




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
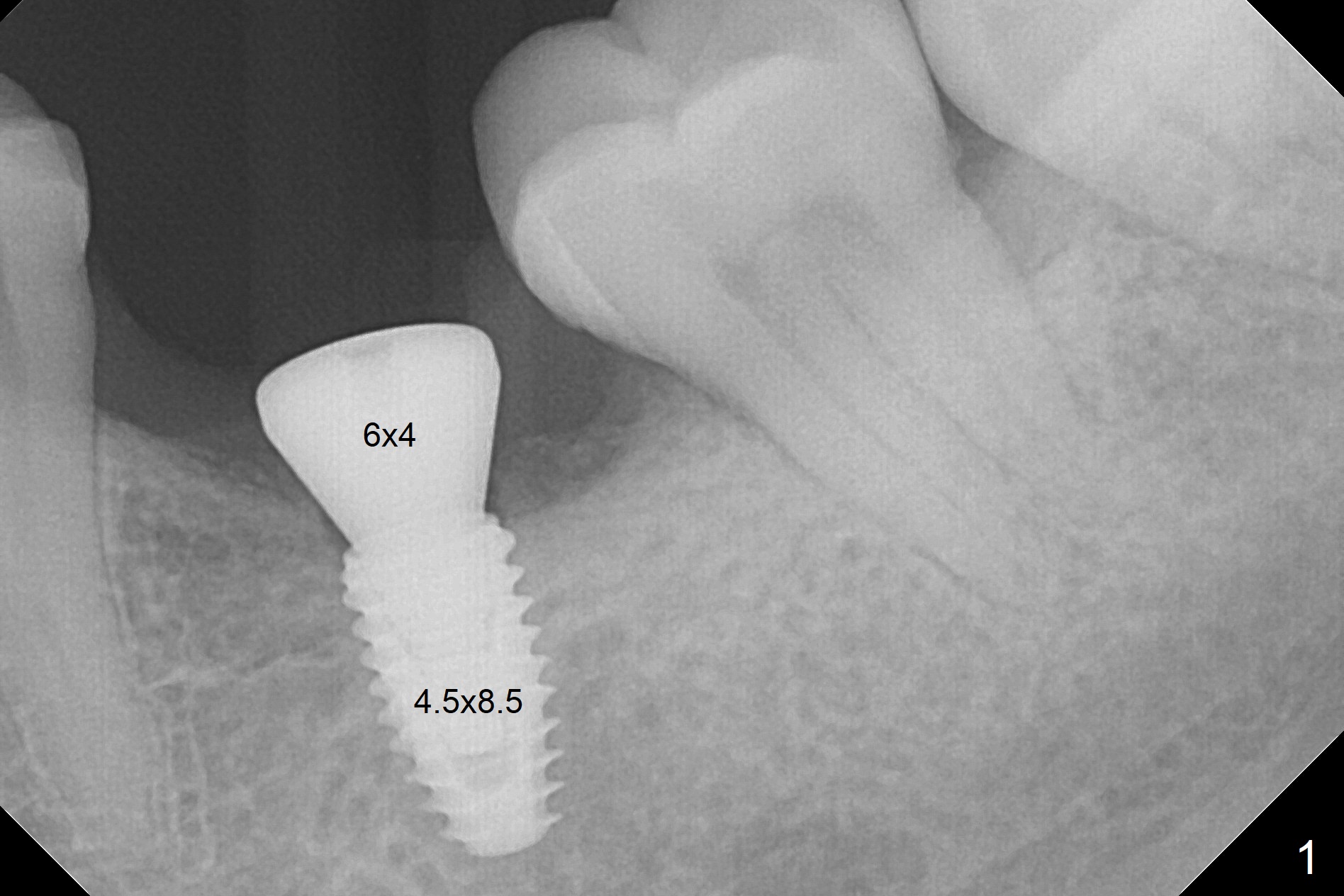
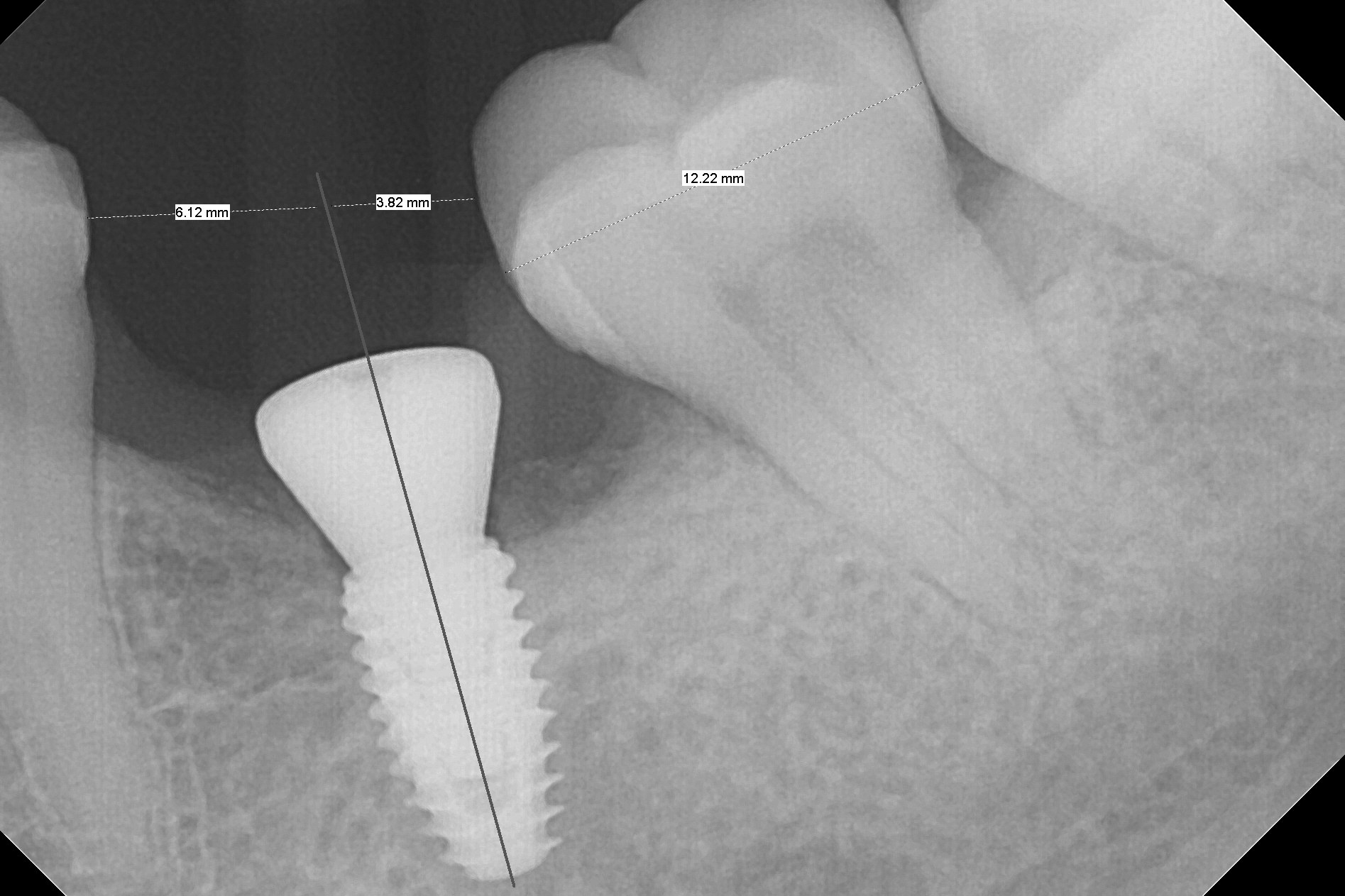
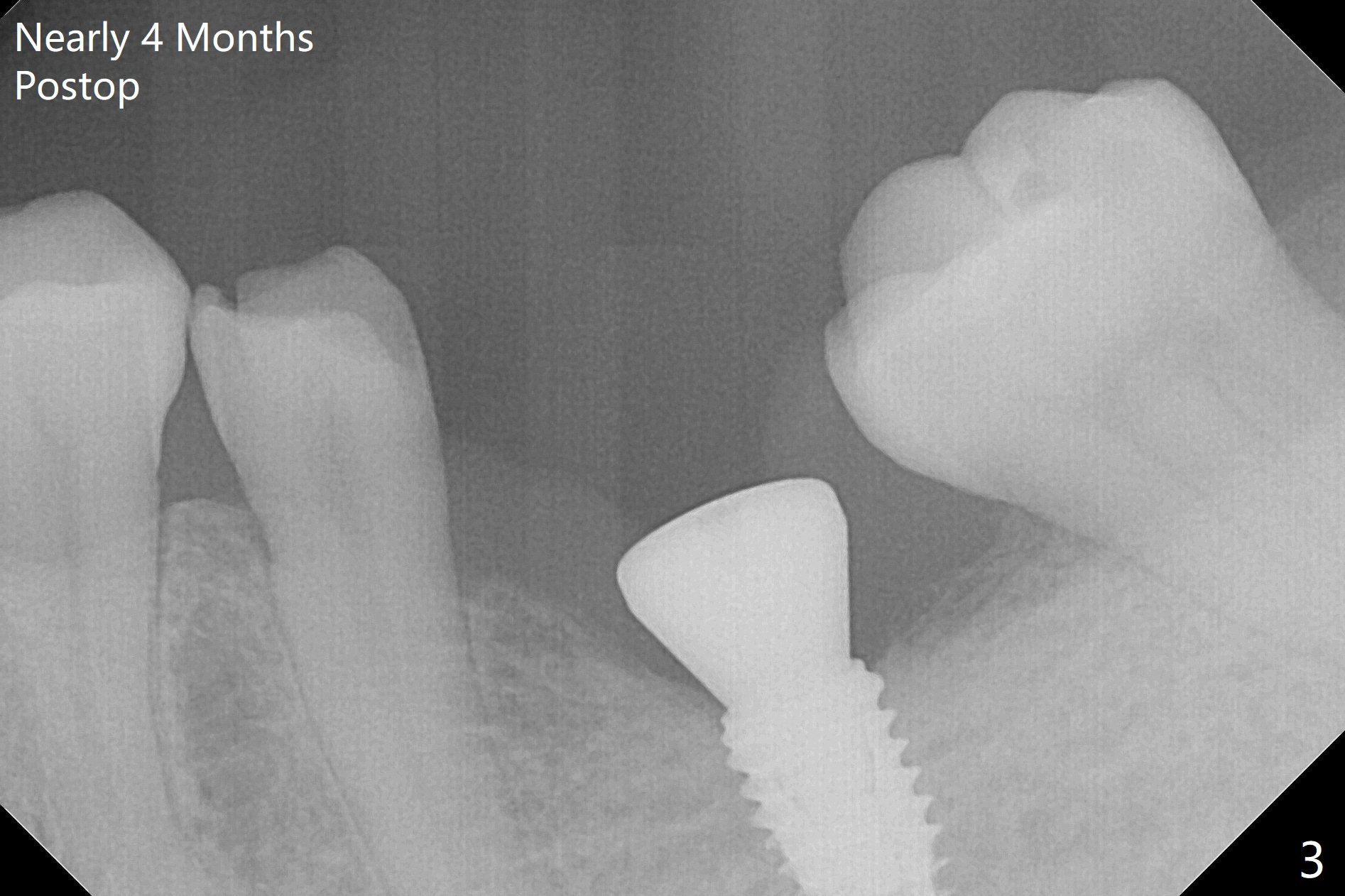
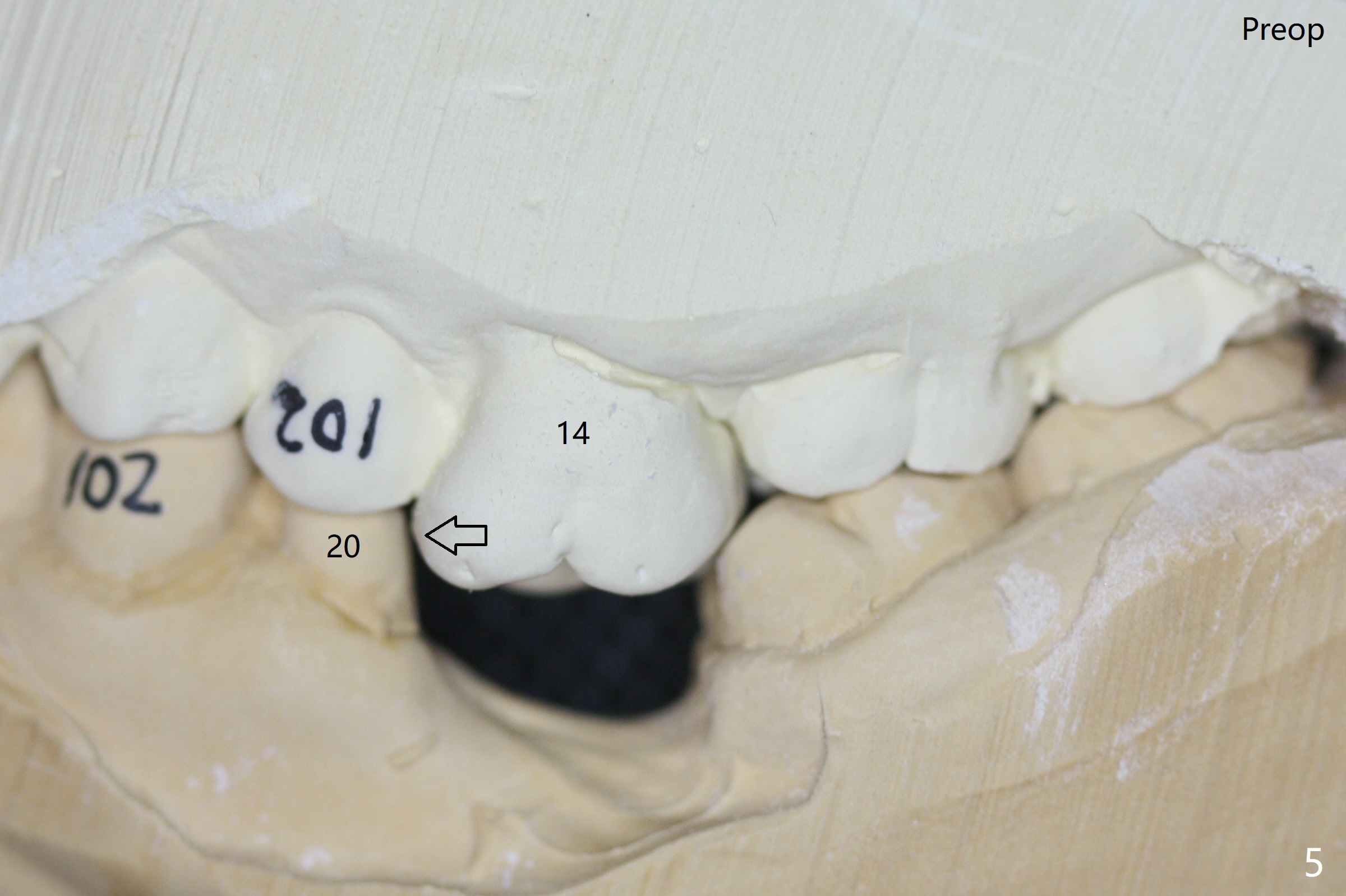
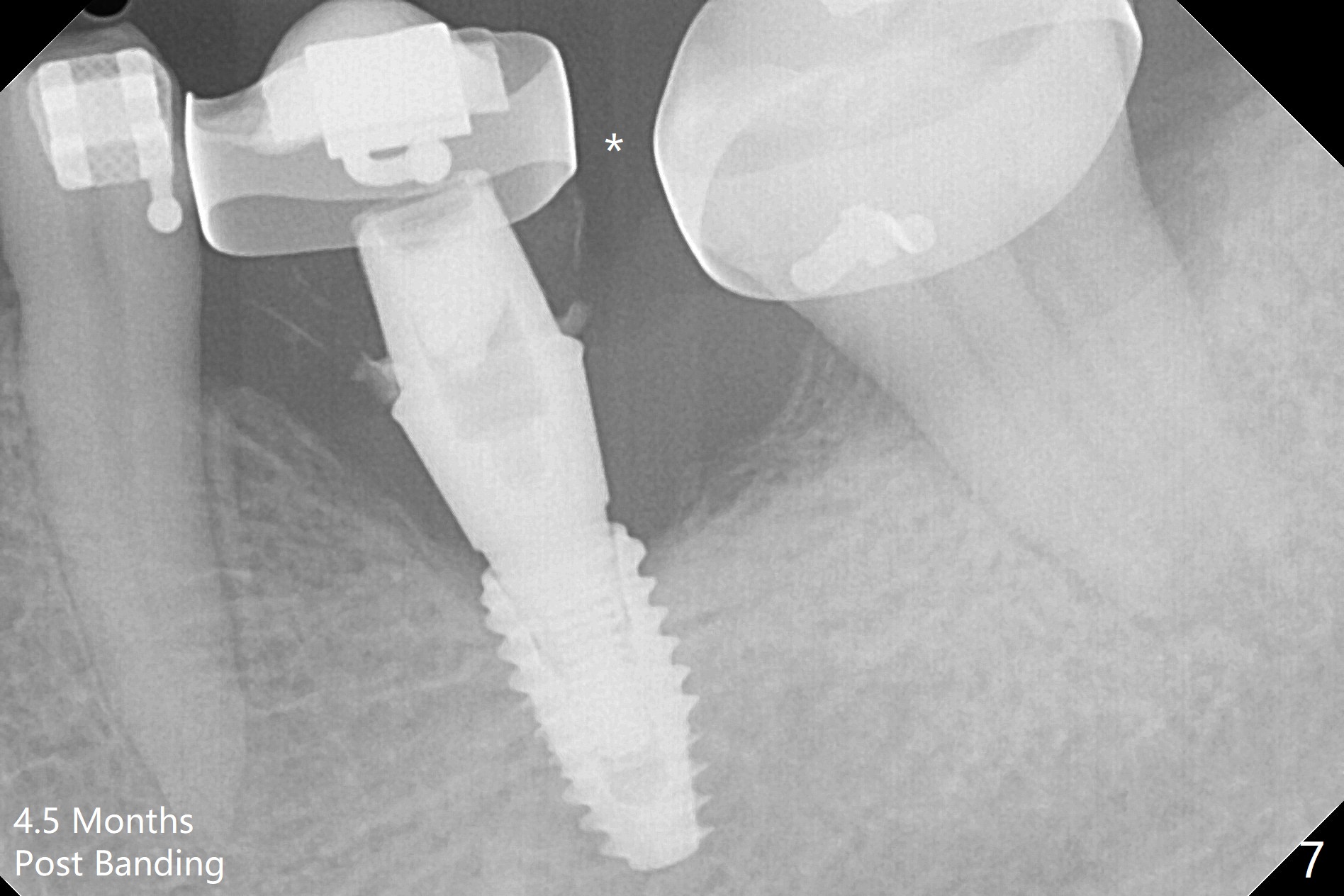
