




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
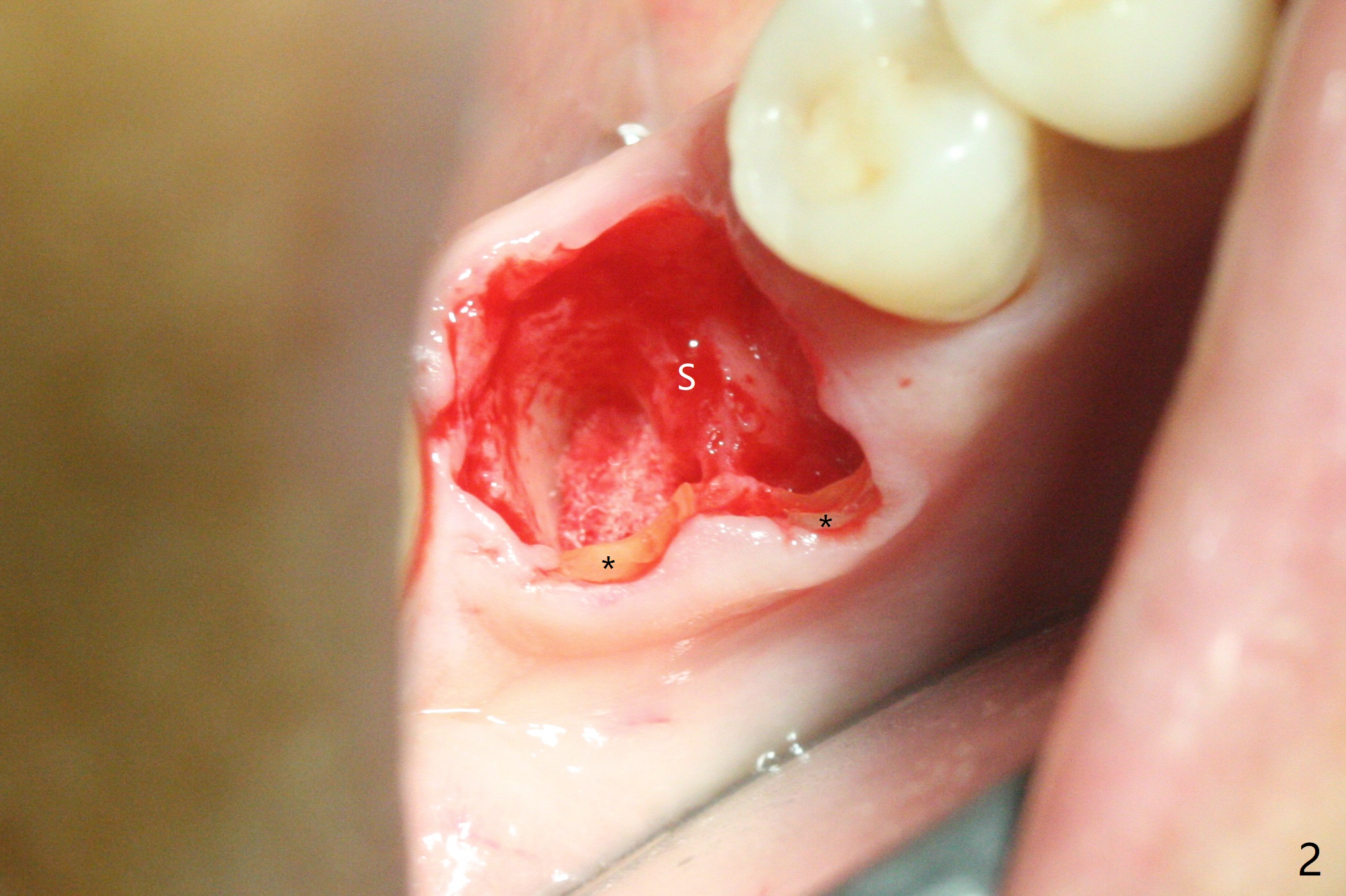
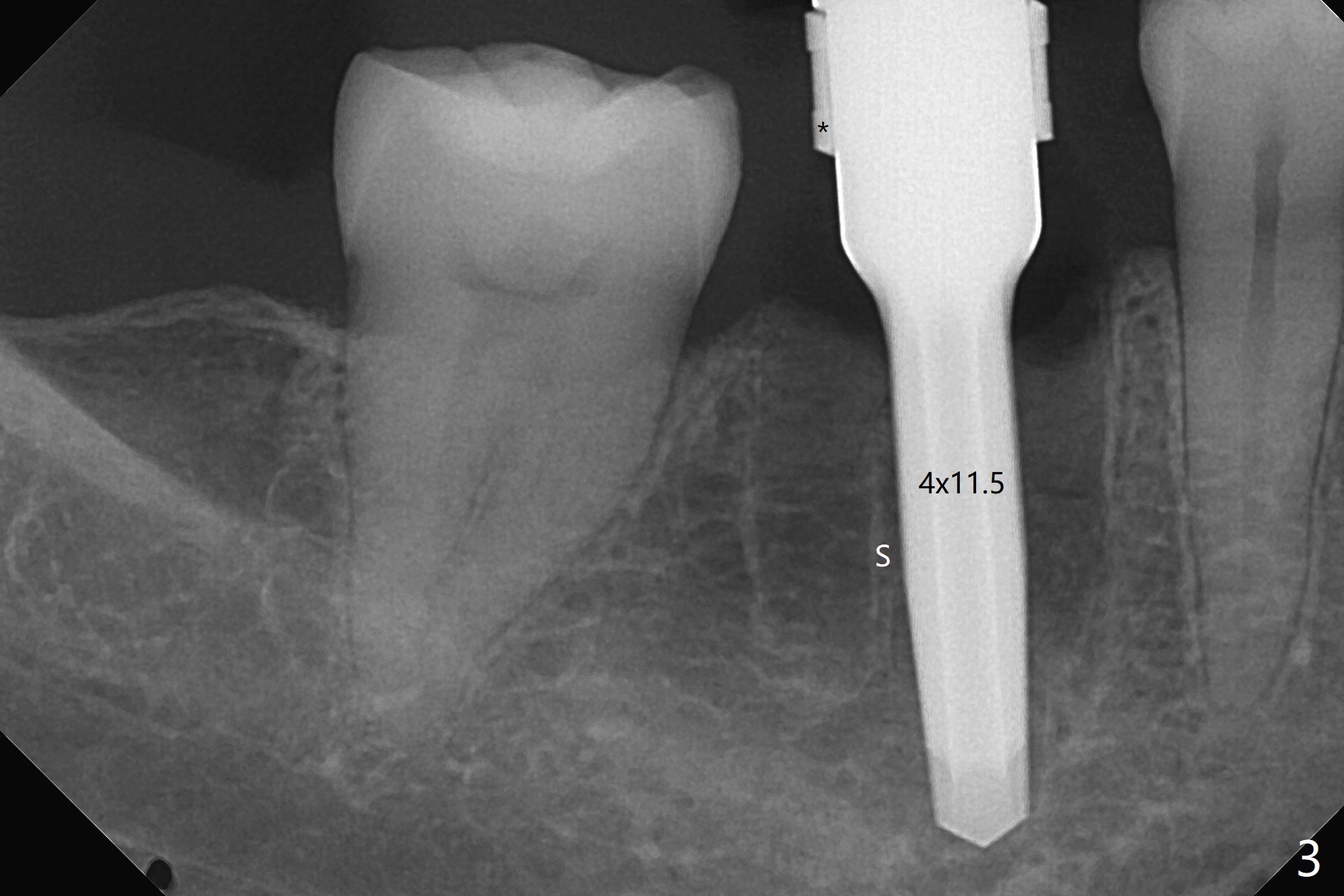
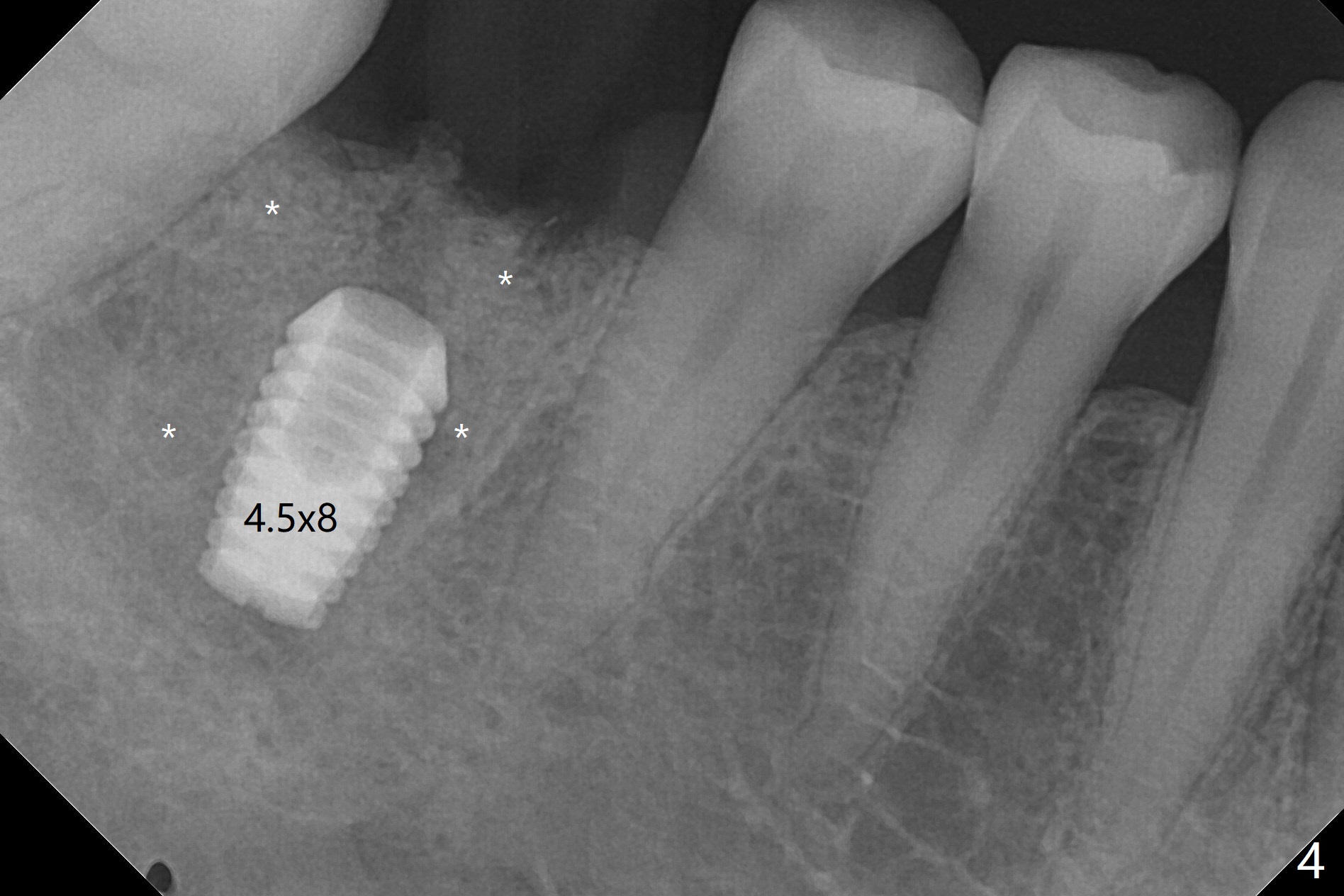
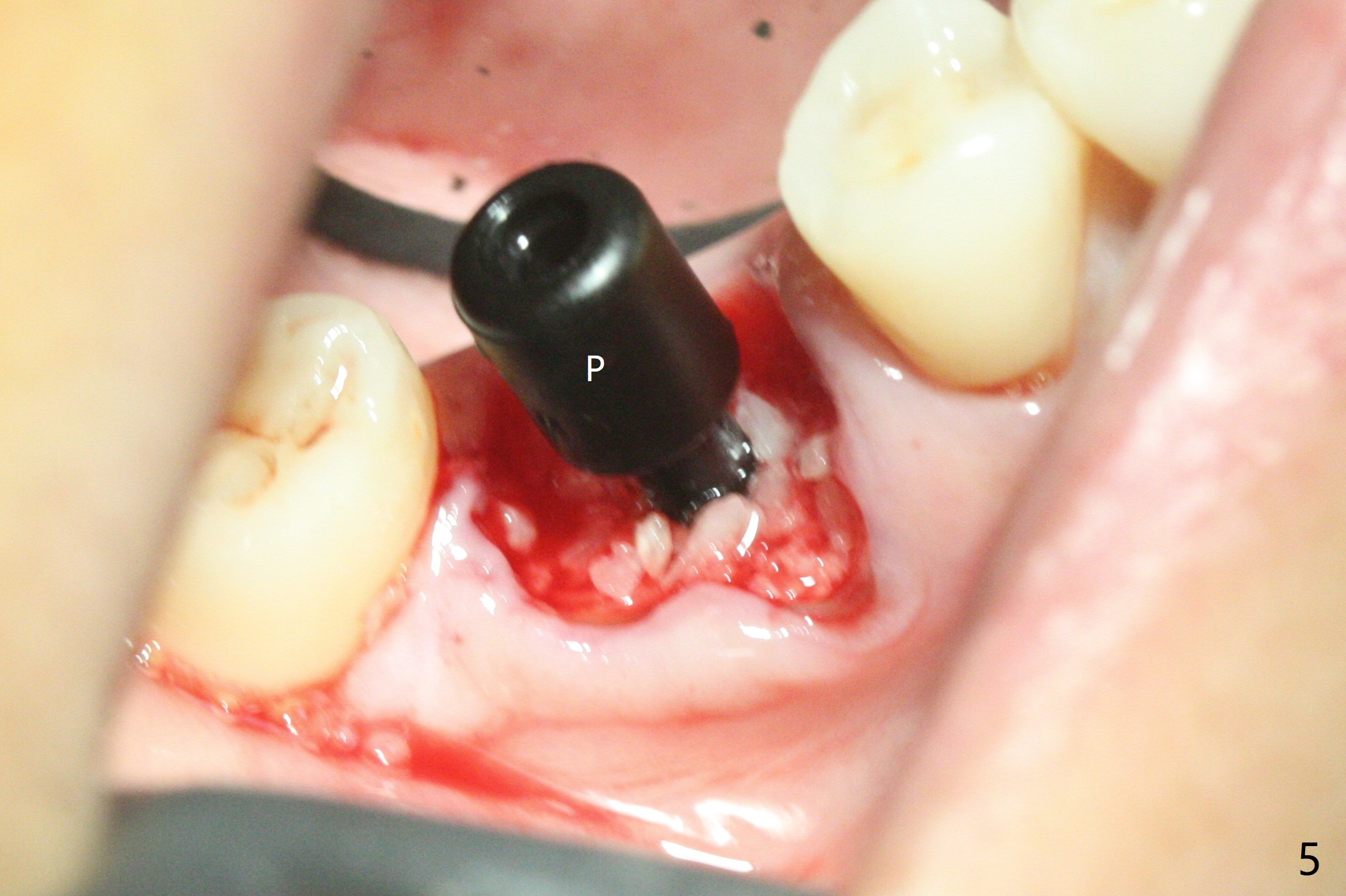
Stability of Bicon Implant (I)
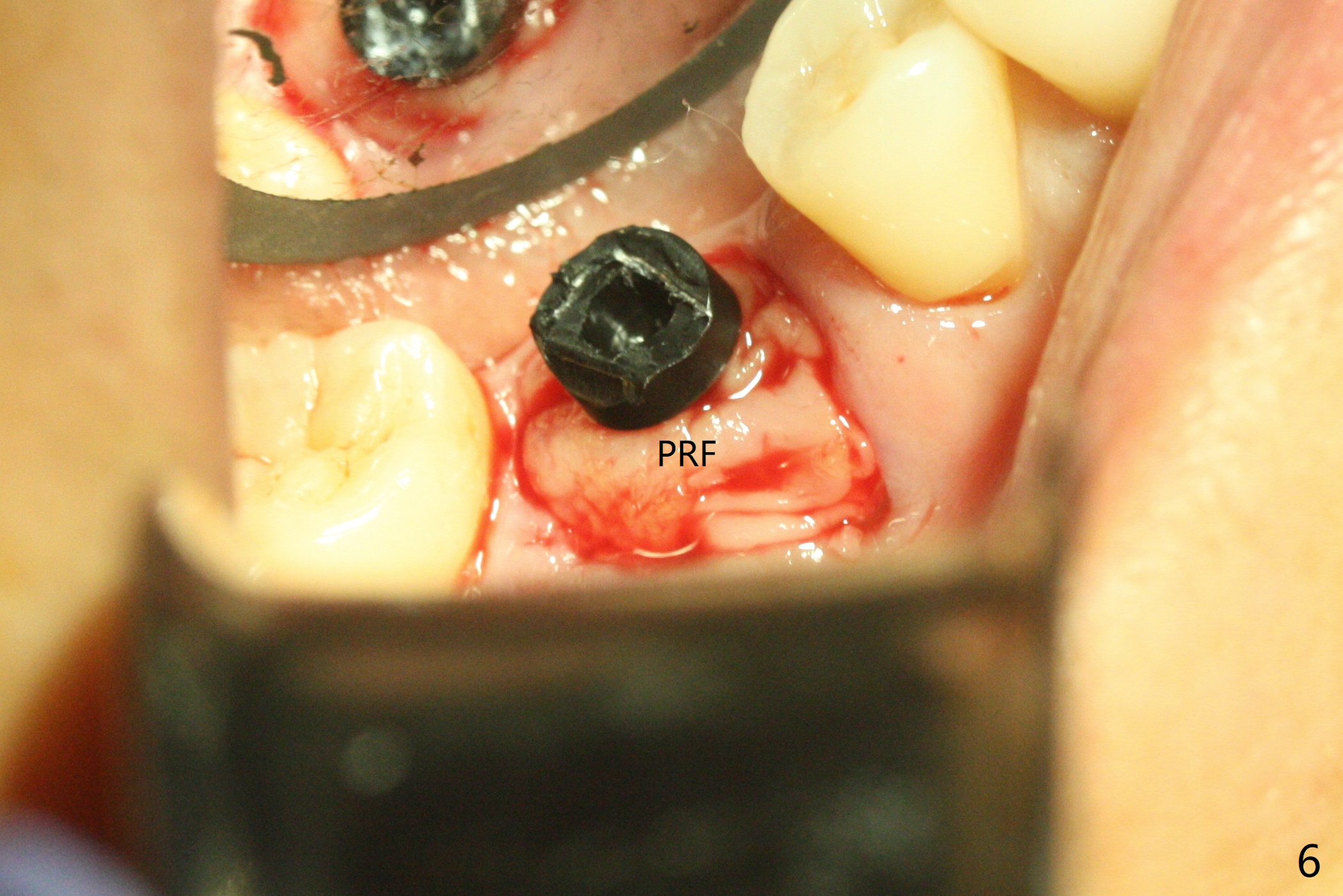
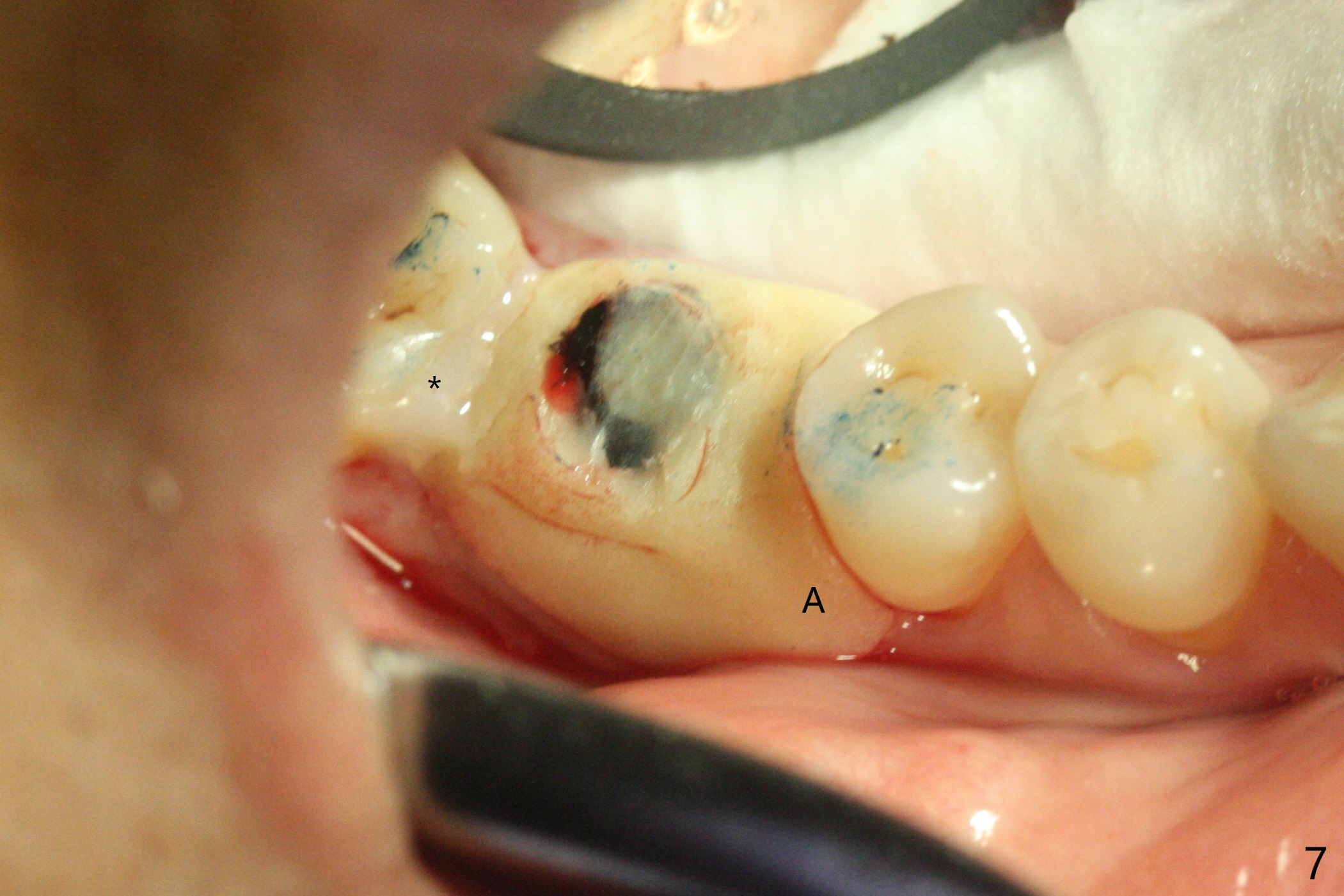
