
,%20bone%20graft%201.jpg)
,%20bone%20graft%202.jpg)


%20for%20impression,%20subgingival%20M.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Septal Placement
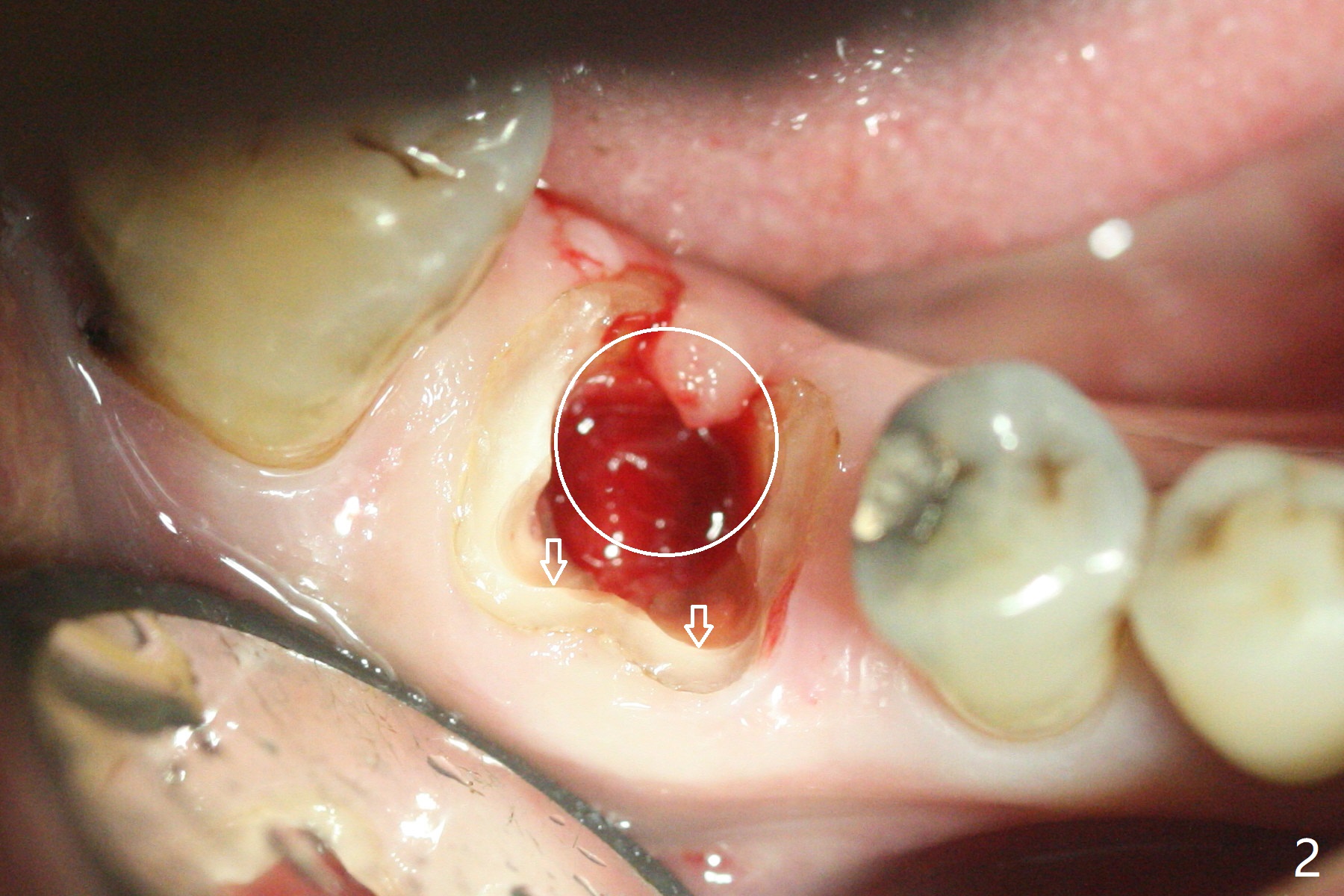
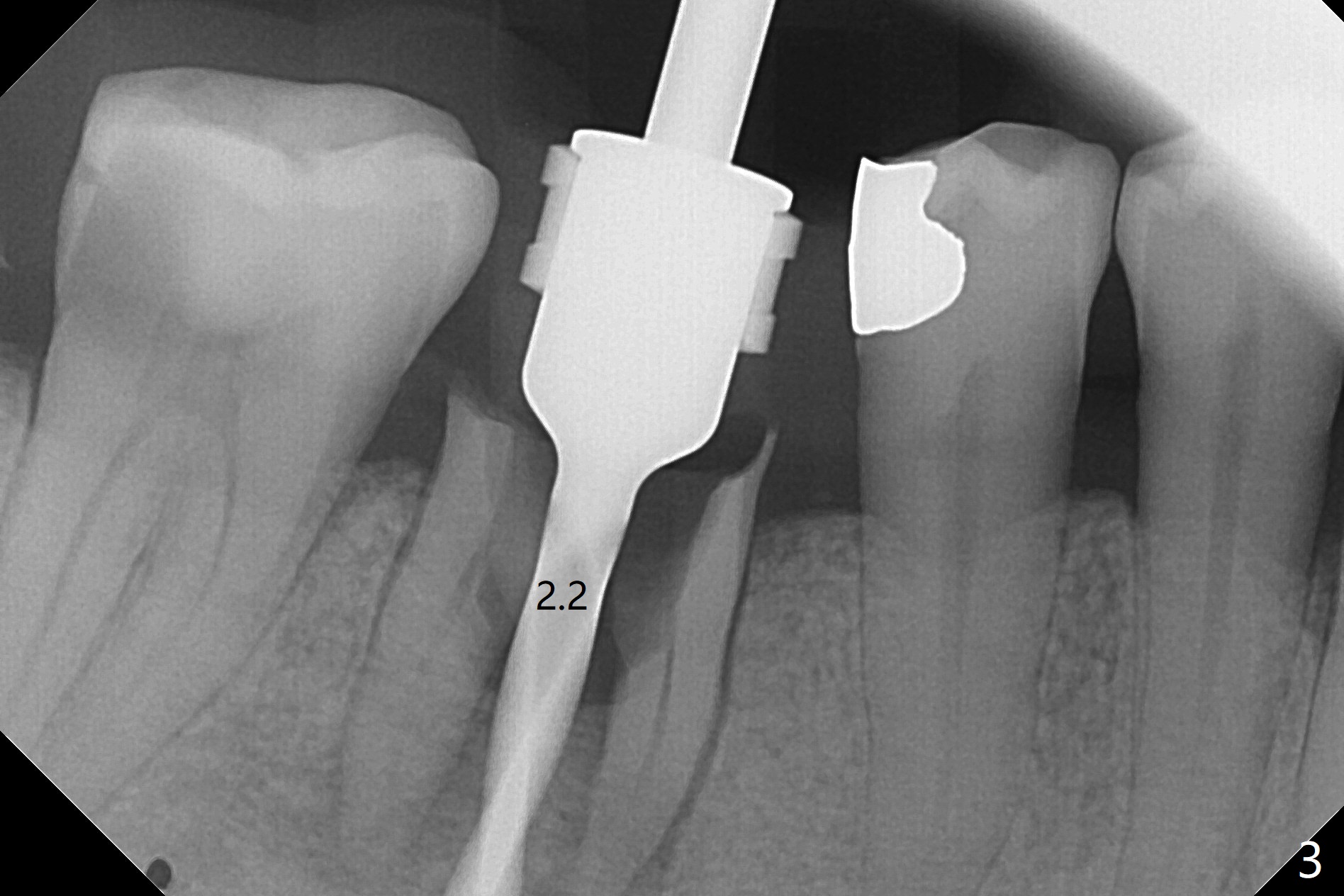
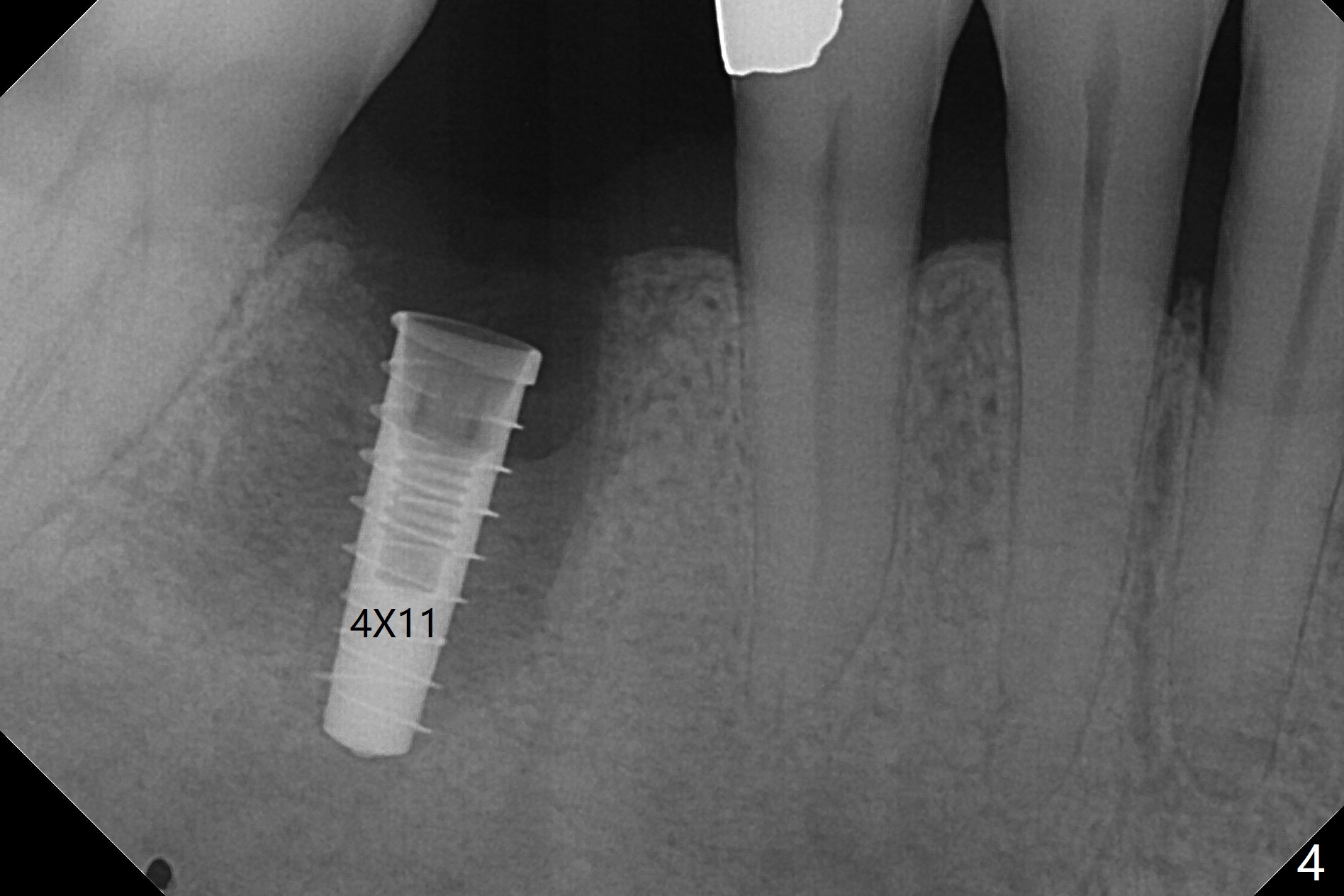
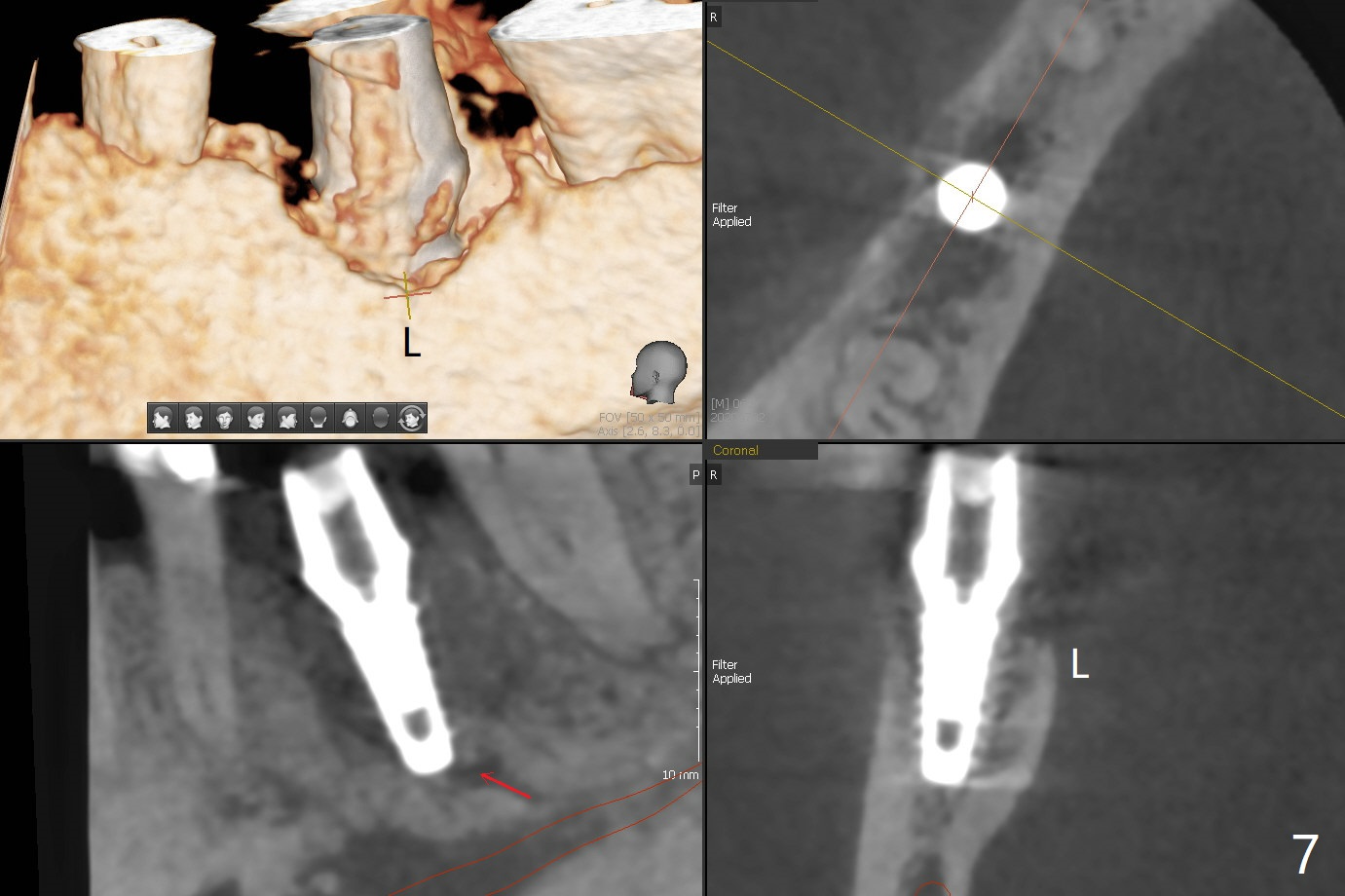
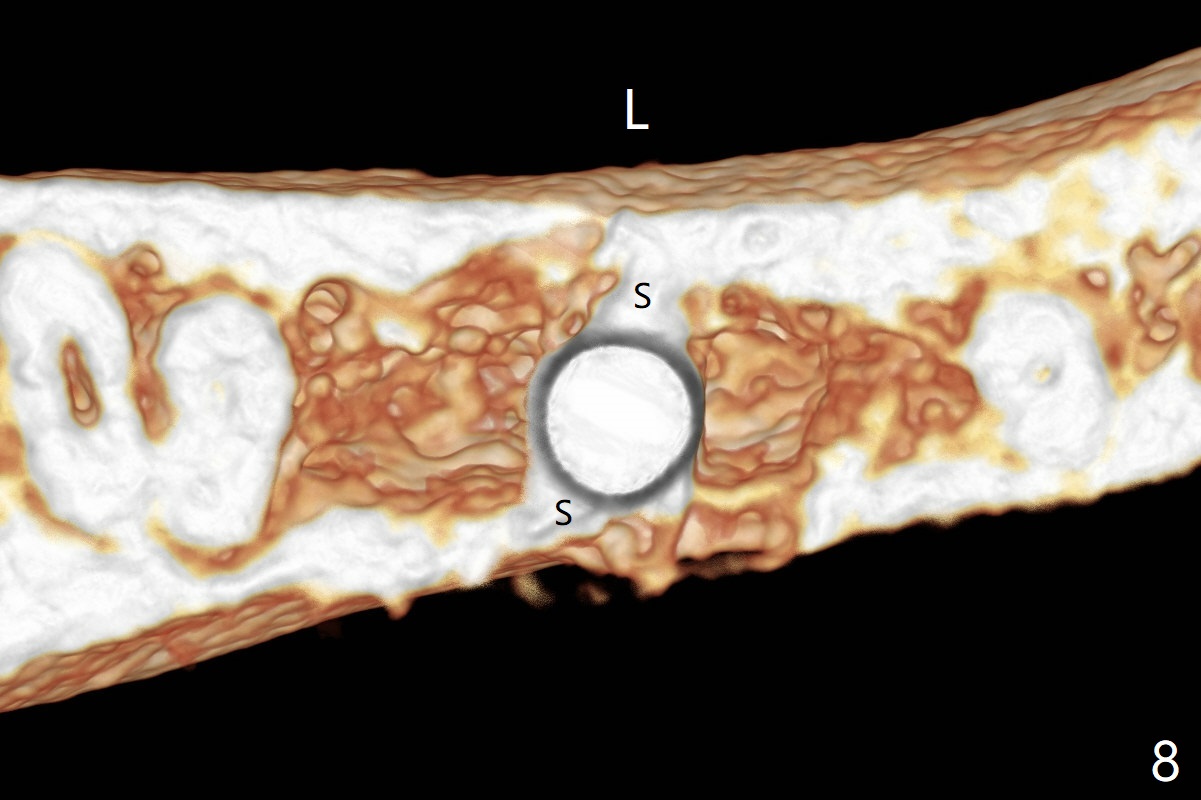
