



|
|
|
|
|
|
|
|
|
|
|
|
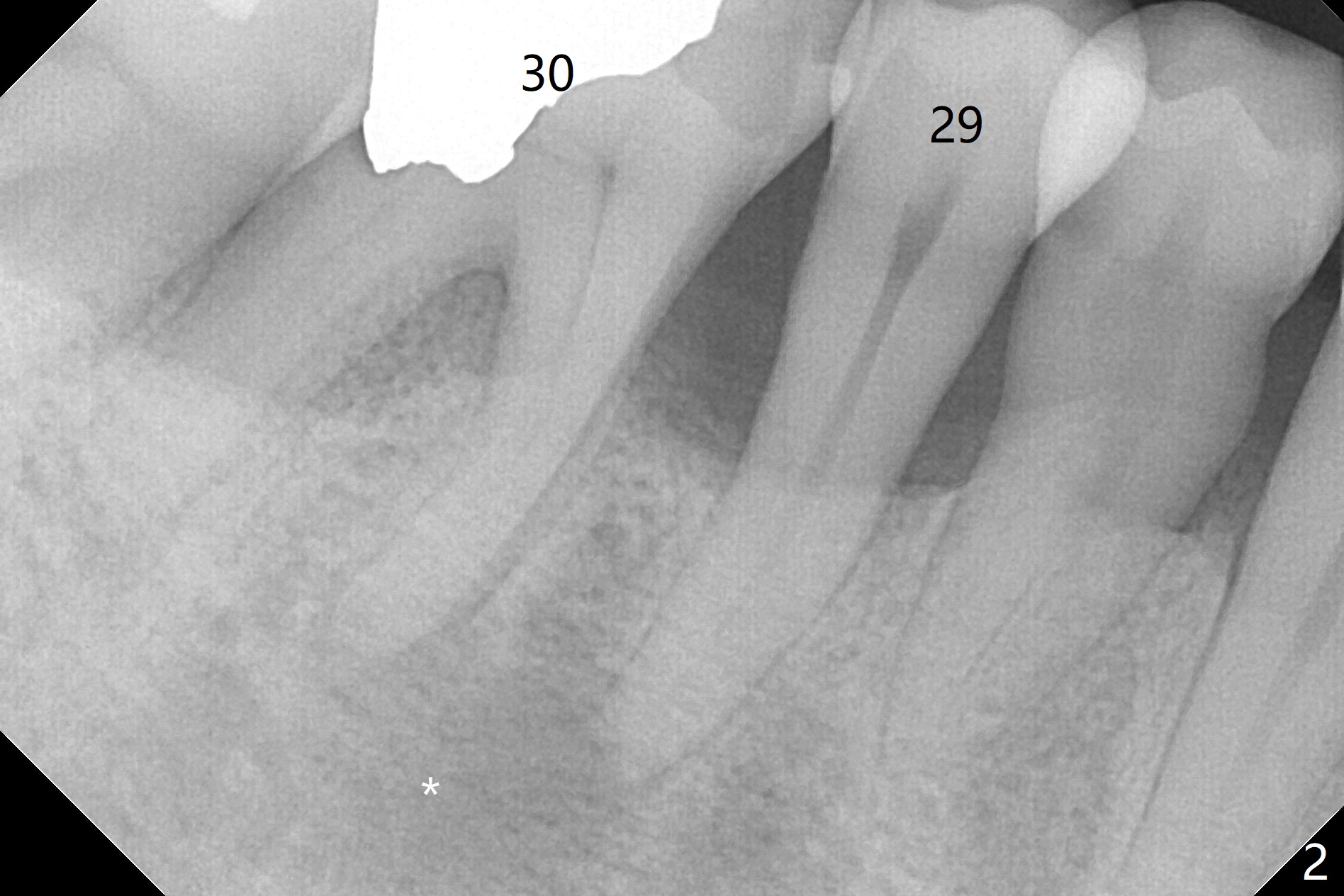
PARL Extends to Neighboring Tooth
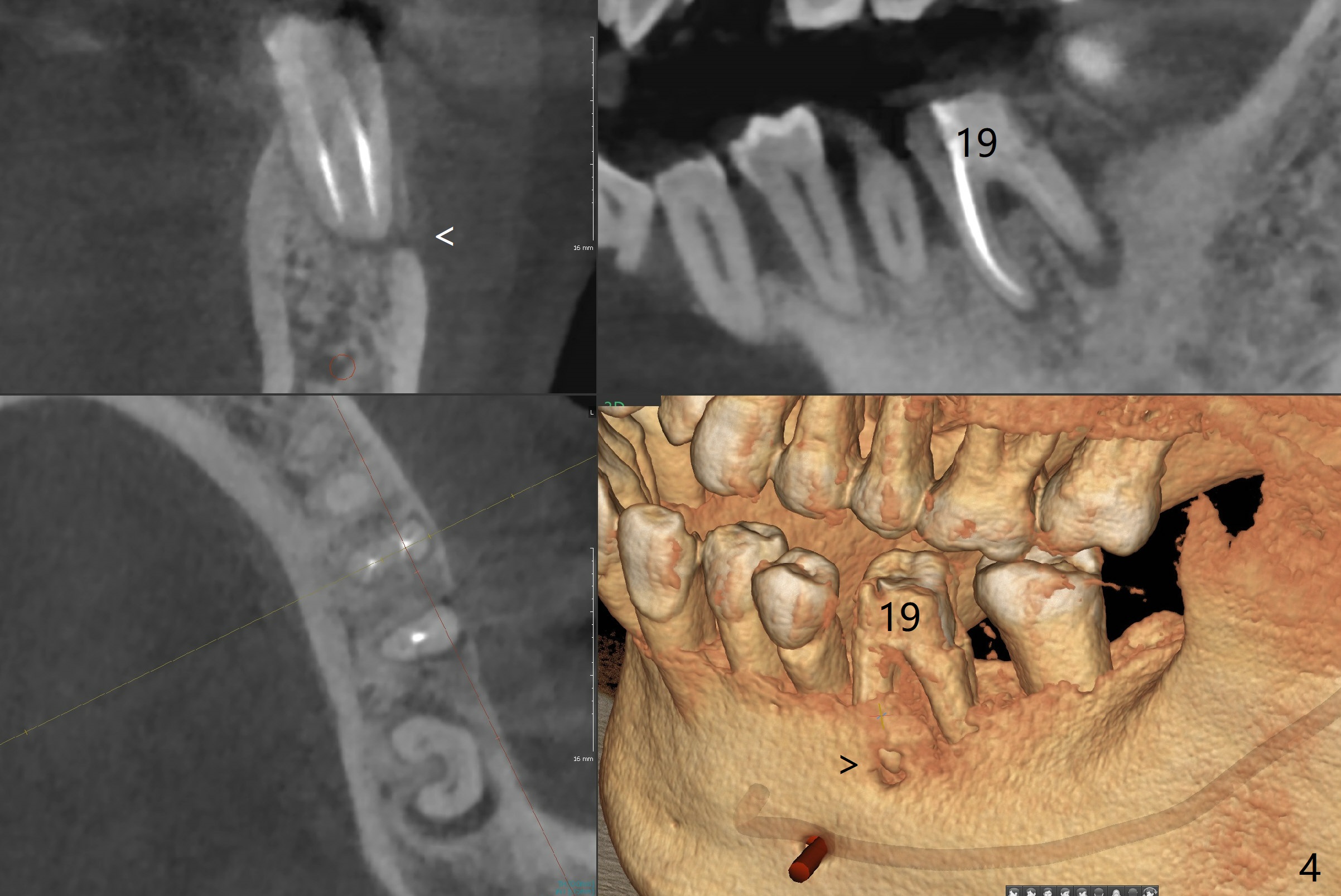
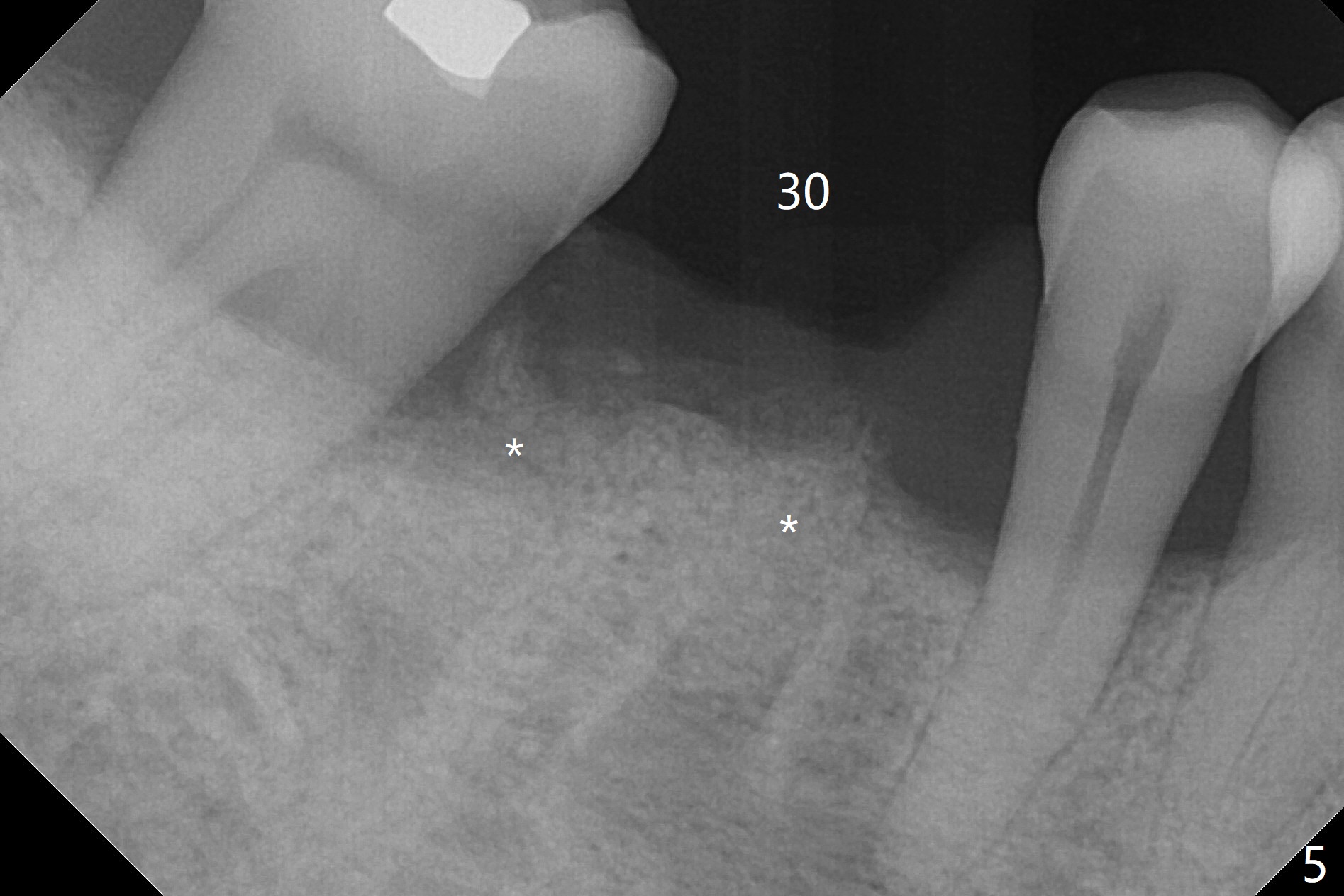
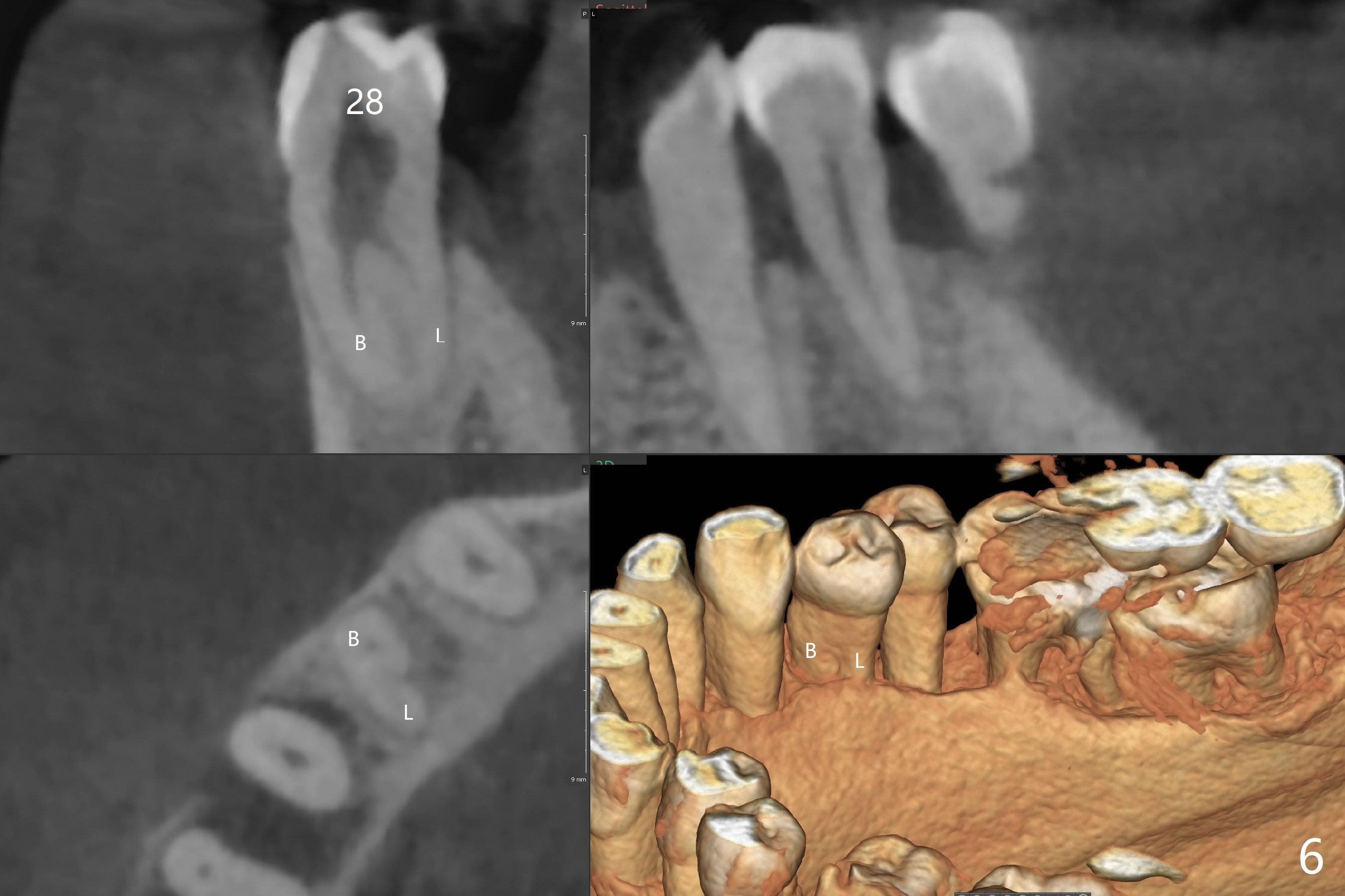
A 60-year-old man (smoker, 1/3 to 1/2 ppd) with large DO amalgam at #30 develops pain and mild swelling apparently apical to #29 (Fig.1-3). Both teeth (having fused PARL (periapical radiolucency) *) have mild percussion with the tooth #29 having higher mobility. CBCT shows apical defect (Fig.3 >). Three weeks earlier, the tooth #19 had much more severe infection with a similar apical defect (Fig.4 >). Combined with history of repeated infection associated with #30, the tooth is extracted with difficulty in obtain sound anesthesia. Socket preservation is performed instead of immediate implant (Fig.5 (*: Vanilla Graft)). CBCT makes it easy to diagnose 2 canals at #28 (Fig.6 as compared to Fig.2). Pain gradually decreases 3 days postop. In fact he has hypertension and smokes.