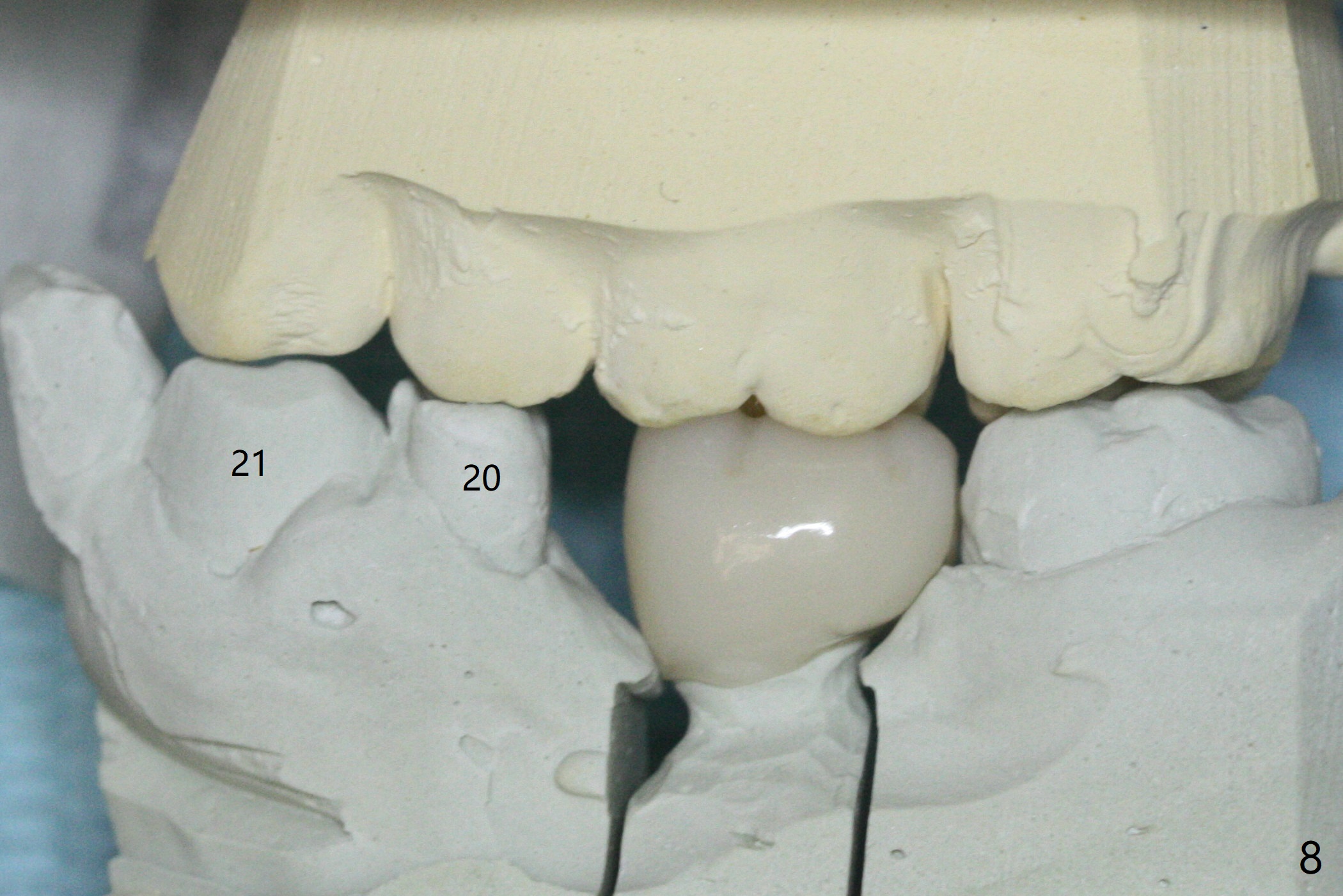
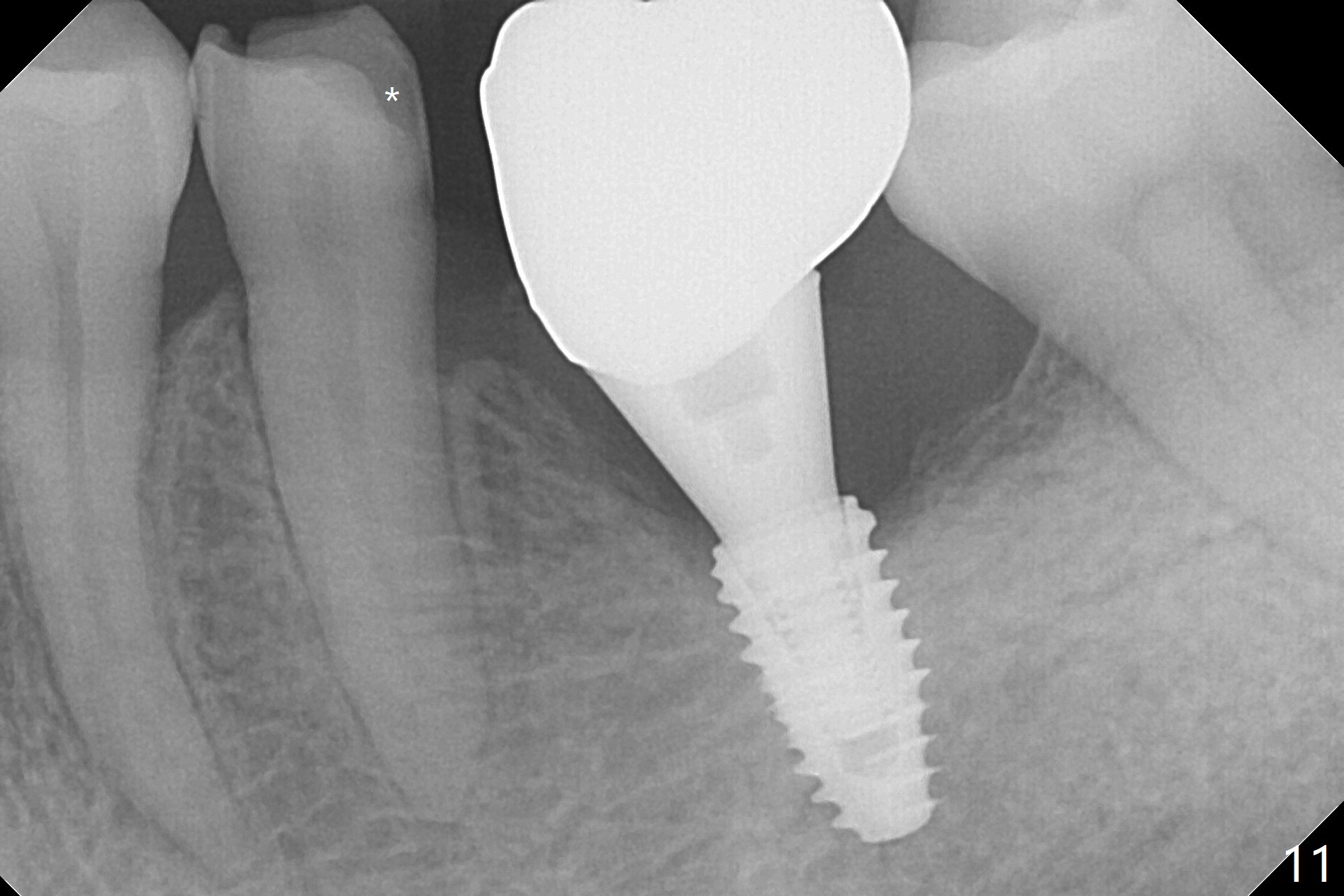
Distal Placement for Upright
With 34 mg of Lidocaine and 17 mcg of Epinephrine (local infiltration), a 4.5x8.5 mm implant is placed with guide. The insertion torque is ~50 Ncm. It is placed in precise