

'.jpg)


|
|
|
|
|
|
|
|
|
|
|
|||
Severe Periodontitis Dictates Deep Placement of Implant
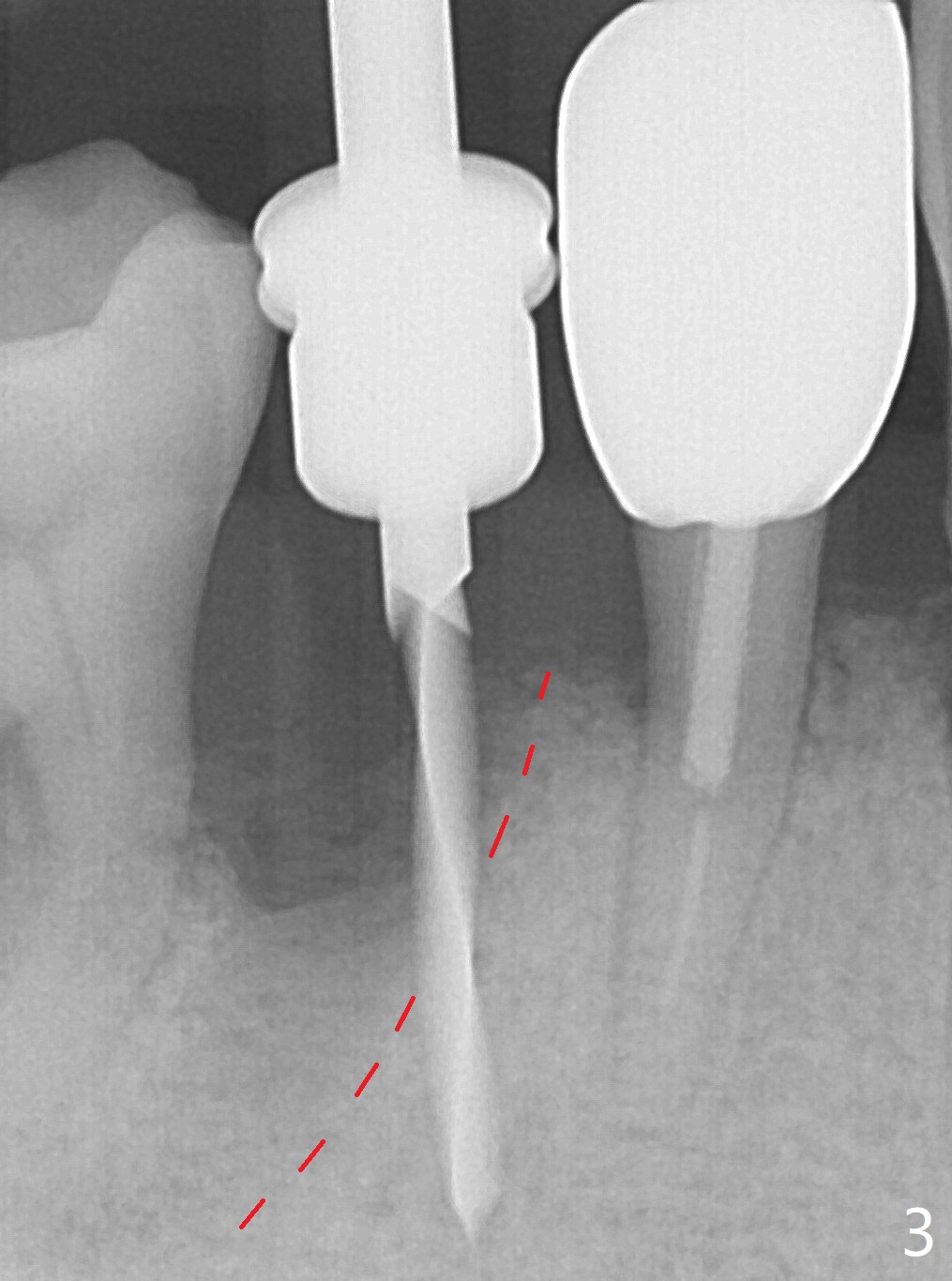
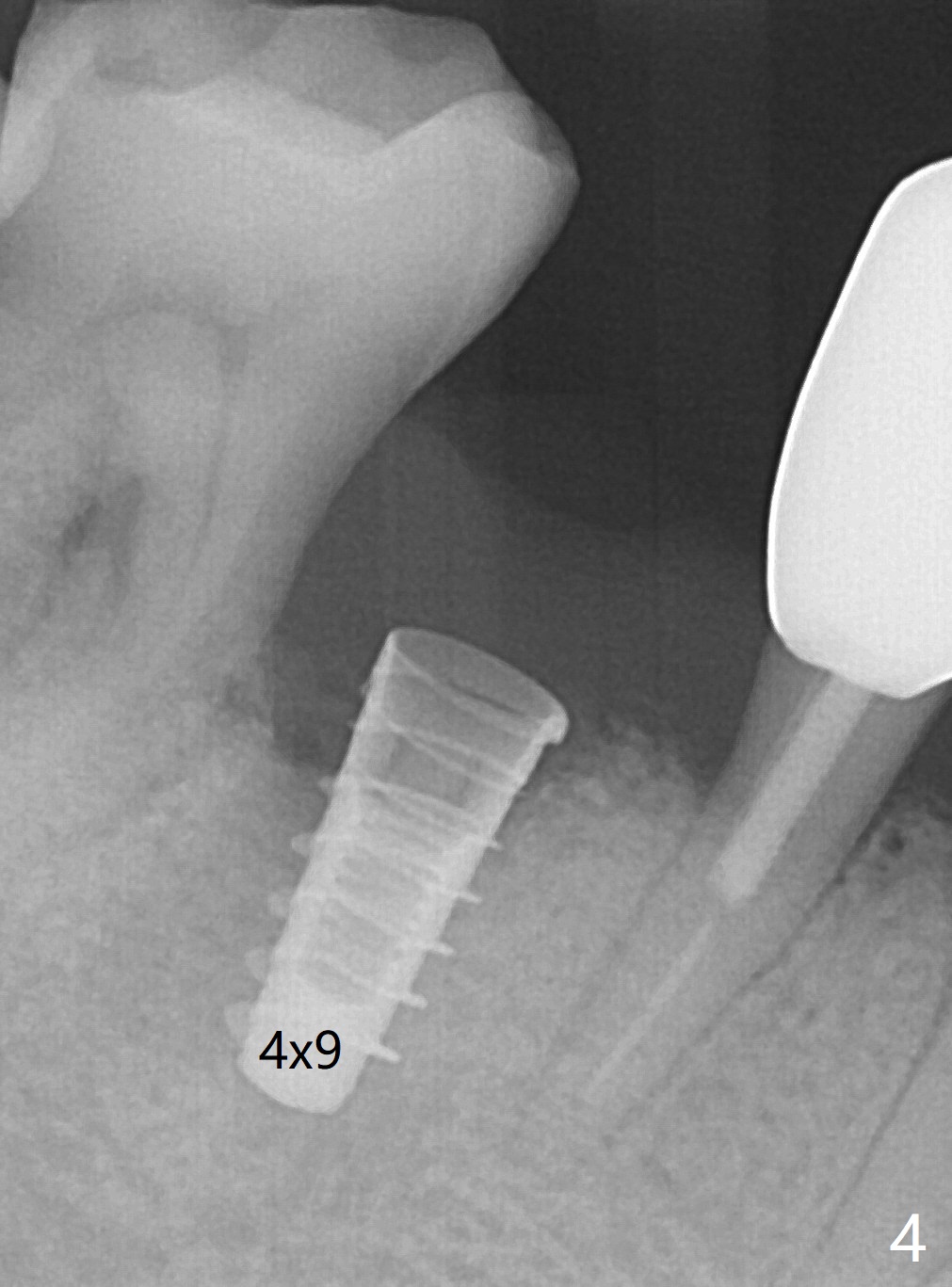
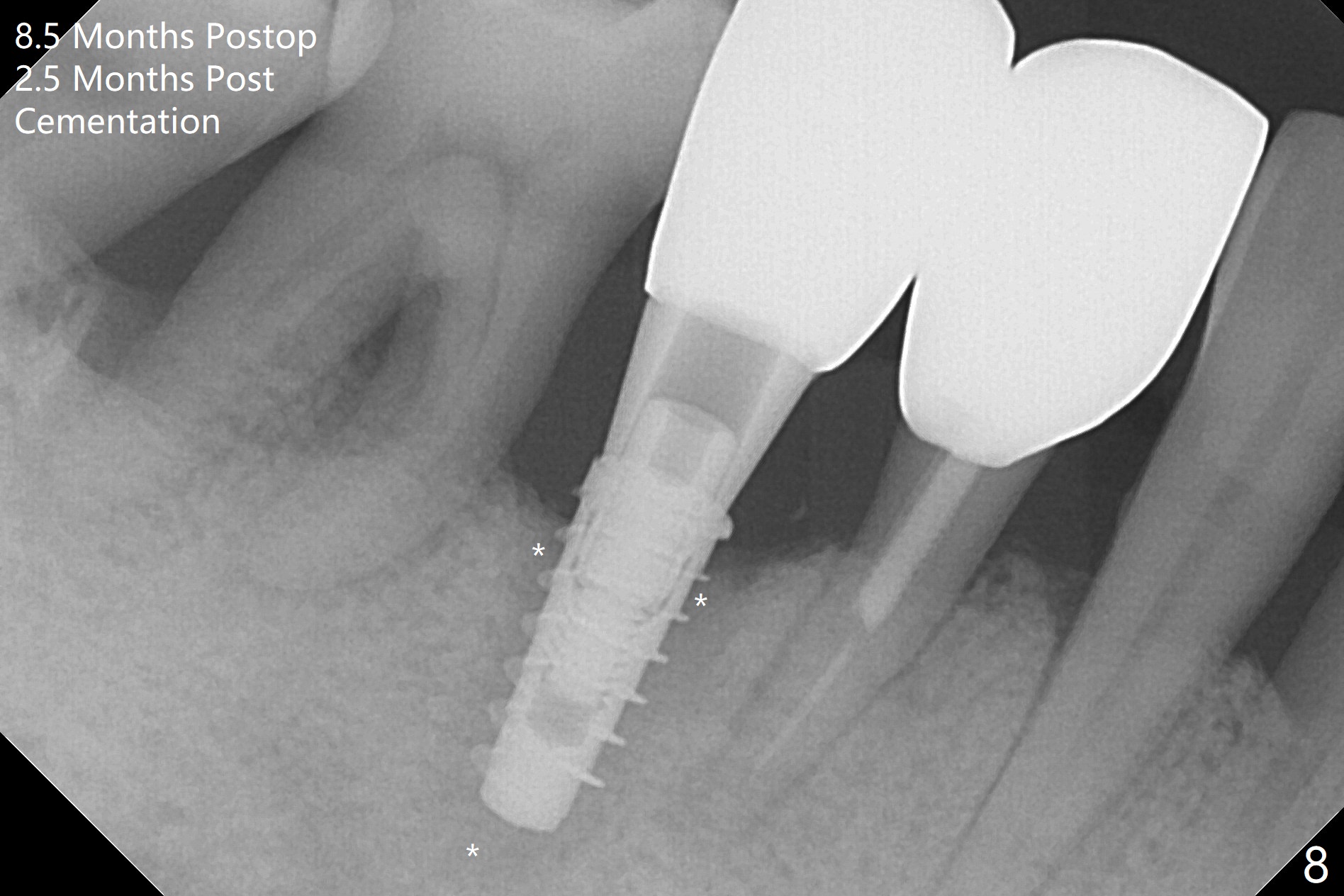
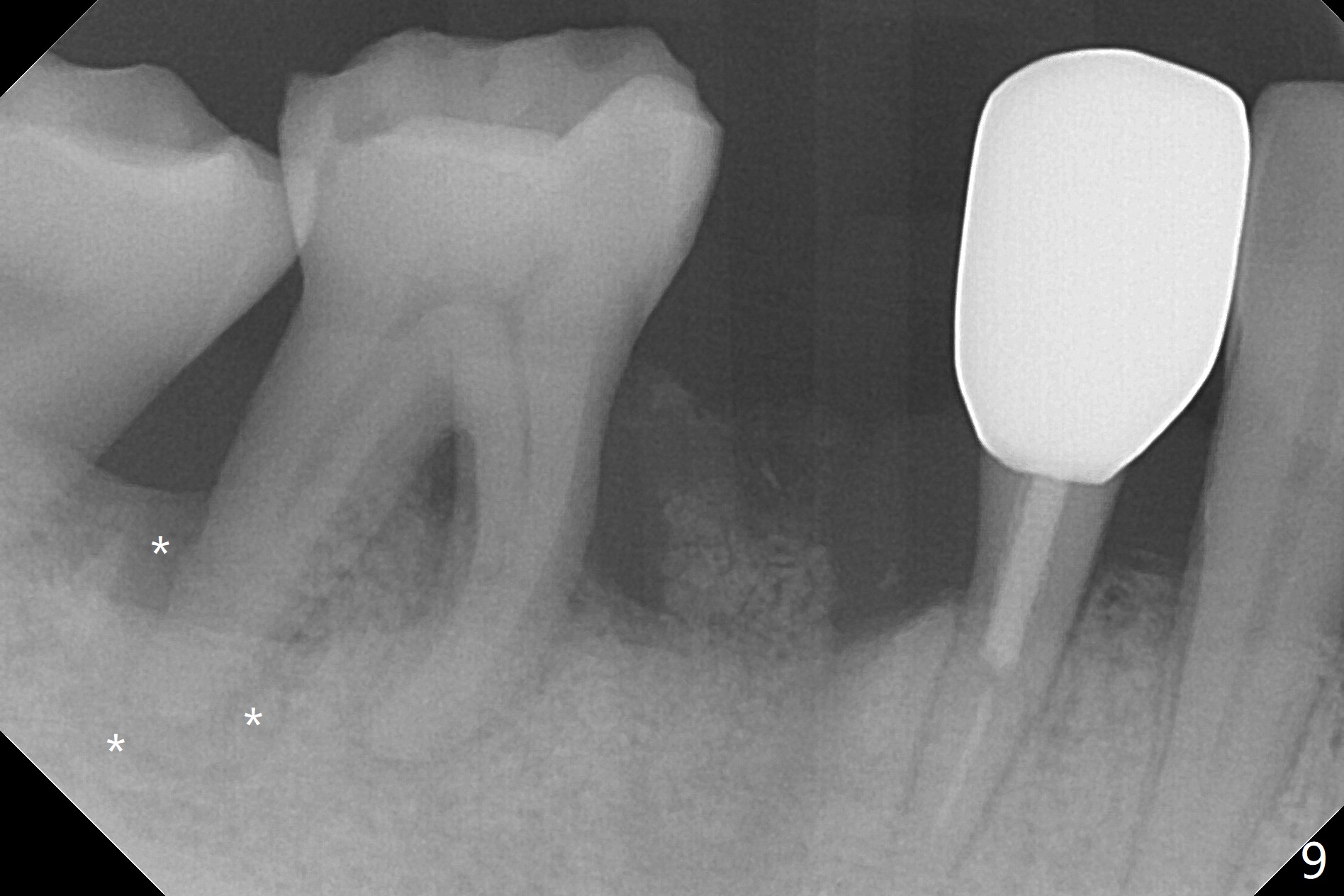
The tooth #29 is easily extracted with granulation tissue attached to the apex (Fig.1,2). The buccal plate is low. Initial osteotomy is established in the mesial slope of the socket for 13 mm subgingival (Fig.3 red dashed line). After adjustment of the osteotomy position and use of Magic Drills 2.8 and 3.3 mm for 15 mm subgingival, a 4x9 mm dummy implant is placed 2 mm subgingival (Fig.4). Final implant (Fig.5: 4x9 mm; red dashed line: socket) is placed 4 mm subgingival (supracrestal buccal; infracrestal lingual); Vanilla graft placed buccodistal (*). With placement of a 4.5x5.7(4) mm abutment (Fig.5), an infraocclusal immediate provisional (Fig.6 P) is fabricated to maintain the interdental papillae. One month later, the abutment dislodges. The patient insists upon no provisional so that he can masticate on the right side, since there is no functional molars on the left side. The implant appears to have osteointegrated 5 months postop (Fig7). The crown is loose 2.5 months post cementation (8.5 months postop); there is bone loss around the implant (Fig.8 *). Vanilla graft is placed after implant removal (Fig.9); in fact the neighboring teeth also have mobility (including periapical radiolucency at #30 (Fig.9 *)).
Return to Lower Premolar Immediate Implant, Armaments Xin Wei, DDS, PhD, MS 1st edition 01/11/2018, last revision 09/27/2018