To prevent further postop buccal gingival recession at #30, socket shield is formed with removal of the residual roots (Fig.1,2 *). Osteotomy is initiated in the septum (Fig.2 S, to be flattened with bone trimmer and surgical round bur) and gradually slides slightly into the mesial socket in spite of using surgical guide (Fig.3 *: sleeve). Following 4.5x11.5 mm drill, a 4.5x8 mm Bicon implant is pressed fit; its stability is lightly enhanced with placement of sticky bone in the remaining sockets (Fig.4 *) and around the black plug (Fig.5 P). After removing the coronal portion of the plug to reduce occlusal interference, two pieces of PRF are wrapped around the remaining plug (Fig.6). The main stability of the implant is obtained when setting acrylic (A in Fig.7) is applied into the edentulous space (undercut). After acrylic setting, flowable composite (*) is added distal for further retention. One month postop, the flowable composite is detached. The provisional is sectioned; the black plug is cut. The socket heals with exposure of the mesial socket shield (Fig.8 >). The black healing plug and the mesial socket shield remains exposed 3 months postop (Fig.9). When a 4.5x6.5 mm temporary abutment is placed, the buccal gingiva is blanched and the mesial socket shield is pushed buccal (Fig.10). The implant appears to remain covered by the bone 3 months postop (Fig.11).
Return to
Lower
Molar Immediate Implant,
Prevent Molar Periimplantitis (Protocols,
Table)
Trajectory II
Shield
Xin Wei, DDS, PhD, MS 1st edition
11/18/2019, last revision
02/21/2020