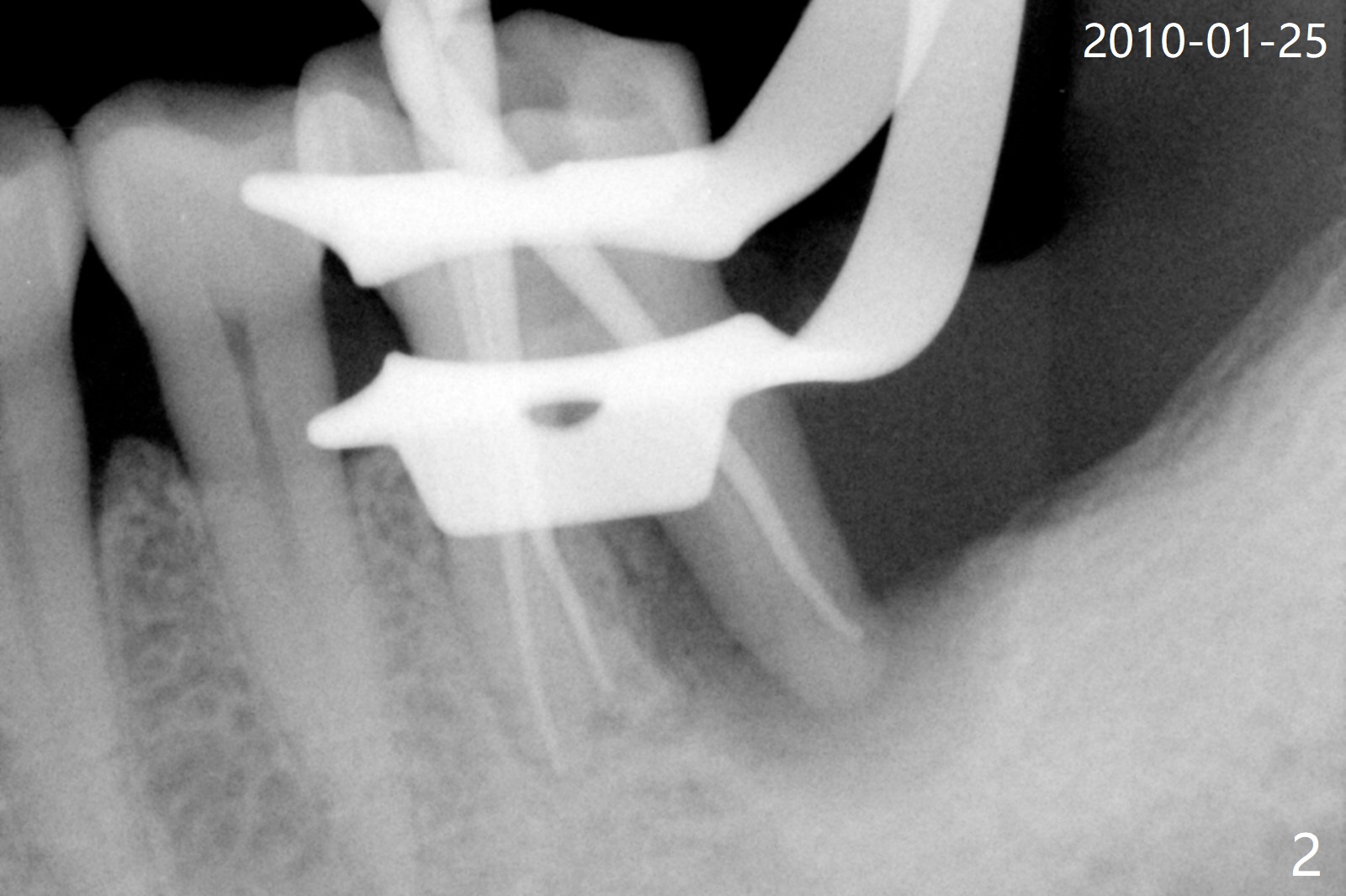
A 56-year-old man had distal gingival erythema at #19 with a fistula (Fig.1). Upon opening the pulpal chamber, the pulp is vital in the mesial canals, while necrotic distal. Root canal therapy is finished 1.5 months later (Fig.2). Although the patient was pleased with the treatment, the gingival infection and fistula did not improve. The tooth mobility increases over the years (Fig.3). He will return for evaluation next Monday. What should be done?
After tooth extraction (Fig.4), a medium-sized implant (4.5 mm, Fig.5 green) will be placed in the mesial socket, but the coronal end of the long axis of the implant (white line) will be in the middle of the socket for future restoration. The gingival margin of the socket is also uneven (Fig.6 pink). Before placement of the final abutment (Fig.7 blue), pack allograft (red circles) over the exposed implant surface until the platform of the implant. After placement of Osteogen plug in the distal socket (Fig.8 yellow), more of allograft is placed coronally. An immediate provisional (Fig.9 white) is to be fabricated to keep the graft in place. If the socket is deemed to be unsuitable for immediate implant, place PRF membrane(s) distoocclusally (Fig.10 purple), followed by collagen membrane and suturing.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Trajectory, Clindamycin Metronidazole No Antibiotic, Weichat
Xin Wei, DDS, PhD, MS 1st edition 01/12/2019, last revision 12/26/2019