,30%20Ncm,%20nearly%201%20y%20post%20cem,%20food%20impaction.jpg)
|
|
|
|
|
|
|
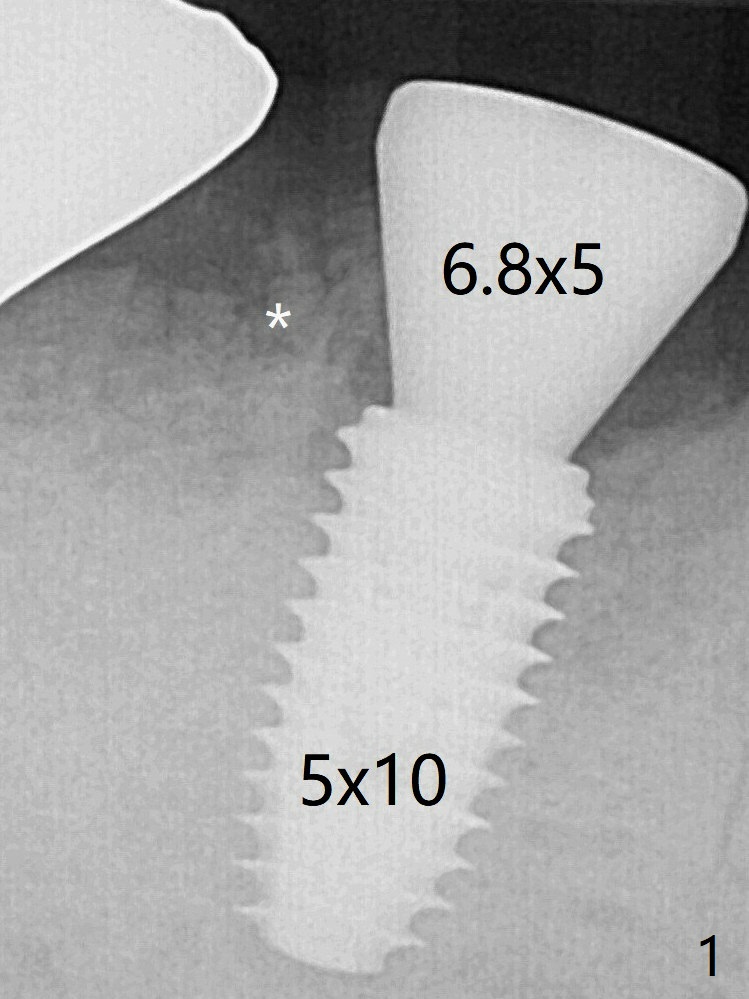
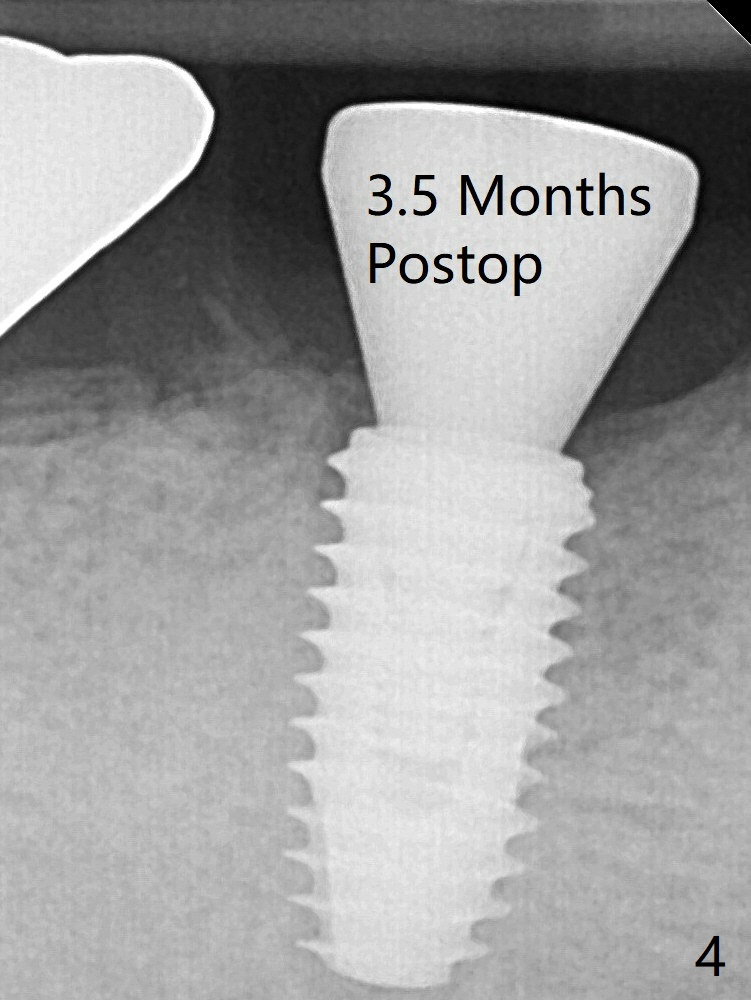
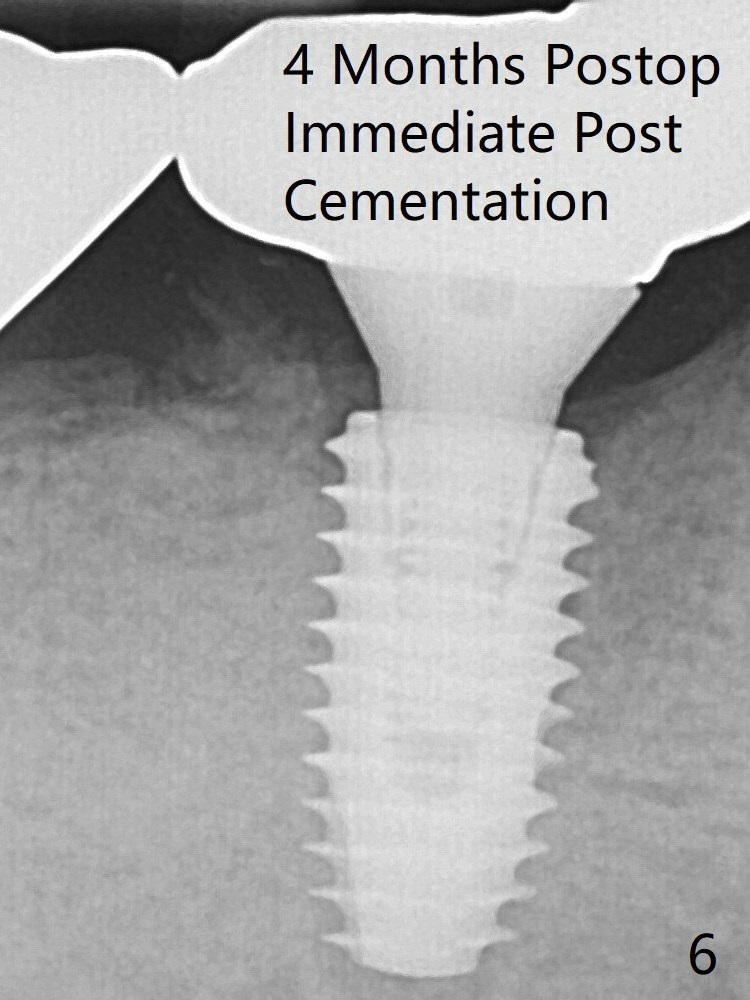
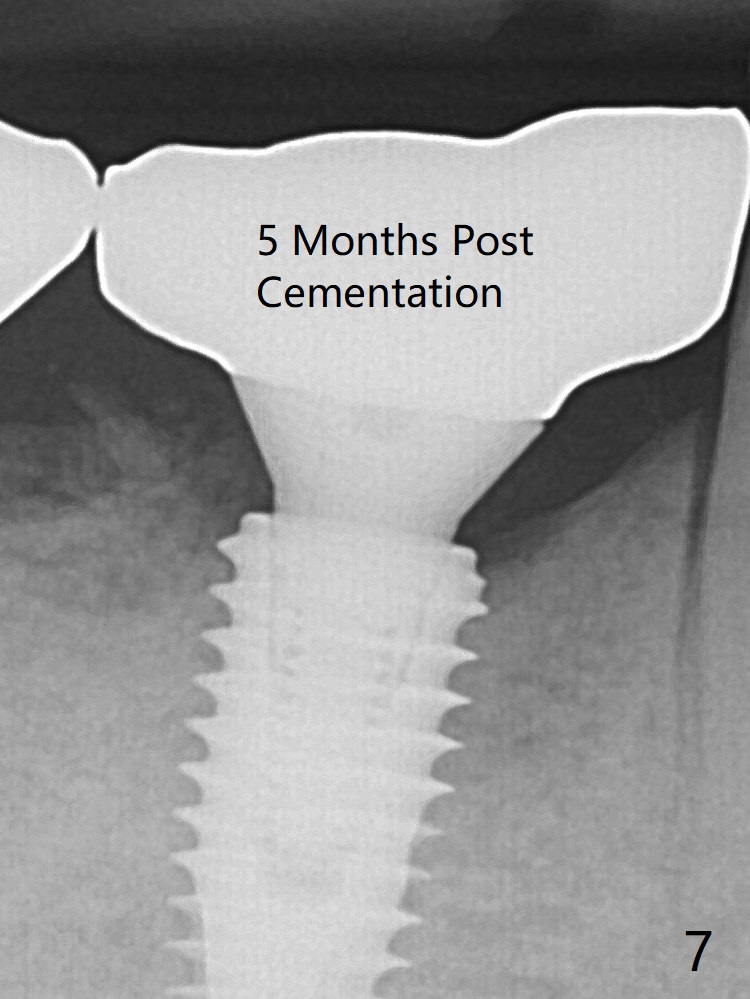
To reduce heat-induced bone necrosis at #19, osteotomy is conducted slowly with copious irrigation with cold saline. Bone density is felt while a 5x10 mm implant is being placed after using cortical tap to the 2nd line of the implant driver. The implant needs to be reverse torqued several times before reaching its final depth (Fig.1 (~50 Ncm)). Since the residual roots are superficially positioned, the immediate implant looks as a delayed one. Although the implant is placed mesial to the septum clinically, its position in X-ray seems to be normal. Because of severe wear and lack of vertical height, a 6.8x5 mm healing abutment is placed. Retention of bone graft placed in the distal socket (Fig.1 *) is maintained by spreading setting acrylic into the edentulous undercut areas. The bone graft placed in the distal socket appears to have been converted to the native bone 3.5 months and 4 months postop (Fig.4,6). There is no bone loss 5 months post cementation, although the abutment screw has been loose (Fig.7). The patient complains of food impaction nearly 1 year post cementation. The mesial and distal contacts of #30 crowns are light. When the abutment/crown is removed, there is implant well contamination (food debris). It appears that the previous abutment (5.7x4(2) mm, Fig.6,7) is incompletely seated. When a smaller abutment is placed and torqued at 30 Ncm, it is seated fully (Fig.9 (<: no gap)). New impression is taken. If there is food impaction distal to the new crown, the distal crestal bone should be removed with lab closure of the embrasure.
Xin Wei, DDS, PhD, MS 1st edition 02/22/2020, last revision 02/22/2020