

.jpg)

|
|
|
|
|
|
|
|
|
|
Infiltration
Anesthesia
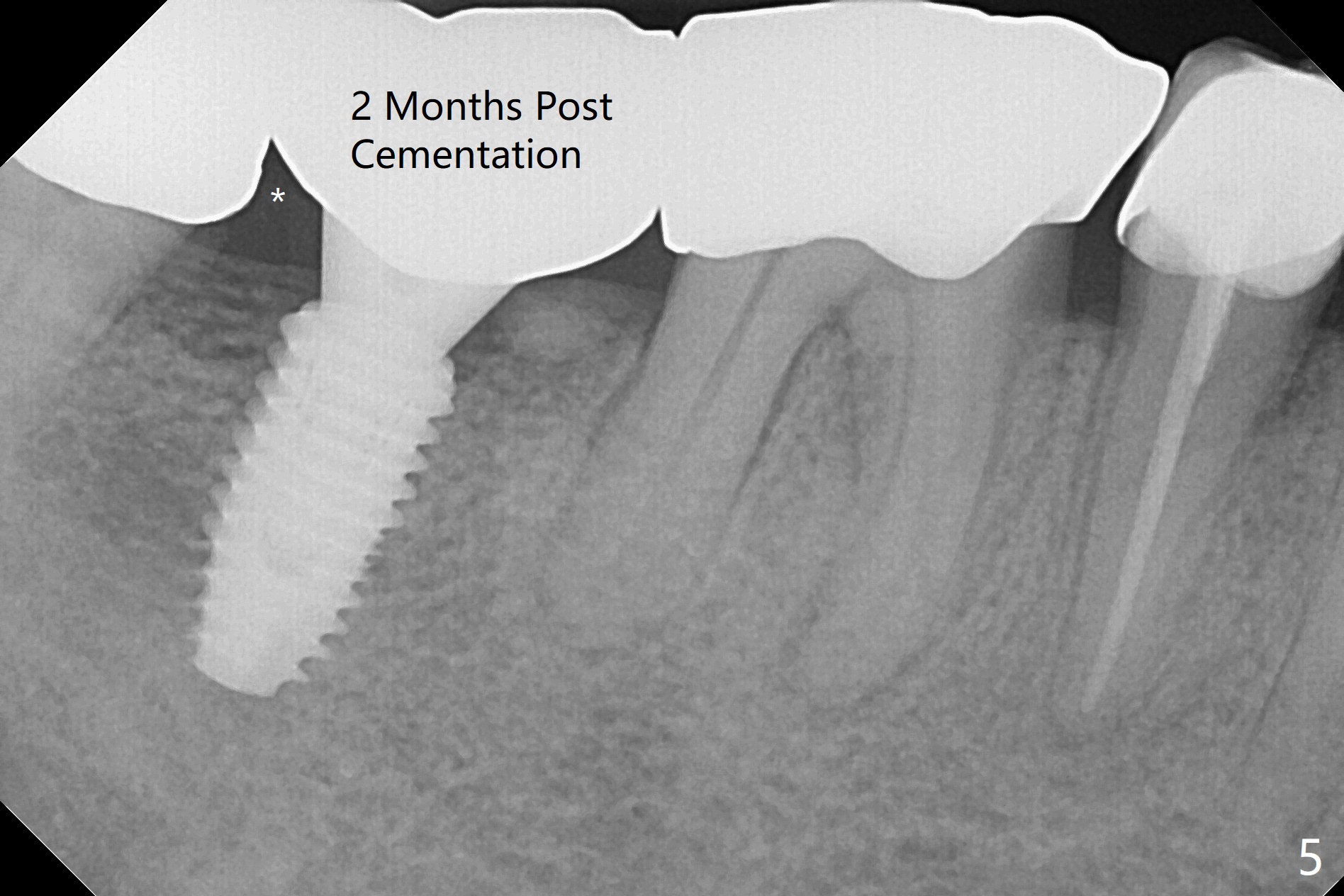
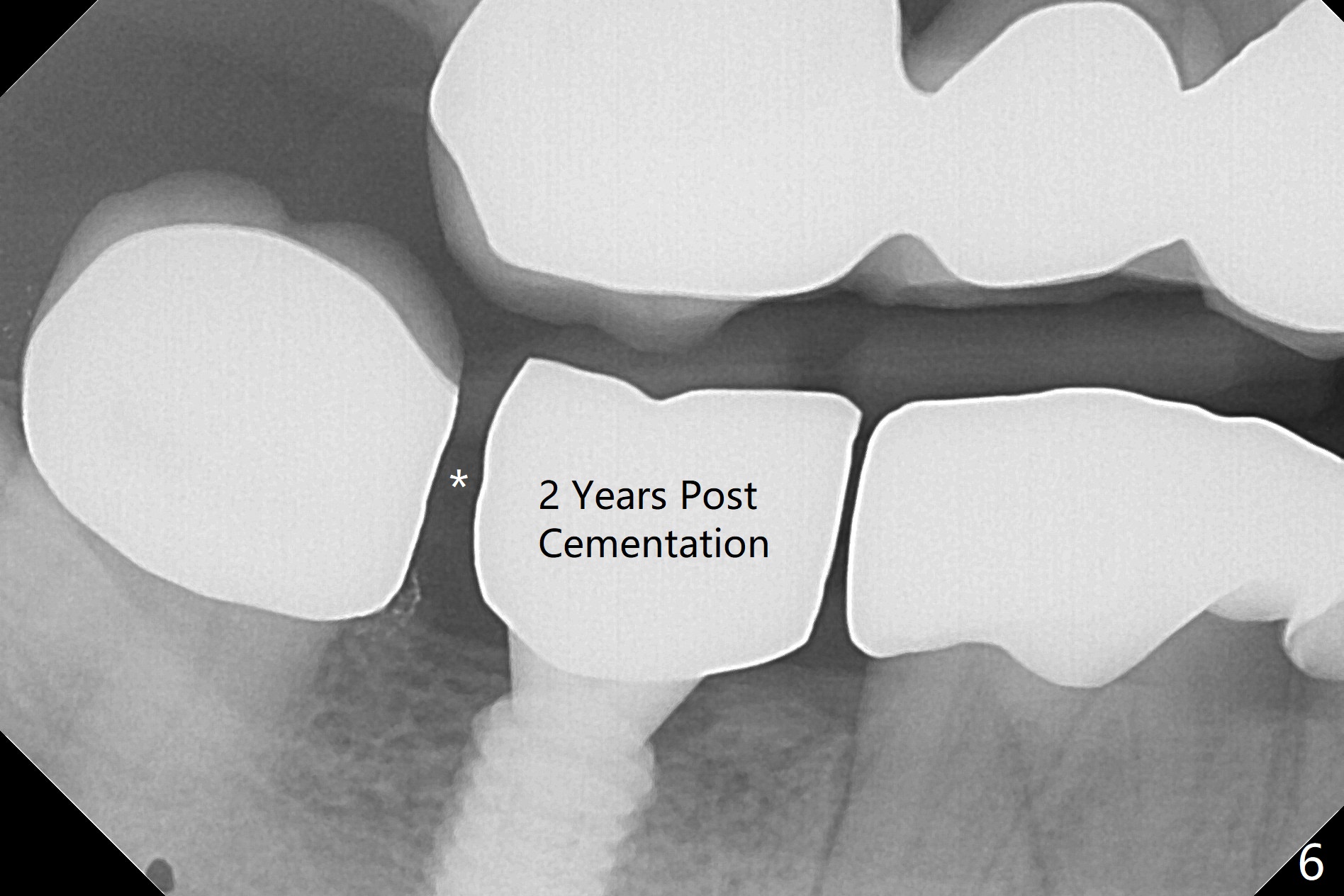
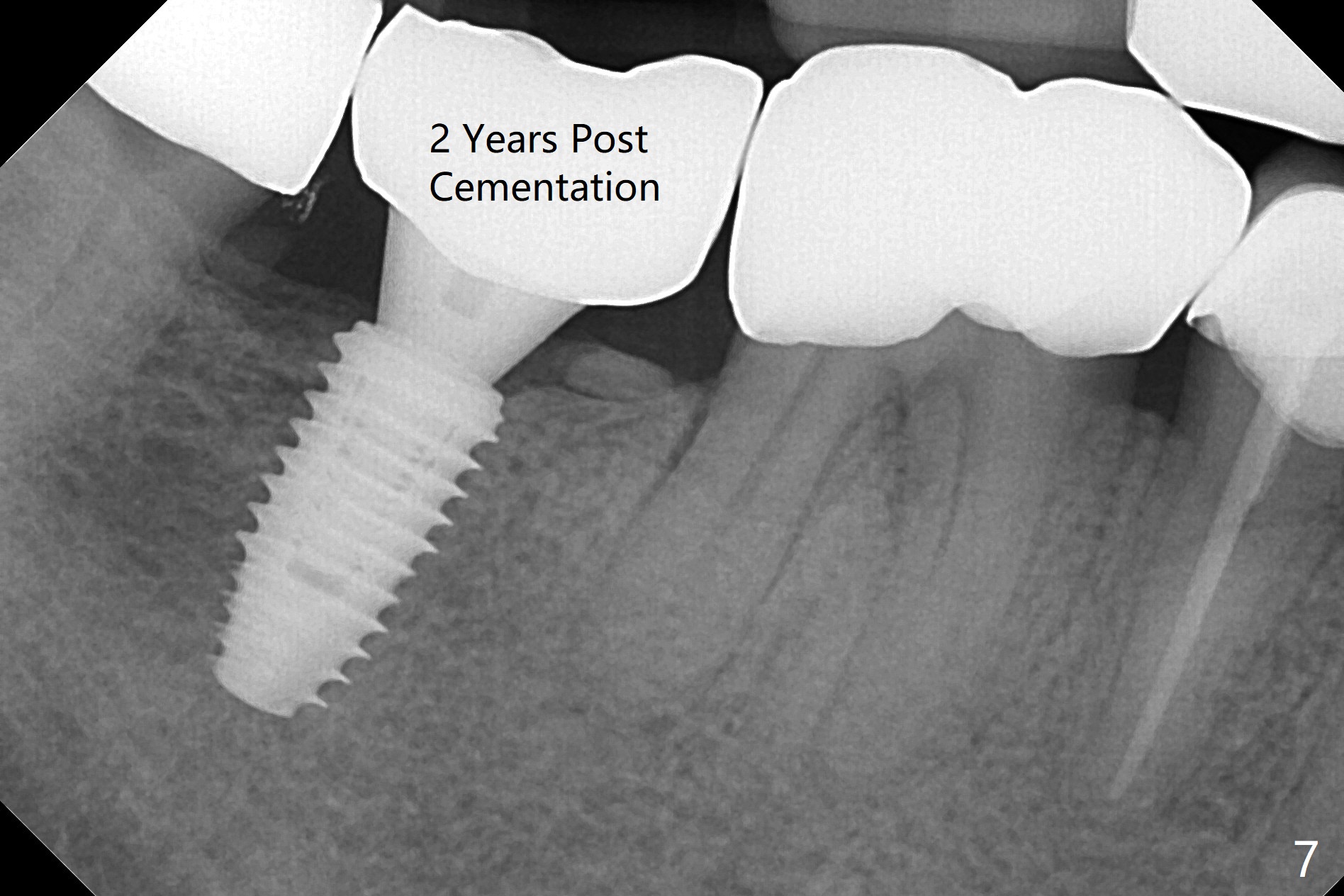
The edentulous ridge at #31 is anesthetized with one carpule of Lidocaine in an infiltration manner for guided surgery (Fig.1,2). In comparison, two or 3 carpules of Lidocaine are required for anesthesia for delayed implant placement without guide. It suggests that guided surgery is associated with less pain. Besides, the implant placed with guide has good trajectory and depth in a timely manner (Fig.3). Since the patient is a heavy bruxer with dislodgement of #30 provisional and #19 abutment screw loosening, a 5.7x4(3) mm cementation abutment is placed immediately so that a splinted provisional is fabricated for #30 and 31 for better retention. However, the gingiva around the implant at #31 is unhealthy 3 months postop (Fig.4). After impression, the provisional at #31 is sectioned without recementation for better oral hygiene. The distal gingival embrasure is large, associated with food impaction (Fig.5). Two years post cementation, the proximal contacts are trimmed (Fig.6 *) for pick up impression for crown repair. The implant and abutment contact is clearly shown with change in X-ray projection (Fig.7). When the new crown with flattened proximal contacts is being seated, it is tight mainly distal. After distal proximal contact adjustment, the crown is recemented without taking out crown/abutment for residual cement removal, because they may be unable to be completely seated because of the flattened larger proximal contacts (hand torque before impression).
Return to Lower Molar Immediate Implant, Trajectory Torque
Xin Wei, DDS, PhD, MS 1st edition 01/28/2019, last revision 06/27/2021