
,%20more%20allograft.jpg)


,%20retightened%20abutment,%20crown,%20not%20fit.jpg)
%20abutment,%20fit.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
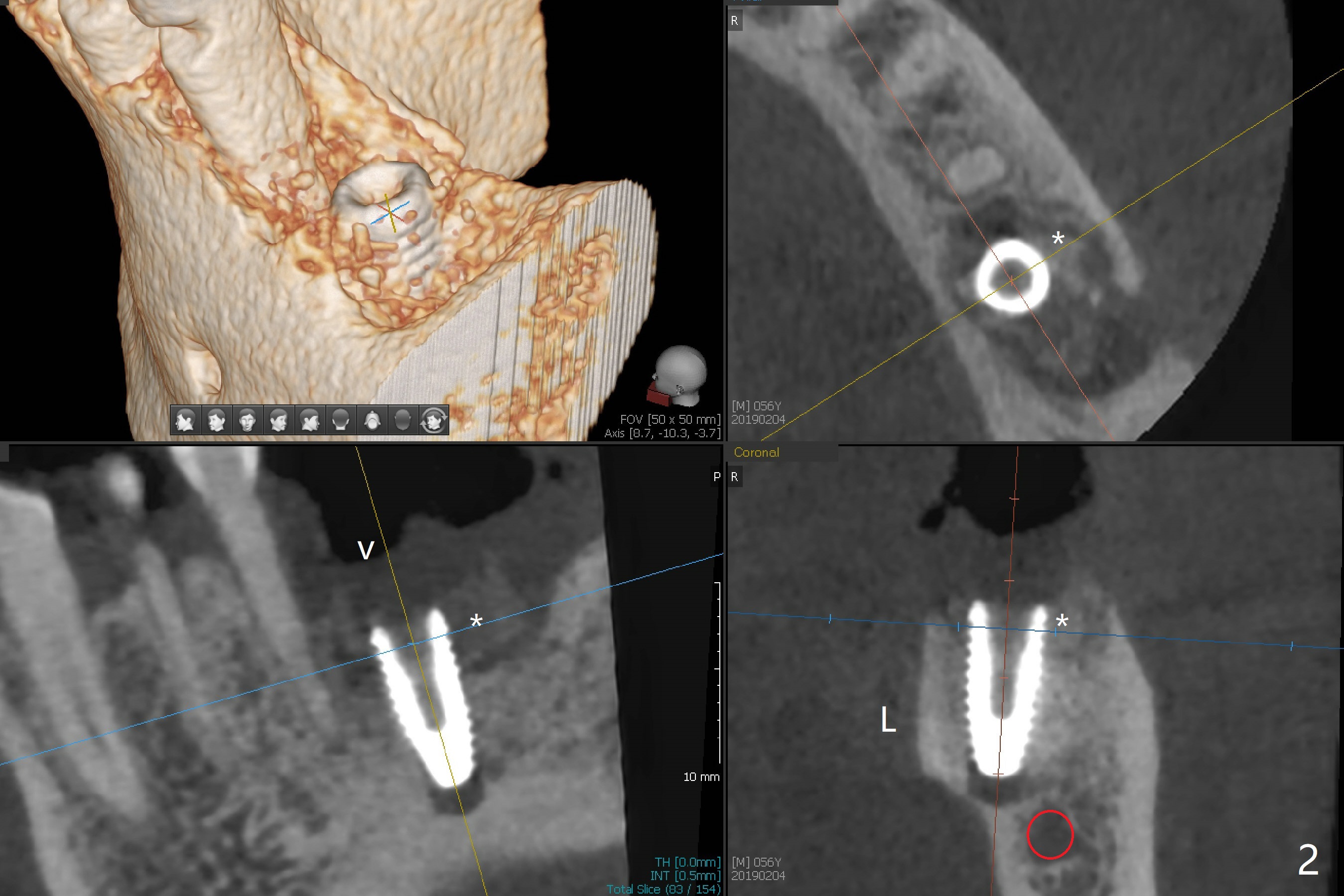
Smaller Implant/More Bone Graft
M
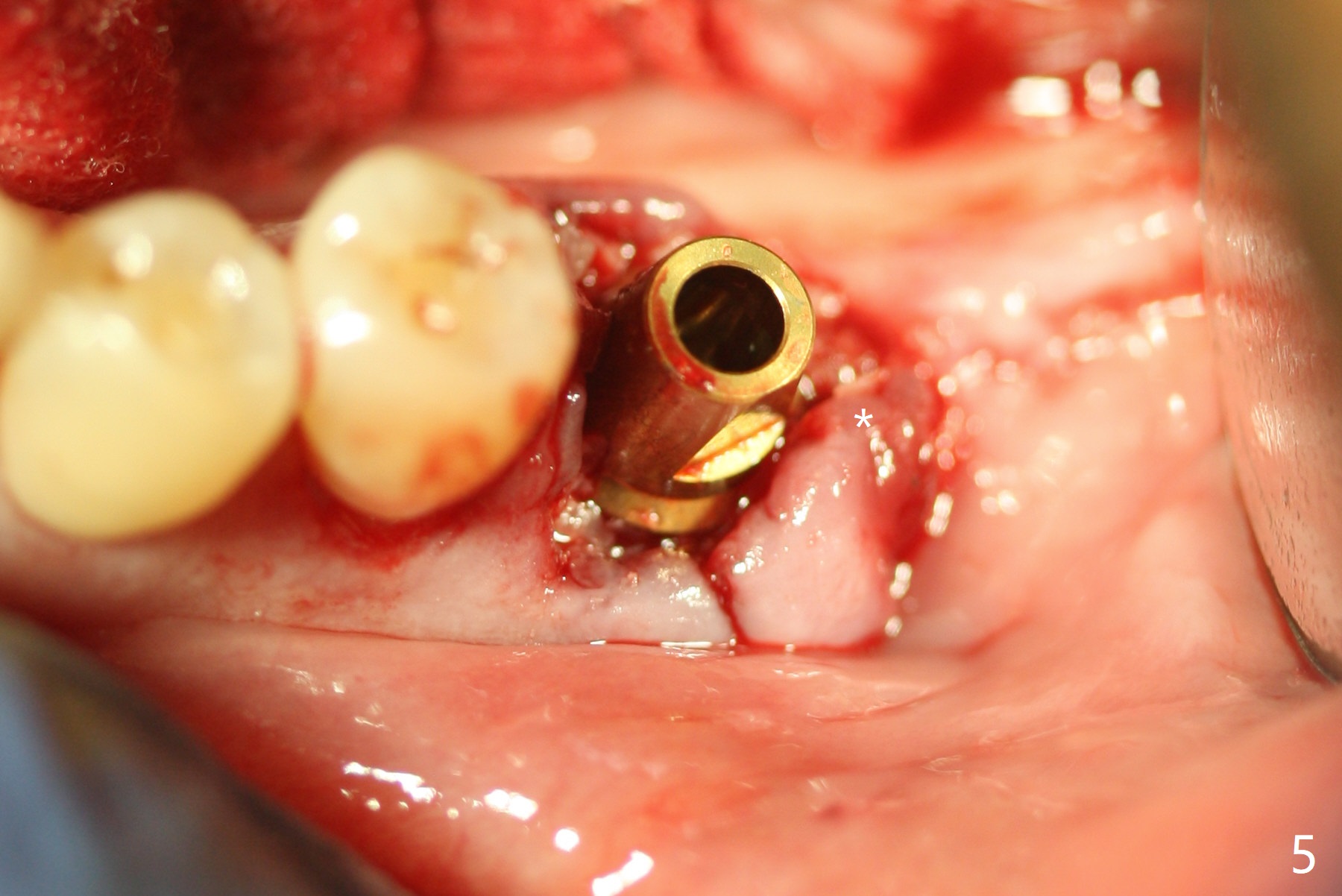
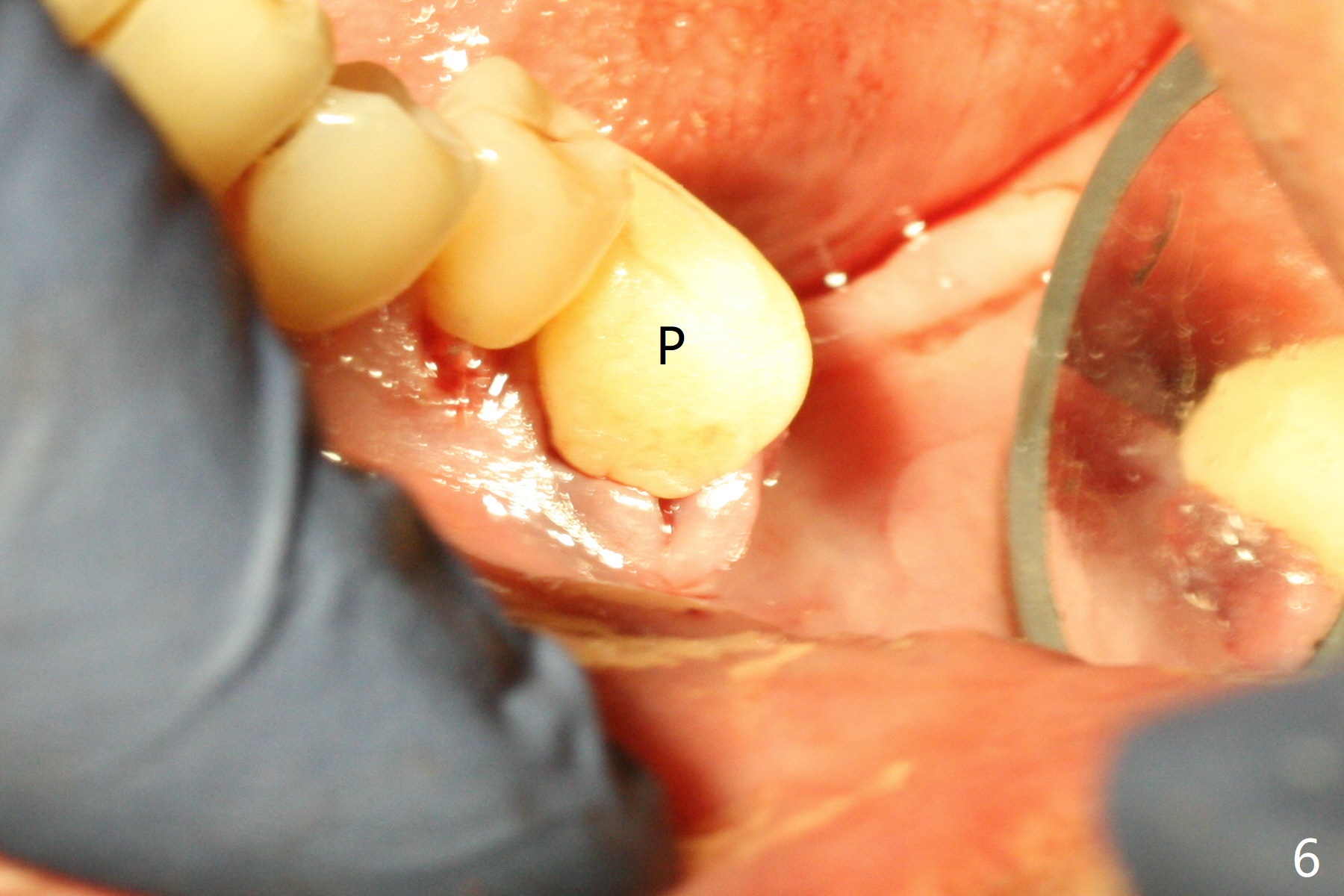
