
,%20Vanilla.jpg)
.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
4 mm Stopper from IS Kit
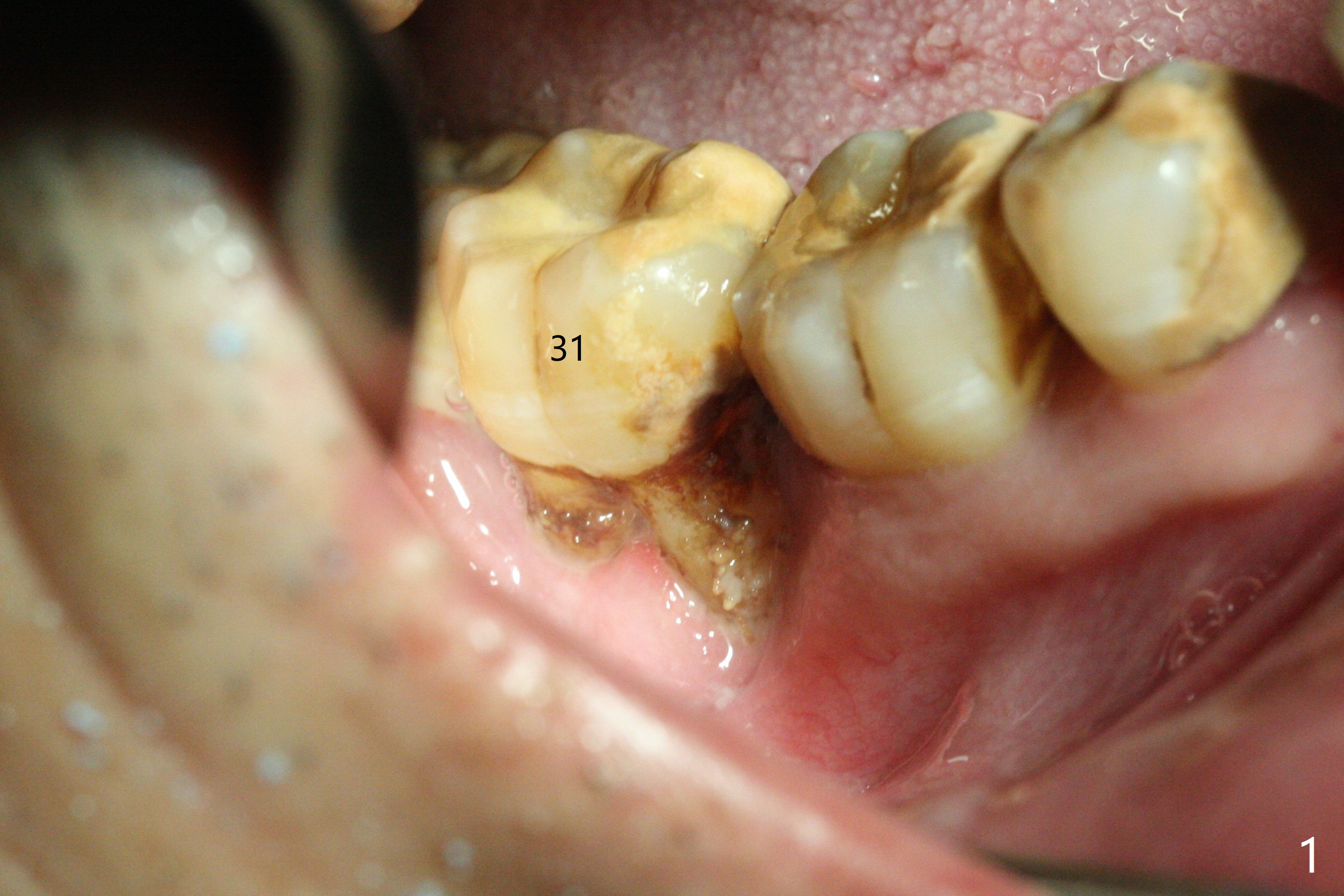
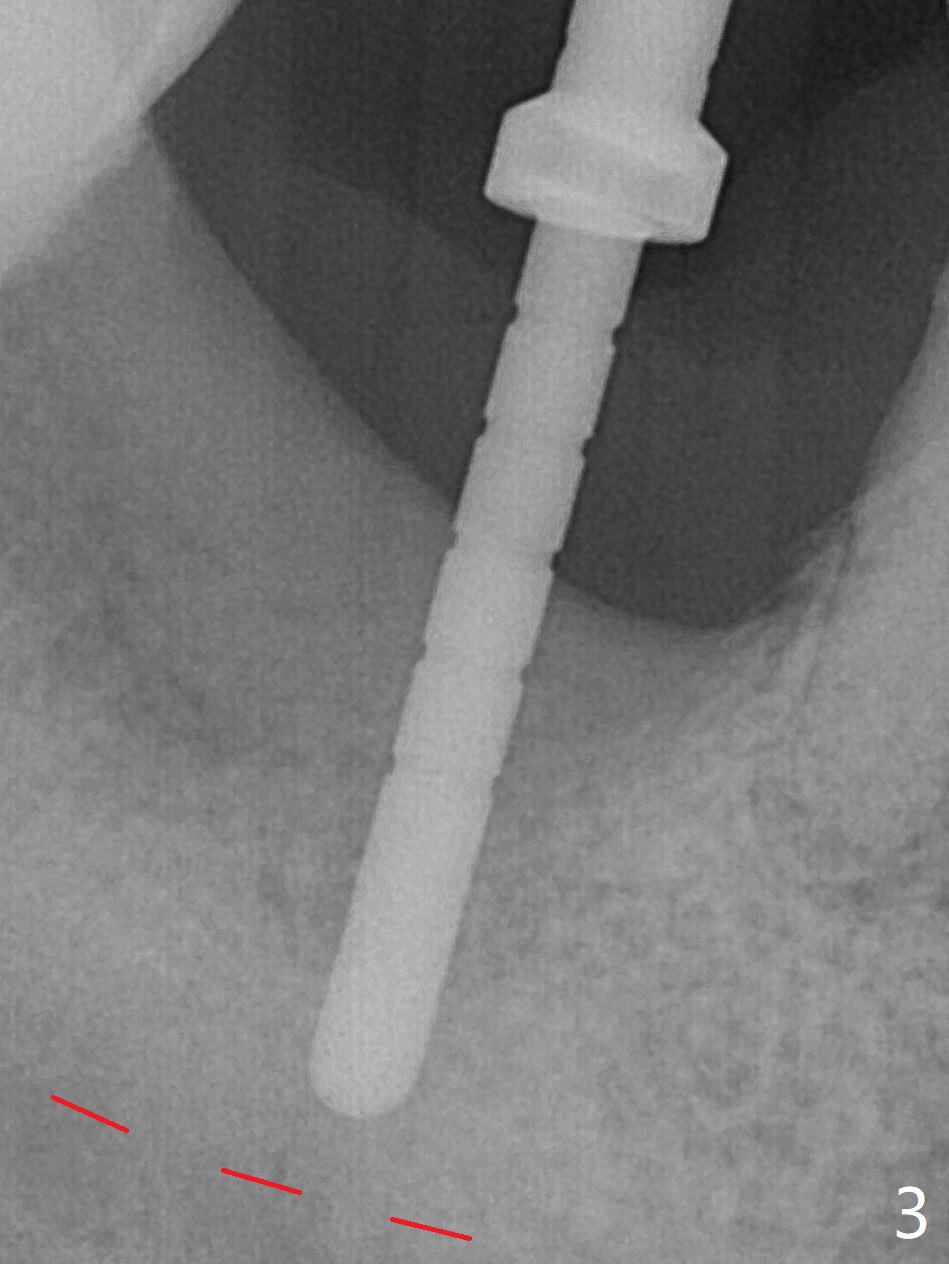
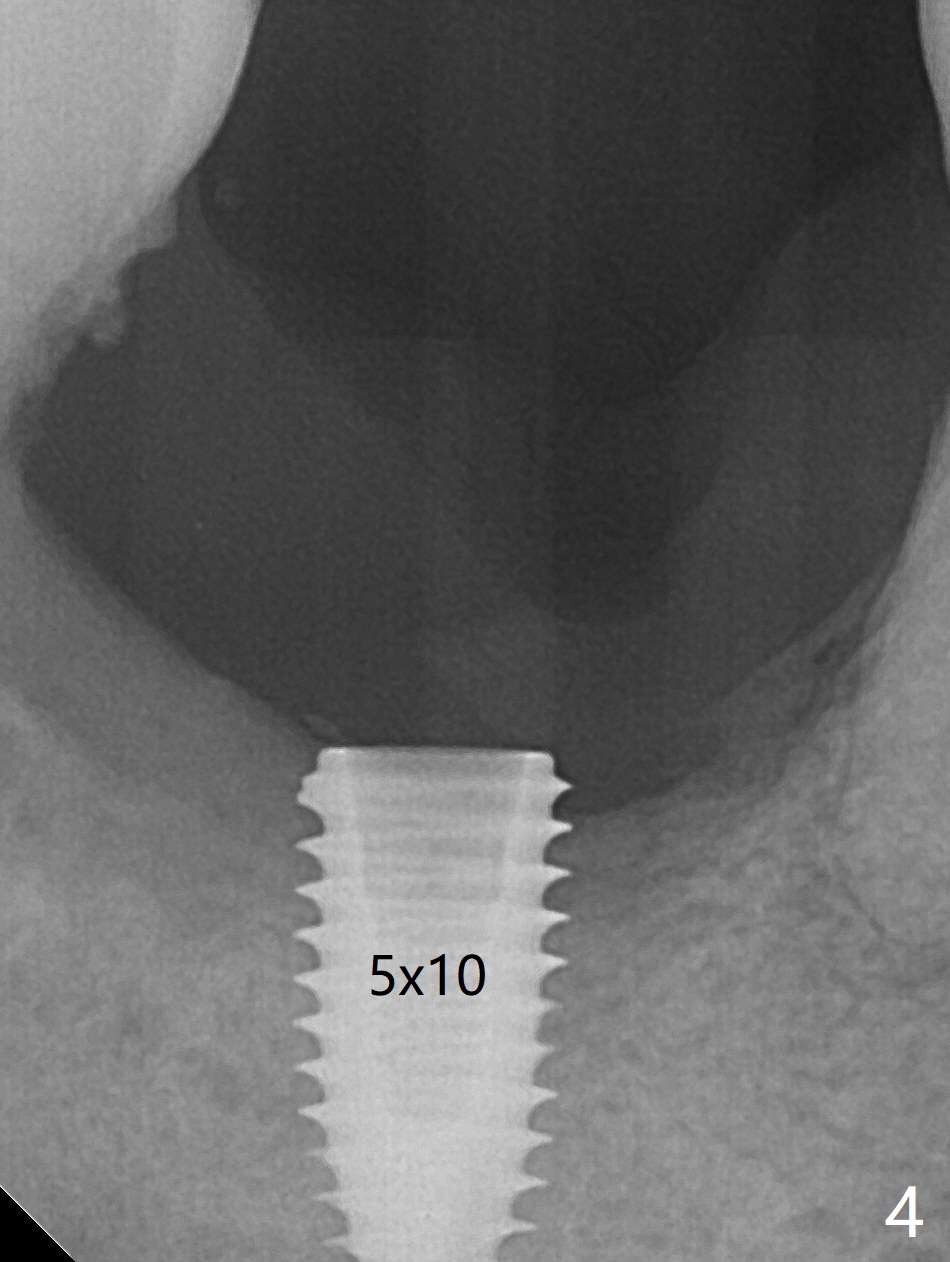
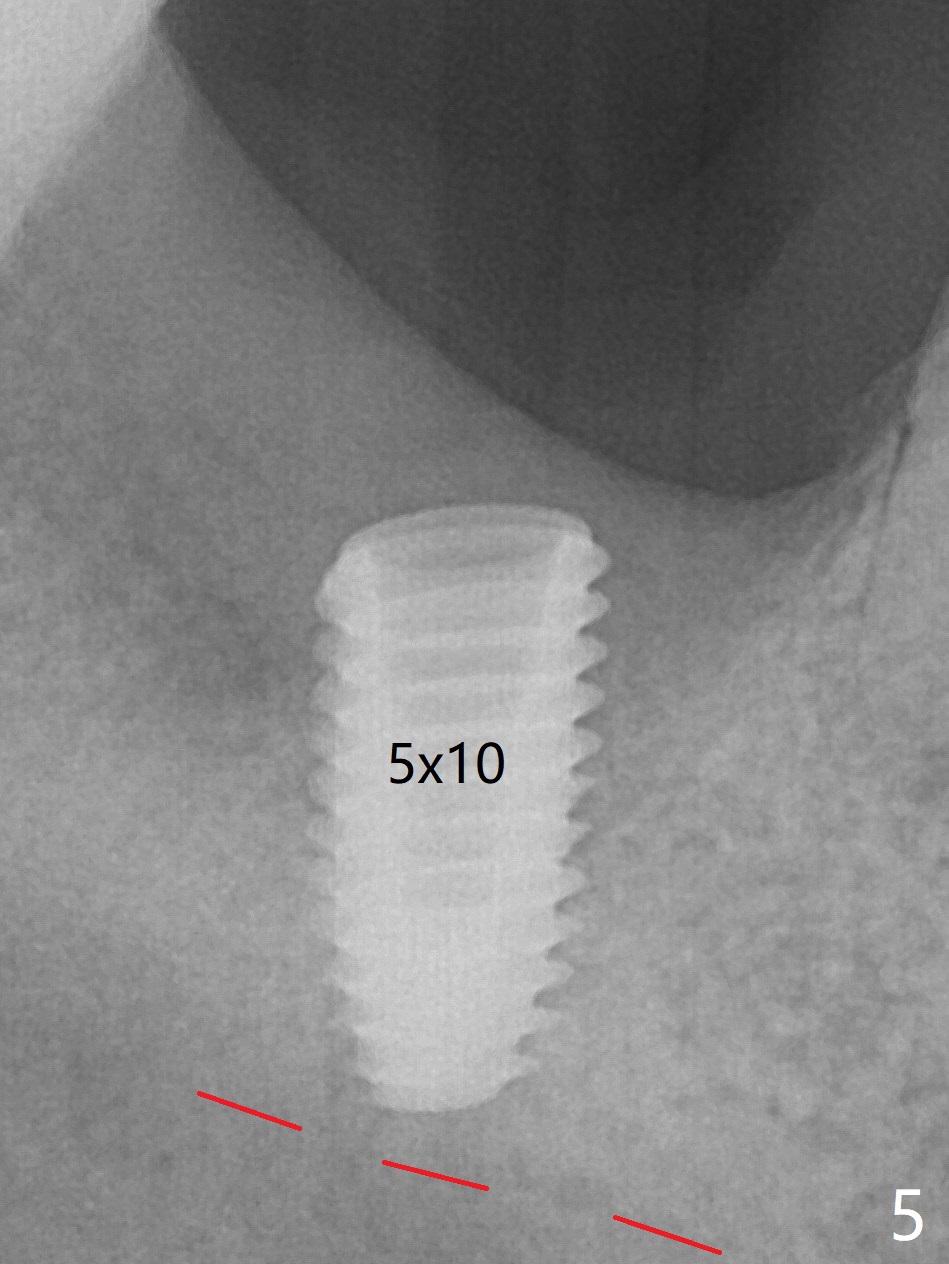
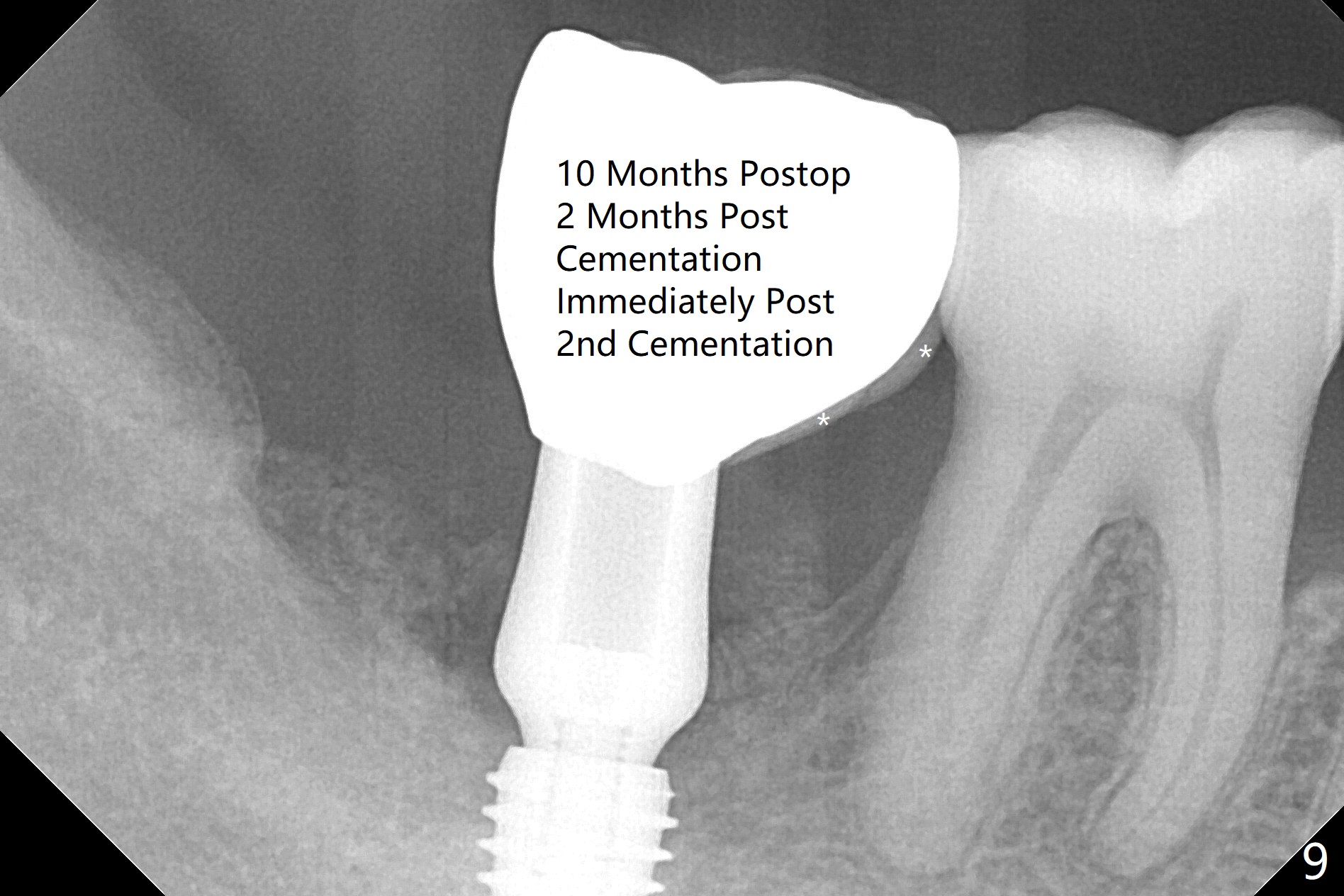
The affected tooth (#31, Fig.1) has severe buccal gingival recession