%20after%20DL%20bone%20trimming.jpg)

,%20latter%20subgingival%20distal.jpg)
%20incomplete%20seating,%20distal%20interference.jpg)
.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|||
Do not Press Hard on Distal End Guide
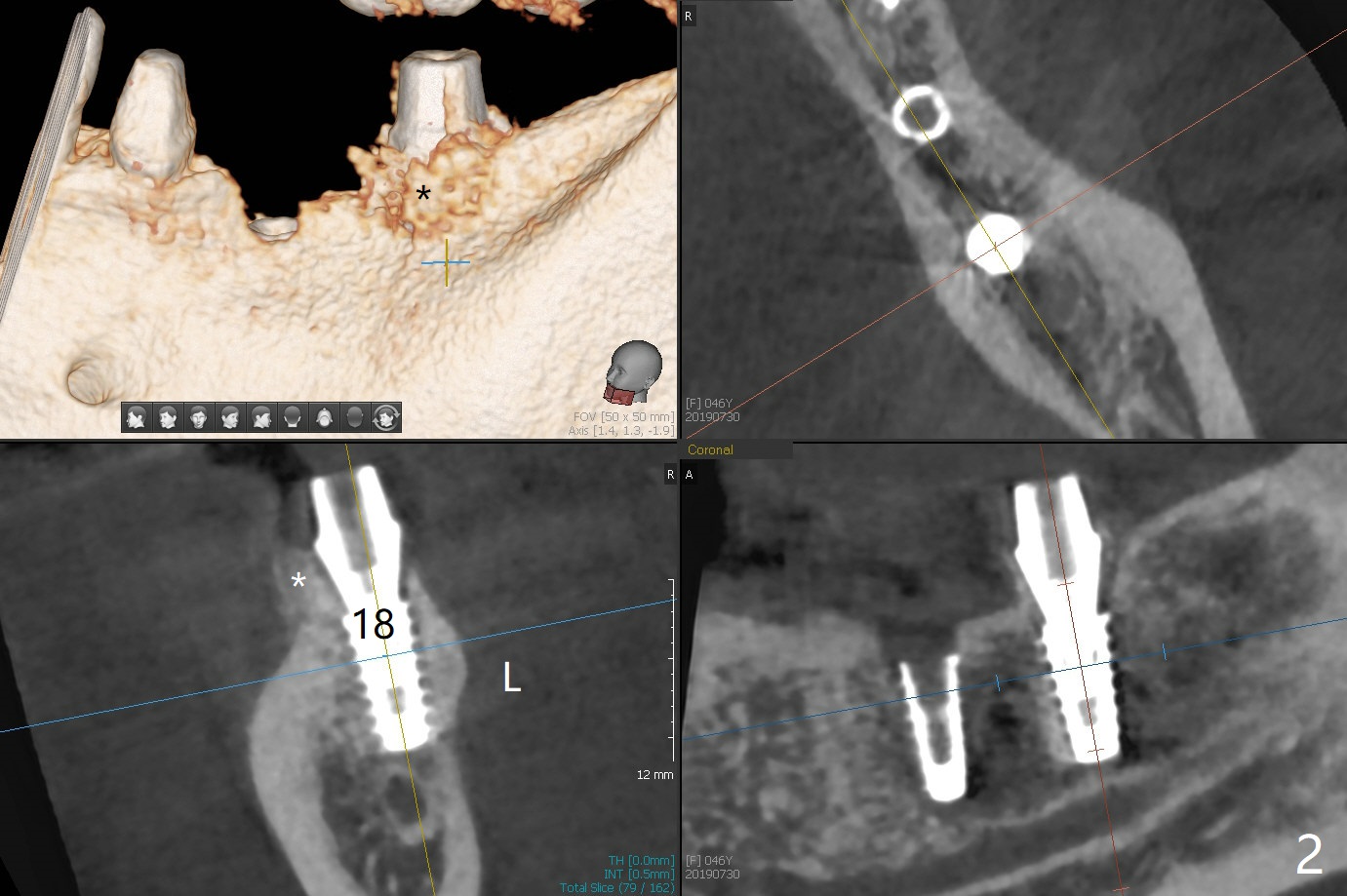
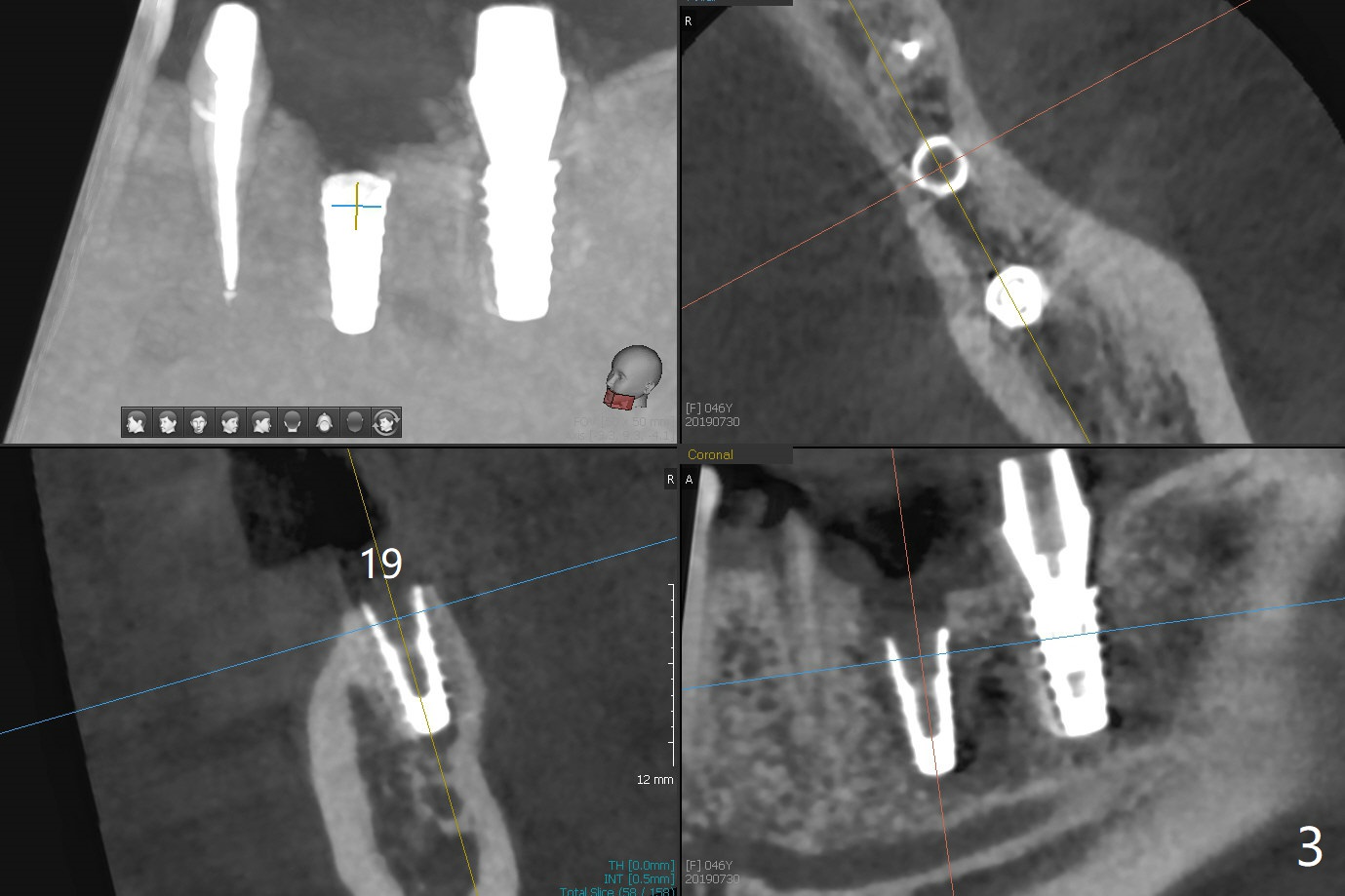
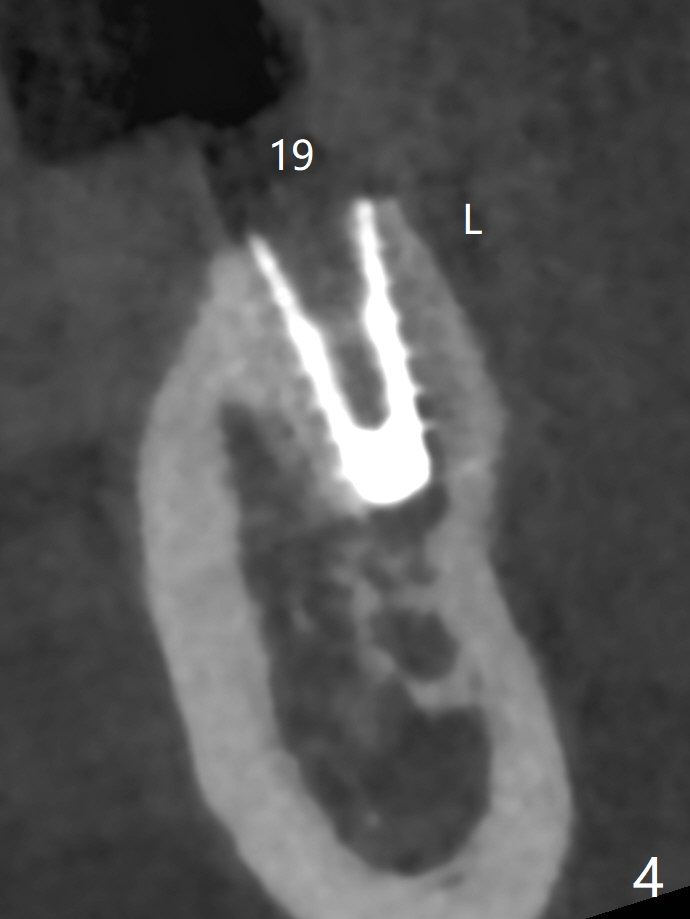
The female woman is afraid of pain. After placement of 4x9 mm FC implant at #19, infiltration anesthesia is not enough for osteotomy at #18. Block anesthesia is added. When a 5x9 mm FC implant is placed in the osteotomy (designed for 5x8.5 mm IS one), it is close to the Inferior Alveolar Canal (Fig.1 red dashed line; Fig.2 (*: bone graft with PRF)). The third contributing factor is the pressure upon the distal end of the distal end guide while osteotomy. A few hours later, the patient reports no paresthesia. The implant placement level and trajectory are normal at #18 and 19 (Fig.3-5). To check pair abutment seating with 30 Ncm torque, PA is taken after removal of healing abutments 4 months postop (Fig.6-8). First the cuff of the abutment is short, subgingival distal of #18 (Fig.6 * (gingiva)). When an abutment with longer cuff is placed, it appears to be close to the distal crestal bone (Fig.7 *). Finally a smaller abutment seams to be appropriate (Fig.8). Retrospectively the larger abutment (6.5x4(4) mm) is incompletely seated initially (Fig.1 with gap).
Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Trajectory II, Next Case Xin Wei, DDS, PhD, MS 1st edition 07/30/2019, last revision 12/08/2019