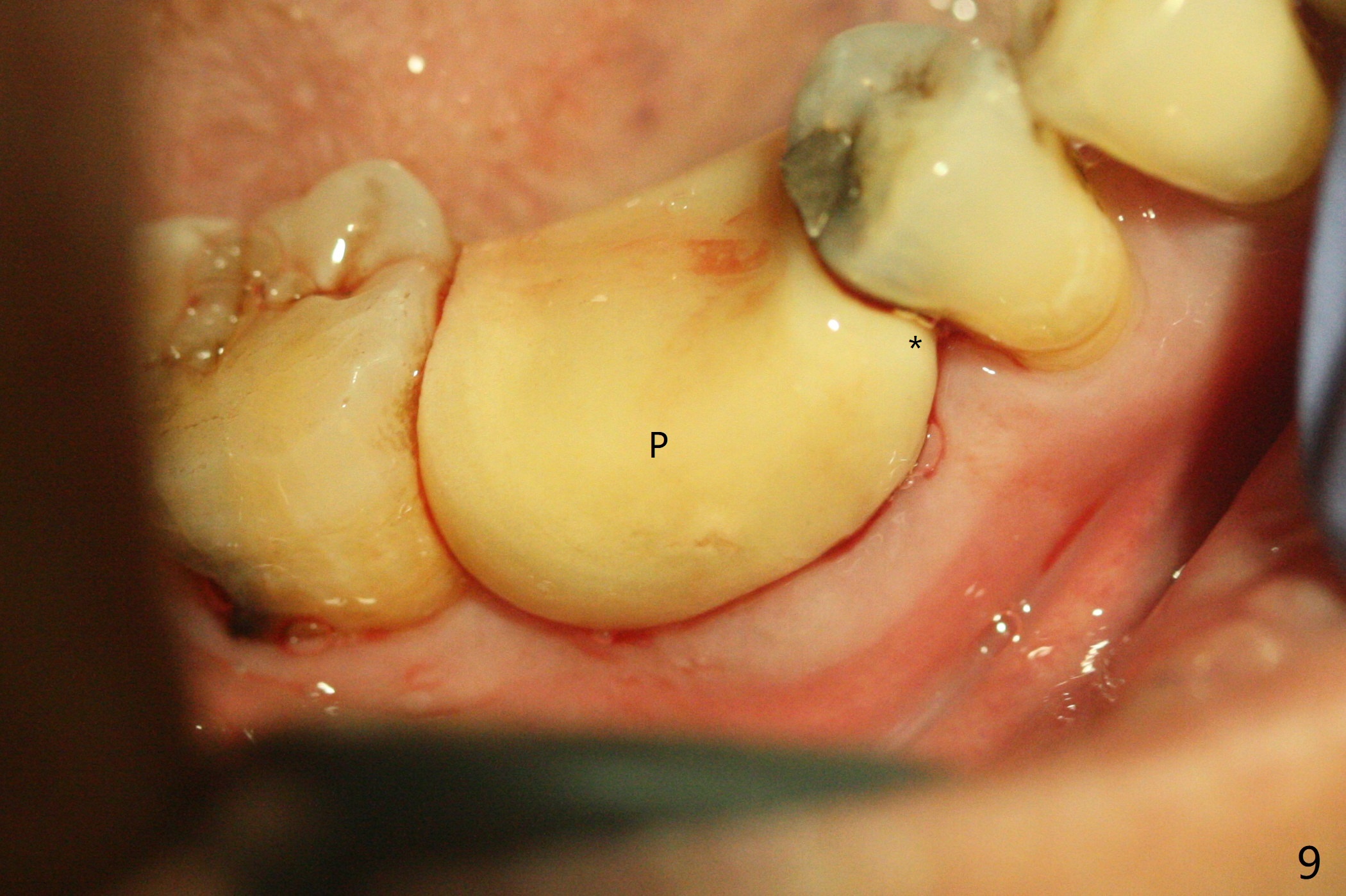
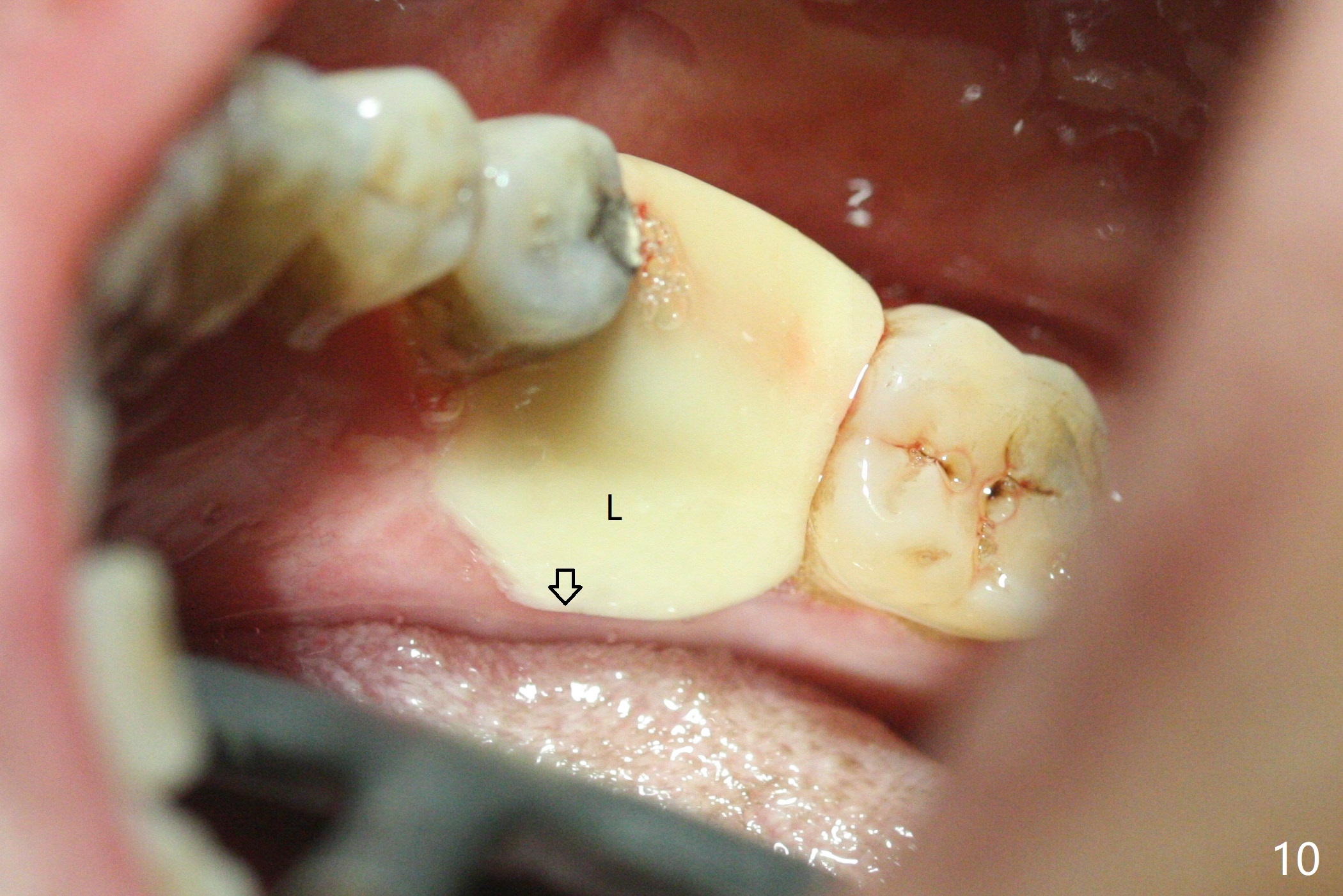
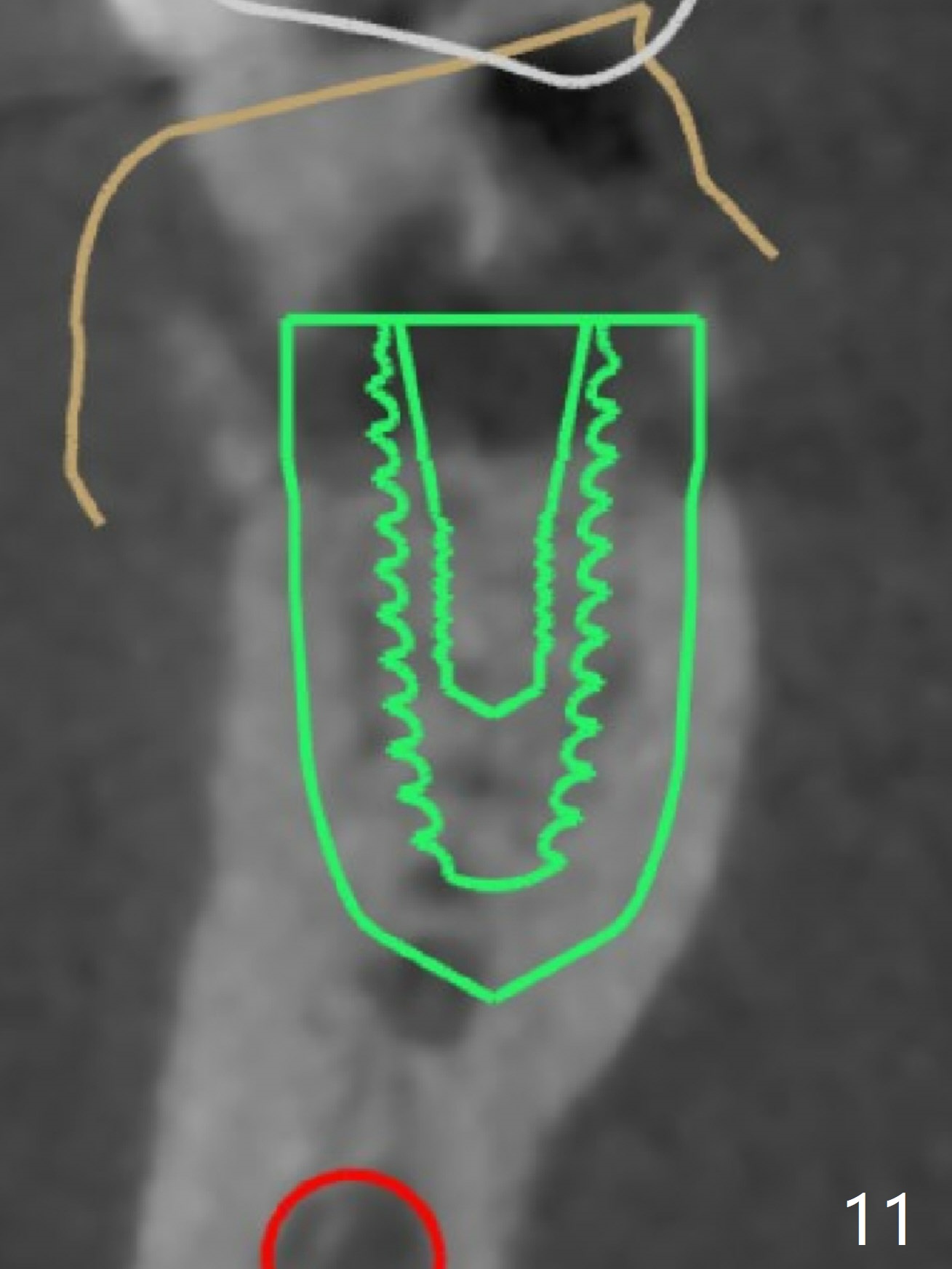
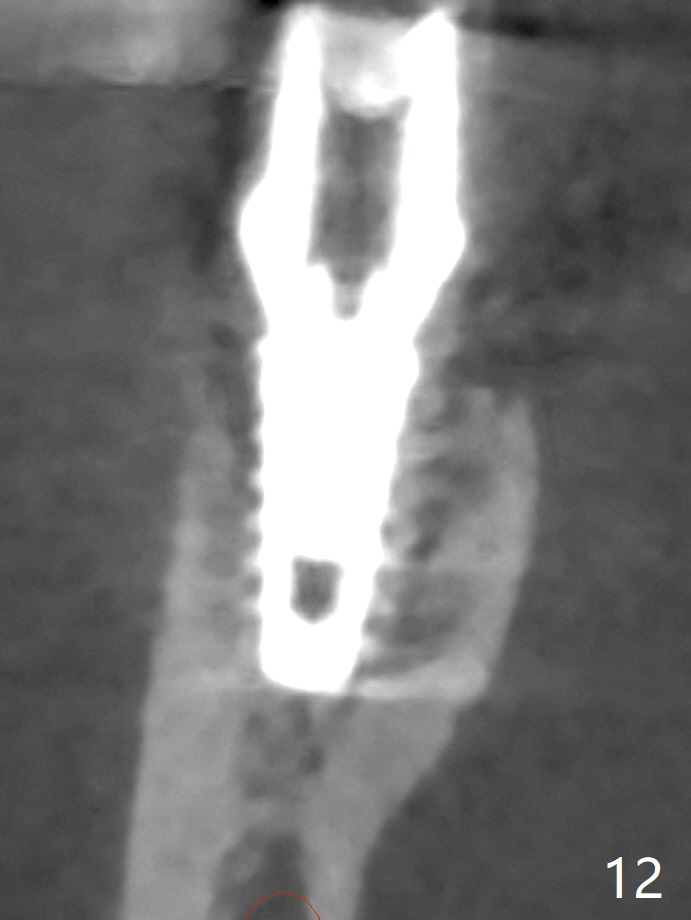
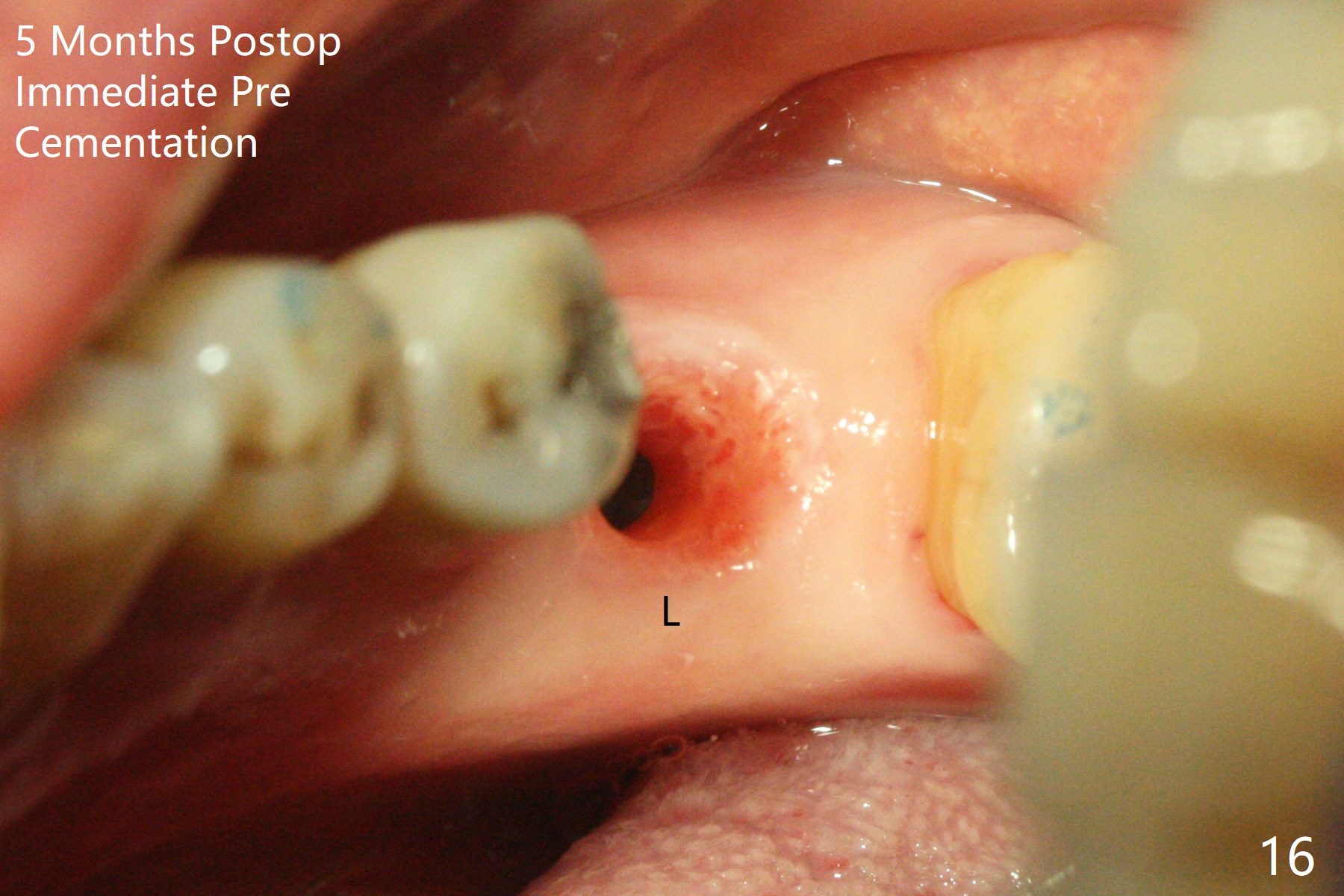
As planned, the crown of the tooth #30 with lingual (Fig.1 L) caries is removed and flattened with surgical handpiece so that the guide is able to be seated without interference. The osteotomy