with mobility III. After extraction and removal of granulation tissue, osteotomy is initiated in the middle of the fused socket using IS drills with 4 mm stopper (Fig.2,3). Following sequential osteotomy until 4 mm drill, a 4.5x10 mm IS dummy implant does not achieve primary stability, whereas 5x10 mm one does (Fig.4,5). Due to limited bone height confirmed intraoperatively, a shorter UF implant is placed with insertion torque 30 Ncm (Fig.6,7) with ~ 4.5 mm implant threads exposed coronally. After placing a 6.5x5(5) mm abutment, Vanilla Graft (*) and PRF membrane and collagen plug, an immediate provisional is fabricated to close the remaining socket. The tooth #32 is kept initially to increase the stability of the provisional and removed 8 day postop because of discomfort. A 5.5(2.5) mm mill abutment is changed to 3 months postop. The implant seems ready for impression 6 months postop (Fig.8). The bone graft remains around the apical portion of the mill abutment with apparently new bone formation around the coronal portion of the implant10 months postop (Fig.9); porcelain (*) has been added to close the mesial gingival embrasure and proximal contact gap. Due to unfavorable crown/implant ratio and poor trajectory, the crown/abutment becomes loose once post 1st cementation. Guided surgery would avoid the trajectory isssue.
Upper Lower Molar Full Arch Immediate Implant, Prevent Molar Periimplantitis, Armaments Xin Wei, DDS, PhD, MS 1st Version 03/16/2018, Last Update 01/13/2019