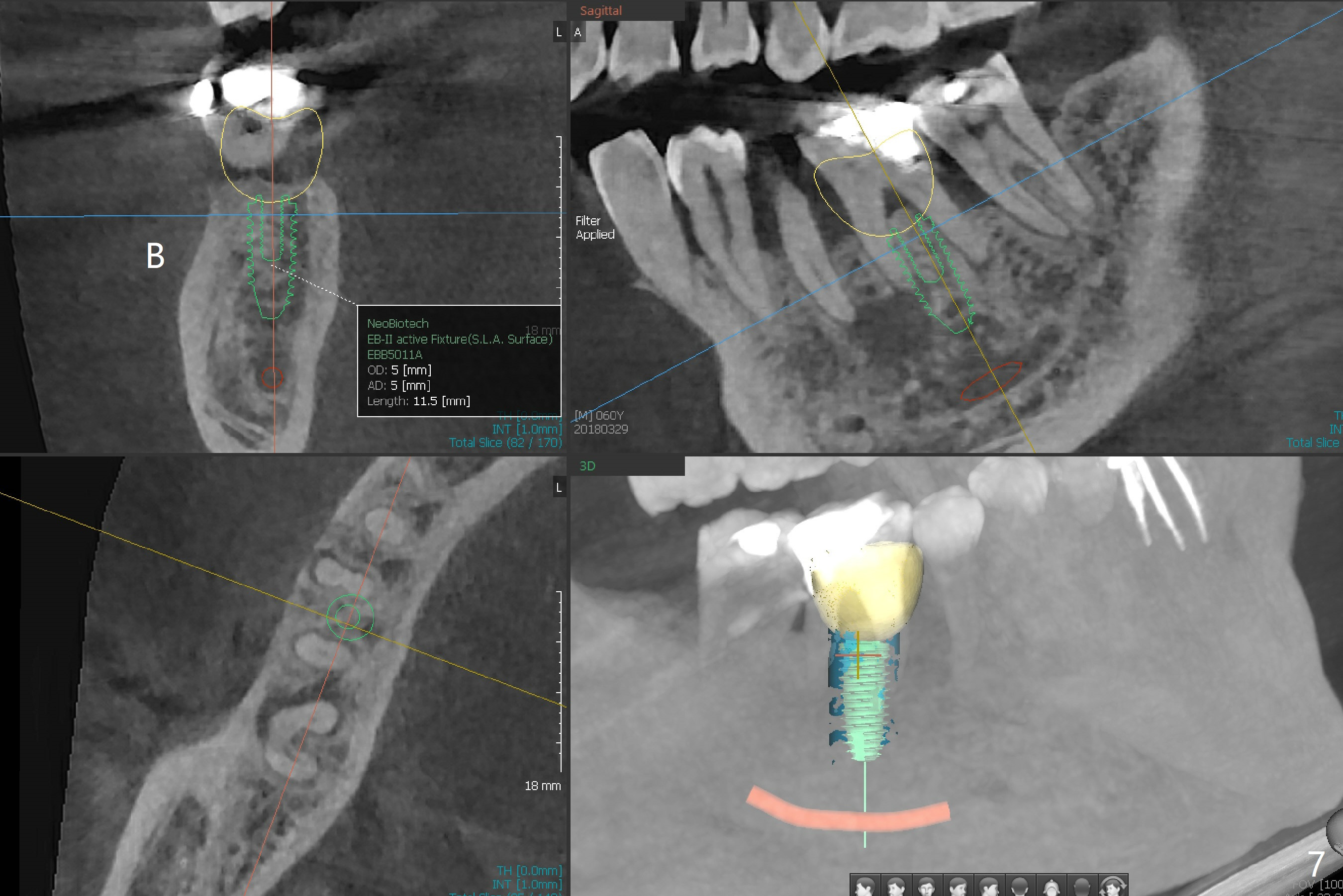
The bone seems to be wide to hold a 5x11.5 mm implant if it is placed early post extraction (Fig.7). Probably due to smoking, the socket appears to heal slow (Fig.8,9). There is mild palpation pain in the buccal vestibule. The tooth #29 remains mobile. The patient is scheduled to return for follow up in 2 months. A 5x5 cm scan is taken for the lower right posterior area for guided surgery.
Return to Lower Molar Immediate Implant, Armaments Placement Xin Wei, DDS, PhD, MS 1st edition 03/29/2018, last revision 07/08/2018