by 10.5 mm offset bone trimmer is lingual (Fig.2 white circle; due to in part the lingual caries and in part design error); in order to let the osteotomy to bounce back buccal, the part of the buccal roots are removed by surgical bur (arrows). The initial osteotomy by 2.2 mm drill is in the middle of the septum (Fig.3). After the last drill (3.5x11.5), the remaining roots are easily removed with proximators; a 4x11 mm dummy implant is placed with low stability and supracrestal lingual (Fig.4). Therefore a 4.5x9 mm final implant is placed with low torque. Following 4x11.5 mm drill, the torque increases to 20 Ncm. With insertion of healing screw, sticky bone (Fig.4 *: .5-1 mm cortical/cancellous allograft) is heavily packed around the implant (arrow), which apparently allows removal of the healing screw and placement of a 6x5.7(3) mm pair abutment without loosening the underlying implant. More bone graft is placed (Fig.6), followed by 2 pieces of PRF membranes. Although the implant is slightly buccally placed (Fig.7, due to over-removal of the buccal root, Fig.2 arrows), it is placed in the septum (Fig.8 S). To further compensate for the low implant stability, setting acrylic is applied in the edentulous area, particularly into the undercuts of the neighboring teeth (Fig.9 *) and around the abutment. The lingual margin of the acrylic dressing is extended (Fig.10 arrow) to cover the soft tissue defect associated with the lingual caries. As compared to the design (4x10 mm, Fig.11), the implant (4.5x9 mm, Fig.12) is placed buccal and ~ 2 mm deeper, reducing the chance of periimplantitis. The acrylic dressing is in place, but has mobility. The gingiva is healthy 2 weeks postop. The dressing is removed 1 month postop; the socket heals around the abutment buccal (Fig.13) and lingual (Fig.14). In spite of the immediate provisional, the abutment margin is substantially subgingival mesial 4 months postop, extremely difficult to take impression. A smaller diameter and longer cuff abutment is placed (Fig.15). The lingual gingiva heals normal 5 months postop, immediately before cementation (Fig.16).
Return to Prevent Molar Periimplantitis (Protocols, Table) No Deviation Free hand Wife 纠纷
Xin Wei, DDS, PhD, MS 1st edition 07/02/2020, last revision 06/11/2021