
|
|
|
|
|
|
|
|
Control Implant Spacing
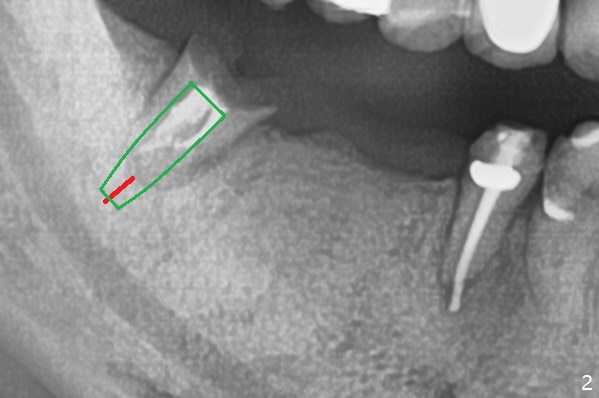
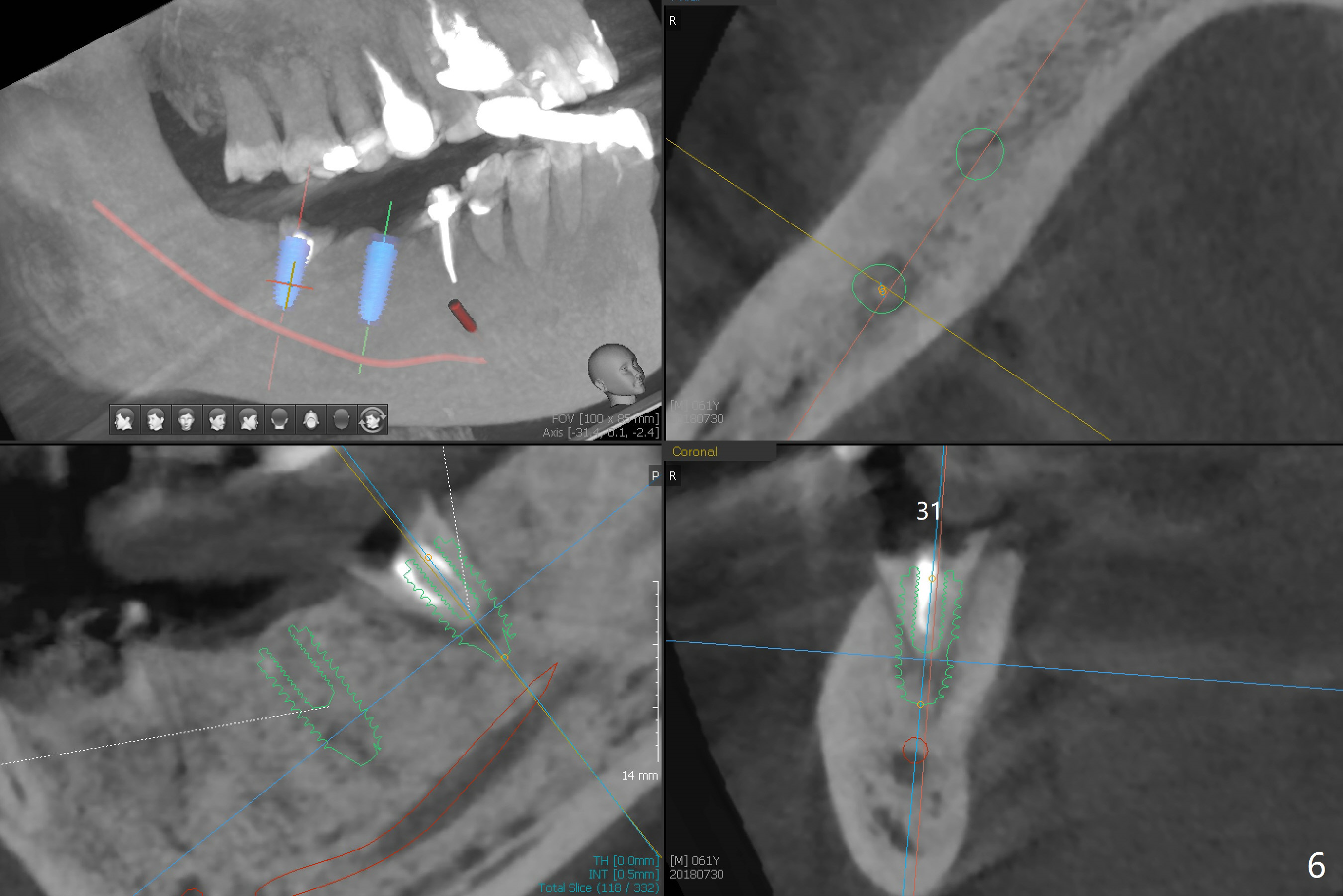
A 60-year-old man has lost a lower right FPD (Fig.1). The ridge at #30 is wide. To control implant spacing, PVS impression will be taken for guided surgery. Use the residual roots at #31 as a distal anchor tooth to finish implant placement at #30. After extraction, use implant anchor at #30 and finish implant placement at #31. Or 3-4 mm osteotomy will be initiated in the