
|
|
|
|
|
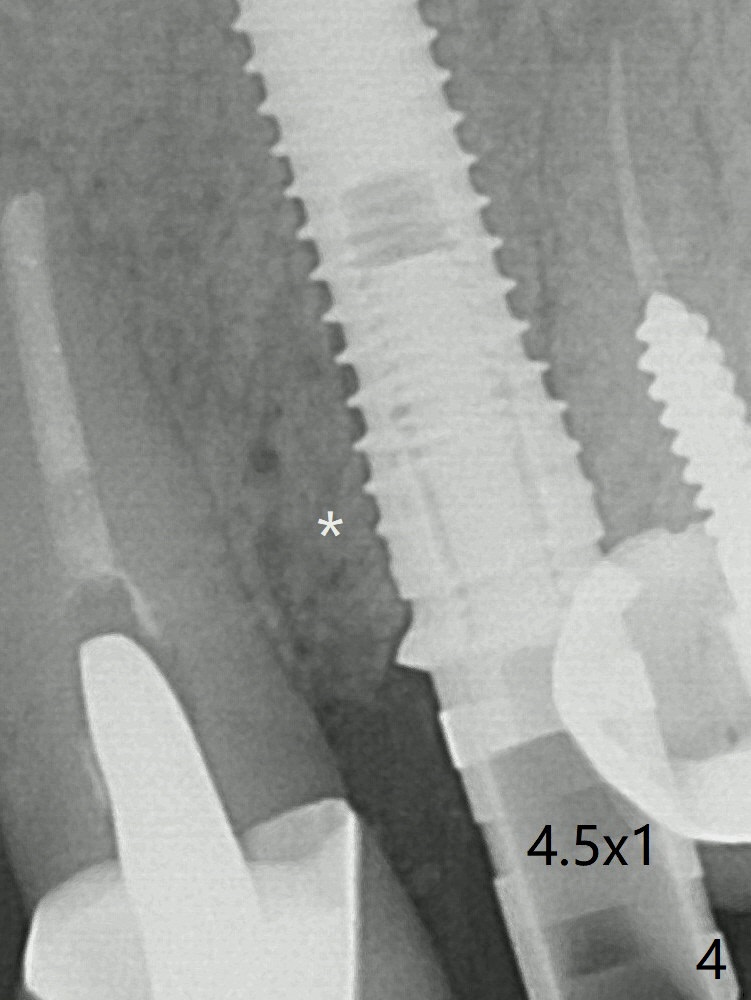
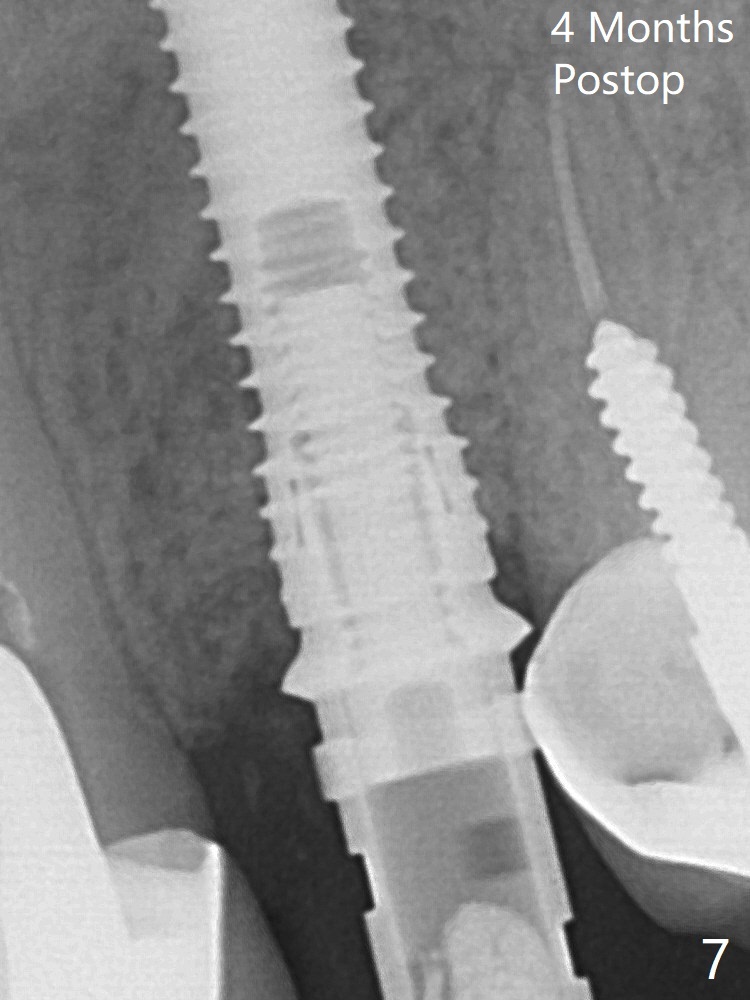
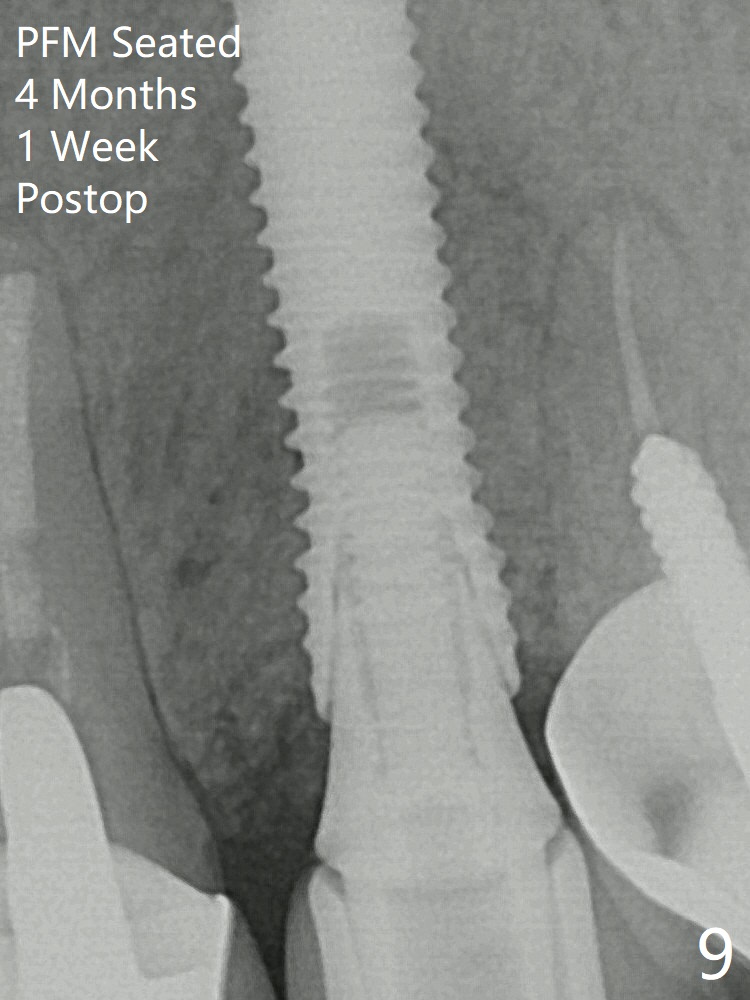
In spite of severe apical infection (Fig1,2 *), a thin narrow strip of the buccal plate (arrowheads, corresponding to the keratinized gingiva) is present when the tooth #11 is extracted. The thin bone keeps the bulging alveolus, i.e., reservoir for bone graft (Vanilla/Osteogen Fig.4 *) after placement of a 3.8x16 mm implant (Fig.3,4). A 4.5x1 mm temporary abutment, placed and trimmed for an immediate provisional, seems to be short in cuff. When an implant is placed deep to prevent periimplantitis, the cuff should be longer, i.e., 3 mm. X-ray should be taken for the depth confirmation after temporary abutment placement. Fig.3: a 2 mm drill in place, 18 mm in bone vs. 16 mm of implant placed ~ 2 mm subcrestal (Fig.4). A narrow implant (3.8 mm) is chosen over 4.5 mm because of the extensive buccal plate defect. While the hard tissue around the implant seems to be healthy 5 months postop (Fig.7), the soft tissue is not (Fig.8). Indeed PFM helps shade match in this case as well (Fig.9,10). Switching abutments (from temporary to cemented) makes it difficult to seat the crown. Post cementation X-ray leaves record for future contact loosening. The buccal gingiva remains erythematous associated with open margin (Fig.11 >) 1 year 4 months post cementation.
Temporary Abutment Last Next Xin Wei, DDS, PhD, MS 1st edition 12/21/2019, last revision 05/26/2020