depth and in a short period of time (tolerable to the operators and patient, easier than mini-implant placement, Fig.1). There is no postop pain or paresthesia. The mesidistal position is within treatment plan (Fig.2). Miniimplants are placed to intrude #14 14 days prior. The teeth #16,17 and 32 are extracted 3 months postop. Minimal bone resorption at the crest is noted nearly 4 months postop (Fig.3). Bands and brackets are placed #18 upright 4 months postop (Fig.4 (14 niti wire)). The buccal and lingual view of the preop model shows that the supraerupted 1st molar (#14) has close relationship with the distal surface of the tooth #20 (Fig.5,6), accounting for the severe wear of the latter (Fig.8-11). The implant not only acts as an anchor to upright #18 in 4.5 months post banding (Fig.7 *), but also as an occlusal stop so that #18 has no interference to be moved. The stress on the implant results in radiating trabecular pattern (Fig.7,11 (9,11 months postop), as compared to before loading (Fig.1,3)). Restoring the distal contour of #20 with composite (Fig.12 C) makes it easy to close the space by adding porcelain the mesial surface of the implant crown. The crown/abutment is loose in China 7 months post cementation.
Return to Lower Molar Immediate Implant, Armaments Xin Wei, DDS, PhD, MS 1st edition 05/24/2018, last revision 12/28/2019