native bone using stopper for free hand (Fig.2 red line). An implant will be place ~ 1 mm subcrestal (green outline). Ask the lab to fabricate a stent for provisional with ~ 1 mm occlusal clearance.
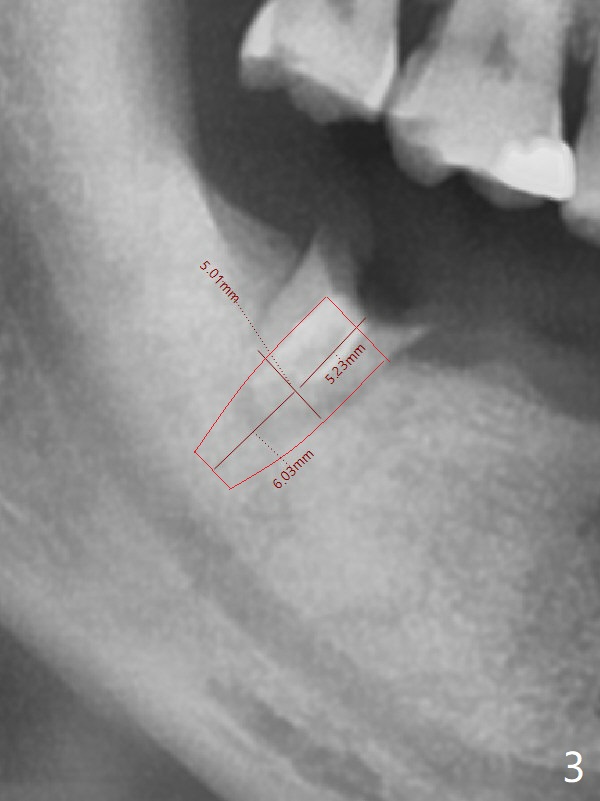
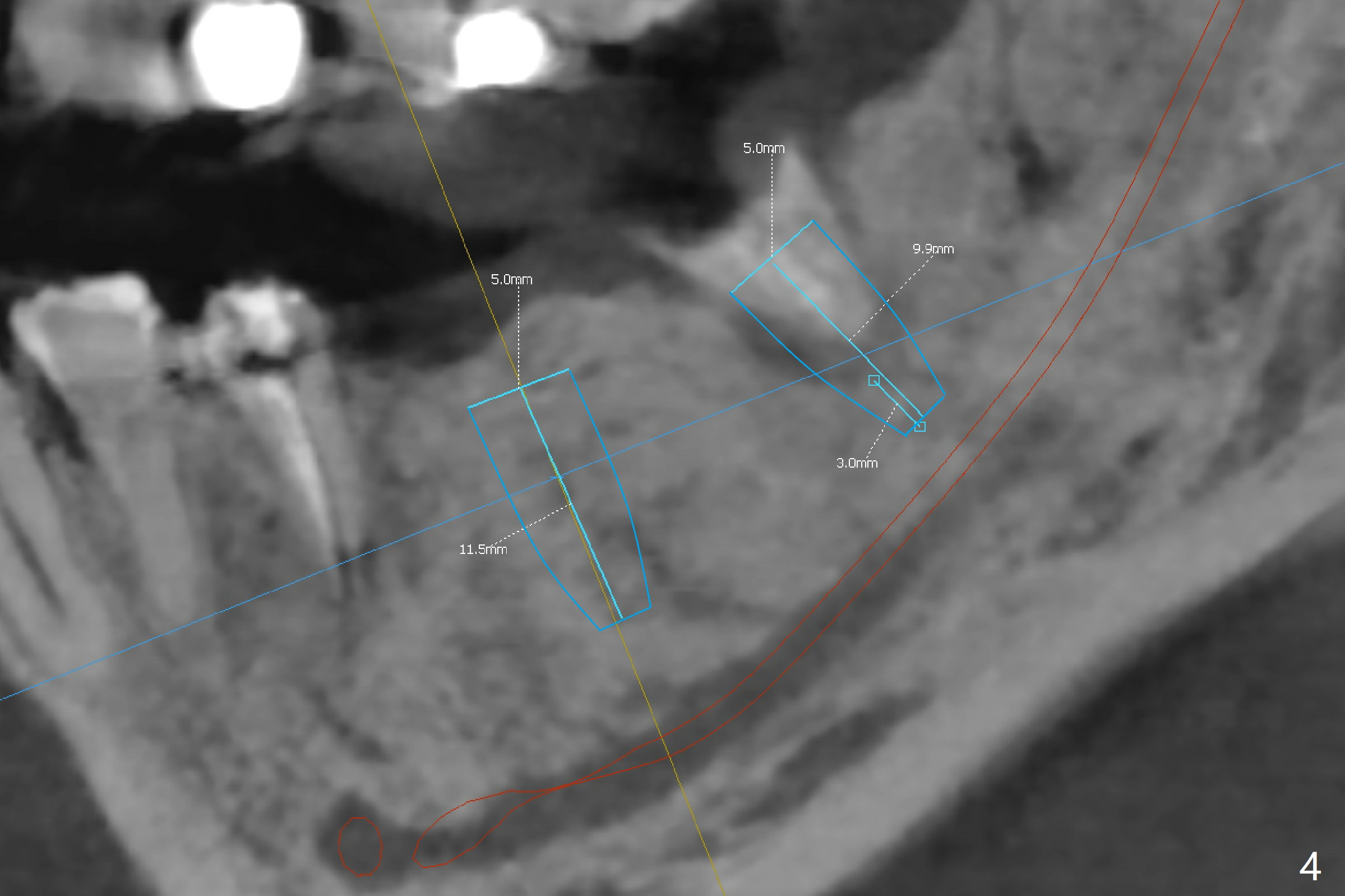
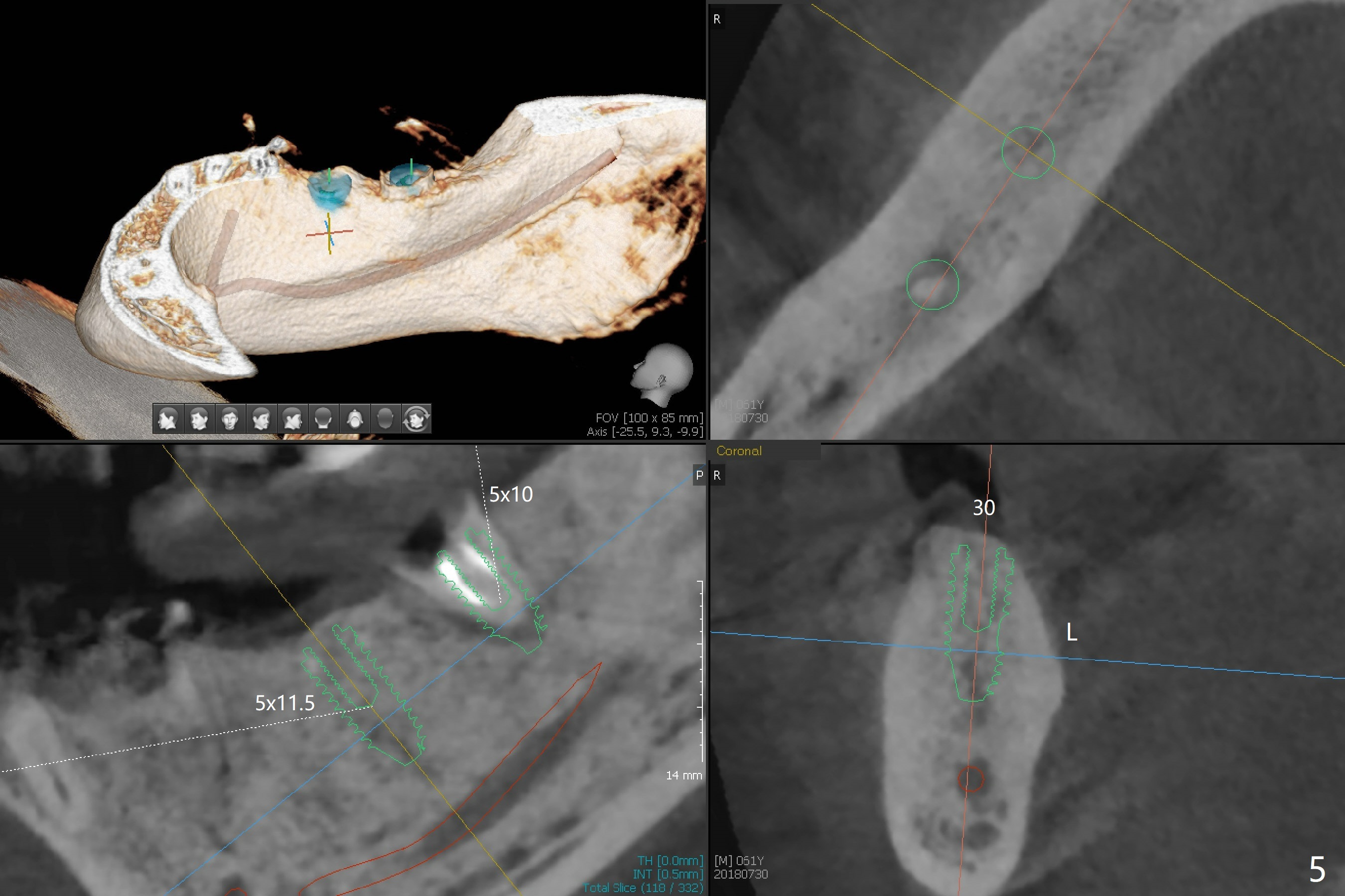
My question is have you measured the how much remaining bones are left at the extraction socket. How much bone depth is left after the root extraction? Do you think the implant could get enough fixation after the extraction? Jennifer It is a good question. As today's CT indicates (07/30/2018), there is ~ 3 mm bone for primary stability with ~ 1 mm clearance (Fig.3-6). Because of the tapered implant, ~5 mm of the implant will be able to contact the native bone if the implant is lingually placed (Fig.6). If you feel it too much a risk, still make a guide for #31 so that an anchor pin can be placed at #31 residual roots for fixation (a new idea?). Make sure that the distal portion of the guide contacts the #31 residual root stump for stability, which is superior to a guide resting on the soft tissue. I have had experience placing implants free hand in this situation. The guide will be great help. I will use judgment in surgery. The worst scenario is socket preservation. Thanks for consideration and design.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Armaments, No Antibiotic Xin Wei, DDS, PhD, MS 1st edition 04/22/2018, last revision 08/23/2018