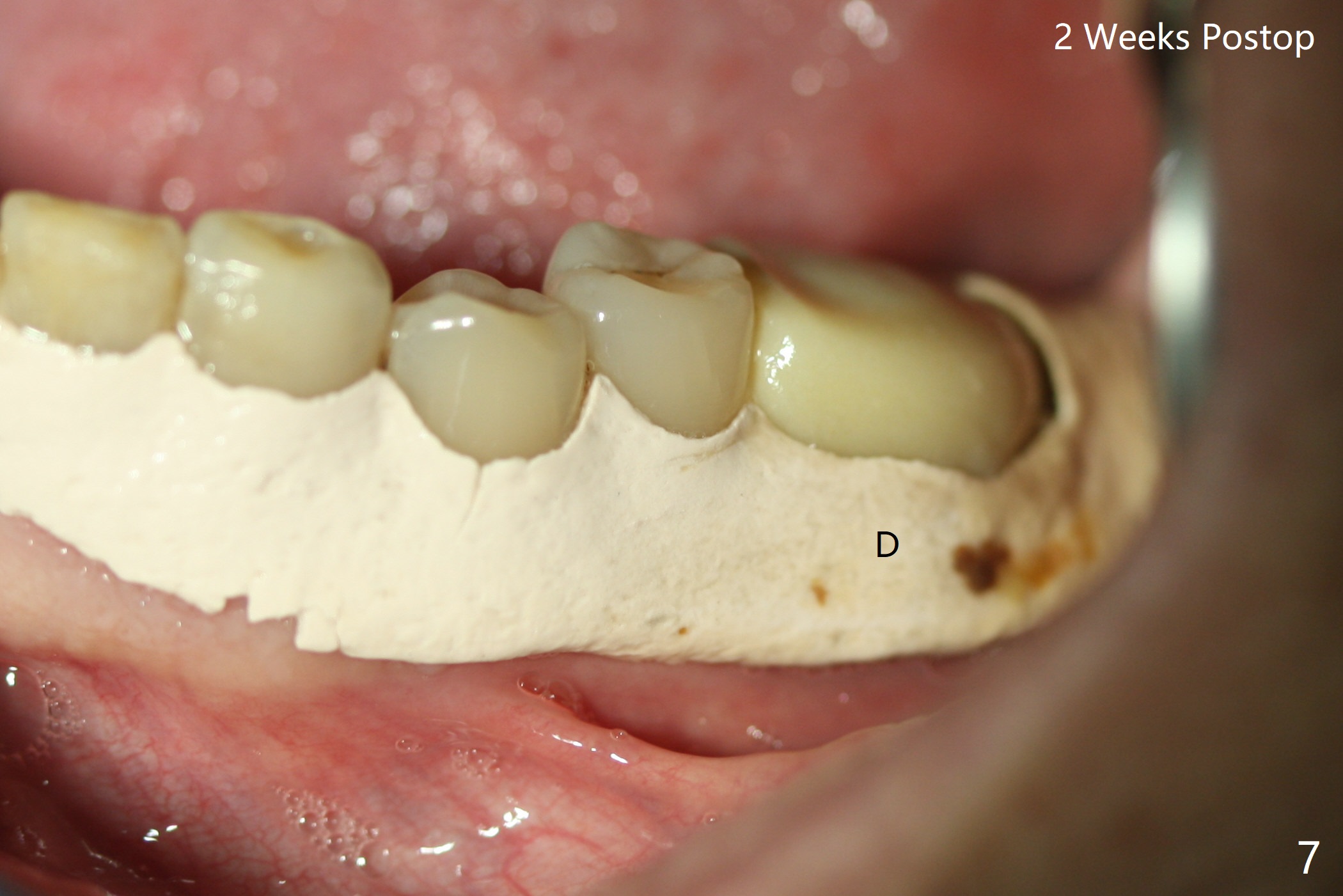
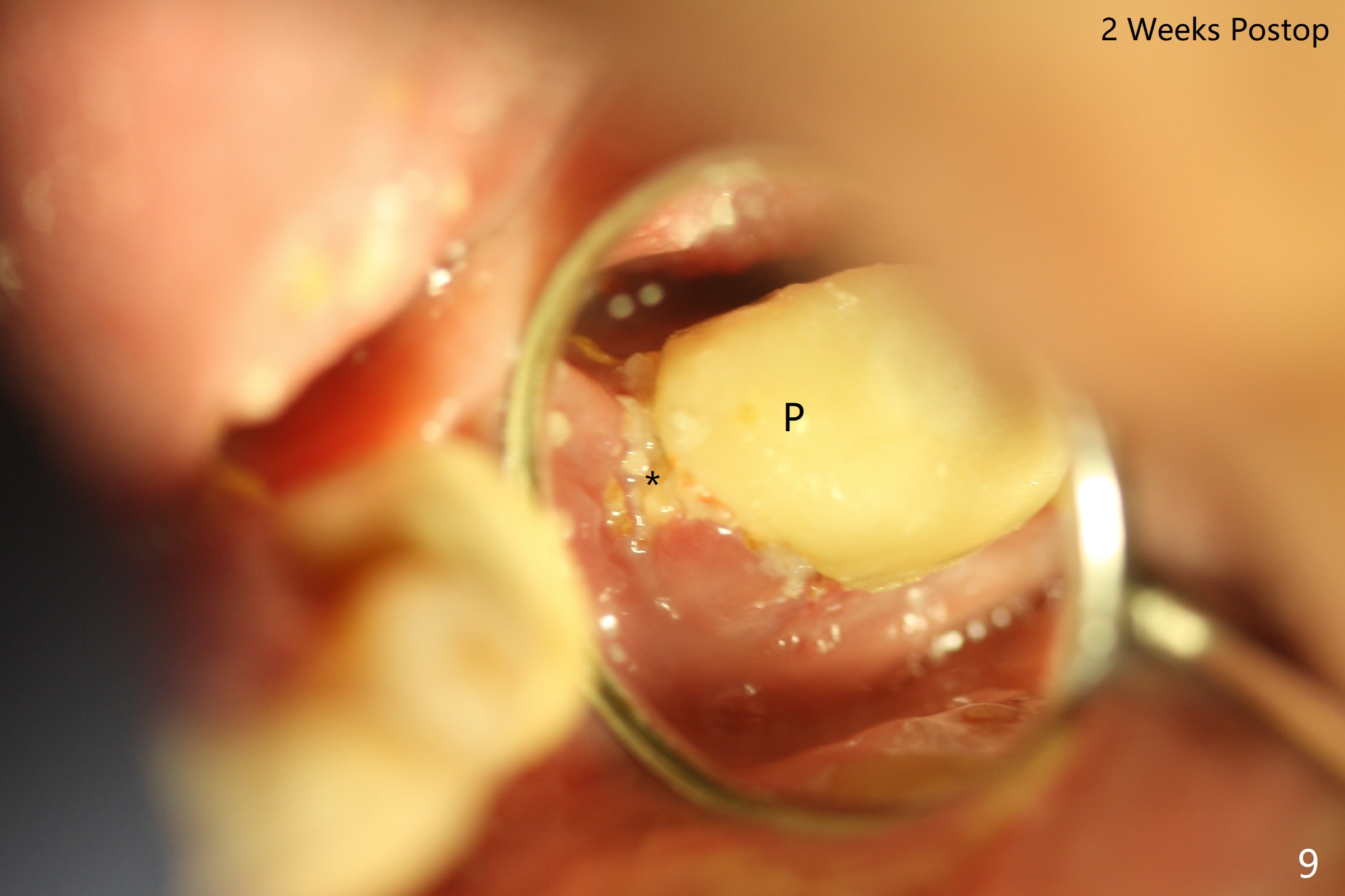
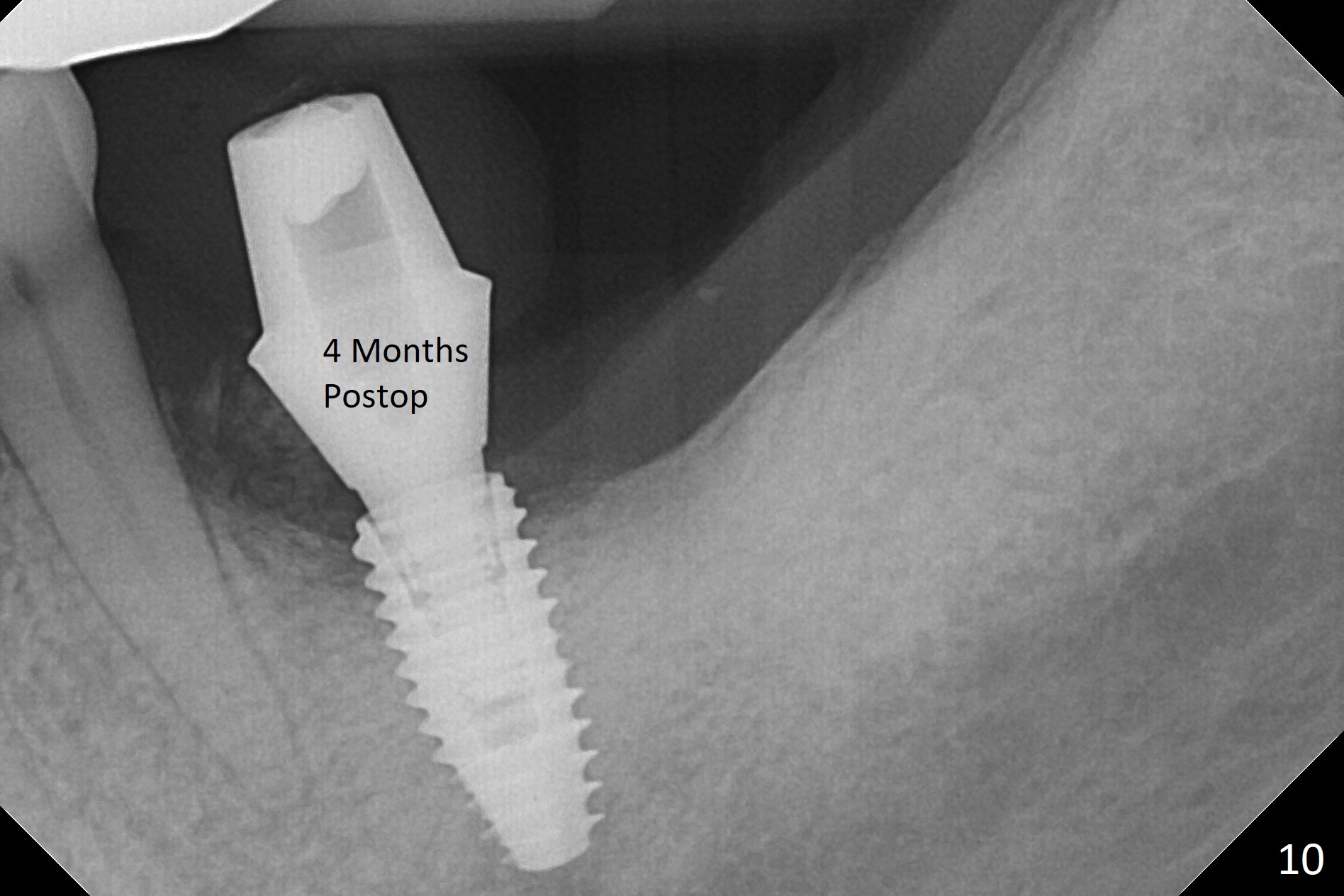
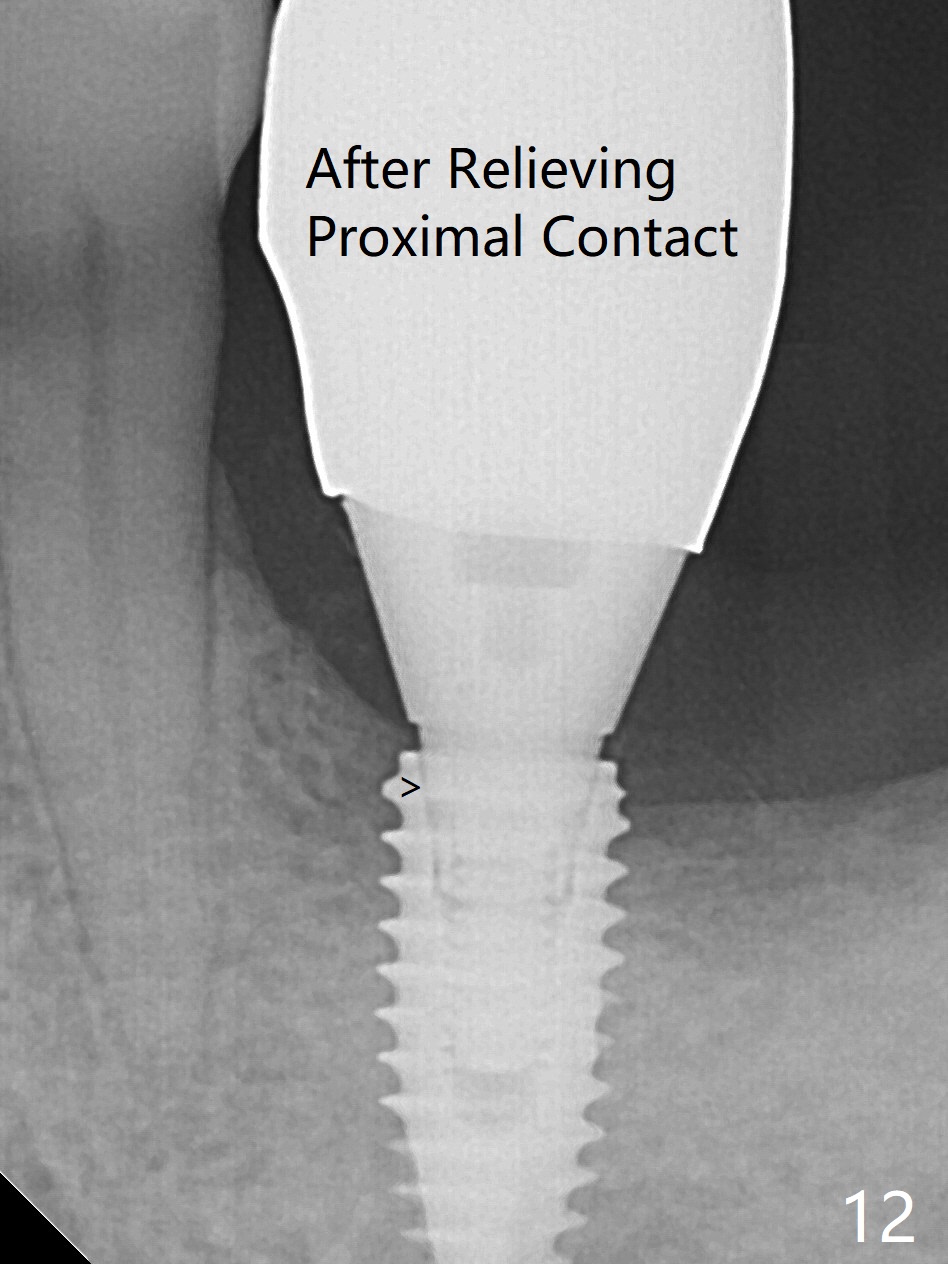
When the patient returns for #19 extraction (Fig.1), there is no 5x10 mm implant available. In fact the smaller one (4.5x10 mm) is able to achieve insertion torque >60 Ncm with more room for autogenous bone/allograft horizontally (Fig.2 *). After insertion of a definitive abutment (6.5x5.5(4) mm), more allograft is placed coronally (Fig.3 *). The gingiva that was between the mesial and distal roots before extraction (Fig.1 *) is transferred distal (Fig.4.5 *). An immediate provisional (Fig.6 P) is fabricated to close the socket opening, followed by periodontal dressing (data not shown). The latter is partially detached 2 weeks postop (Fig.7 D). When it is removed, some of possibly collagen plug is exposed distobuccally (Fig.8). When the plug is removed, some of the bone graft (Fig.9 *) is exposed distal to the provisional (P). New periodontal dressing is applied to keep the exposed graft in place. There is no apparent thread exposure 4 months postop (Fig.10). The abutment is loose 4 months post cementation, probably related to unfavorable crown/implant ratio; but when the abutment is retightened, there is a gap between it and the implant (Fig. 11 >). After relieving the proximal contact of the crown, the abutment is retightened one more time with the same gap (Fig.12 >). In fact the latter is present previously. A narrower abutment with longer cuff appears to be completely seated, probably avoiding contact with the regenerated crestal bone (Fig.13 *). If the new crown gets loose, bury a driver inside the abutment.
Return to
Lower
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table),
Trajectory,
Weichat,
Iatrogenic Defect with Free Hand Osteotomy,
3,14
Xin Wei, DDS, PhD, MS 1st edition
02/04/2019, last revision
04/15/2020